
Abstract
Objective:
To describe urinary tract infections (UTIs) after robot-assisted radical cystectomy (RARC) and investigate the variables associated with it.
Materials and Methods:
A retrospective review of 616 patients who underwent RARC between 2005 and 2019 was performed. Patients were divided into those who developed UTI and those who did not. Patients who developed UTI were further subdivided into three subgroups according to the onset, number, and severity. The Kaplan–Meier method was used to depict time to UTI. Multivariate analysis was used to investigate variables associated with UTI.
Result:
Two hundred forty (39%) patients were diagnosed with UTI after RARC; 48% occurred within 30 days, 17% within 30–90 days, and 35% at 90 days after RARC. Twenty-three percent of the patients presented with urosepsis. The median (interquartile ratio) time to develop UTI was 1 (0.3–7) month. On multivariate analysis, patients who received neobladders (odds ratio [OR] 2.80; 95% confidence interval [CI] 1.50–5.20; p < 0.01), prolonged hospital stay (OR 1.06; 95% CI 1.03–1.08; p < 0.01), adjuvant chemotherapy (OR 2.20; 95% CI 1.40–3.60; p < 0.01), poor renal function postoperatively (OR 2.30; 95% CI 1.30–3.80; p < 0.01), postoperative hydronephrosis (OR 2.50; 95% CI 1.40–4.50; p < 0.01), ureteroileal anastomotic stricture (OR 2.90; 95% CI 1.50–5.70; p < 0.01), and stented ureteroileal anastomosis (OR 9.35; 95% CI 1.23–71.19; p = 0.03) were associated with UTI after RARC.
Conclusion:
UTI is common after RARC mainly within the first month after RARC. Enterococcus faecalis was the most common causative organism.
Introduction
Radical cystectomy (RC) with urinary diversion is the standard of care for muscle-invasive and high-risk, or refractory, nonmuscle-invasive bladder cancers. 1 Robot-assisted radical cystectomy (RARC) has emerged as an alternative to the conventional open approach with comparable oncologic outcomes. 2 Whatever the surgical approach, RC remains a morbid procedure. 3
Urinary tract infections (UTIs) contribute significantly to the morbidity associated with RC. 4 UTI occurs in up to 39% of patients after RC, with one-third of them occurring within the first 3 months after surgery. 5 The use of bowel segments for construction of urinary diversion is a major risk factor for UTI, with Escherichia coli as the most commonly isolated organism in urine cultures and less commonly skin flora in patients with ileal conduit or catheterizable pouches. 6 Nevertheless, prior studies lacked standardized criteria for what constitutes UTI, and many of them included patients with asymptomatic bacteriuria. 7,8 UTIs represent a major cause of readmissions after RARC, especially within the first month after surgery.
It is still controversial whether antibiotic prophylaxis after surgery is needed or not. A recent study showed that the use of prophylactic antibiotics in the first 30 days following RC significantly decreases UTIs and readmissions from urosepsis after surgery. 9 In this context, we sought to report a detailed analysis of UTIs after RARC and better characterize variables that affect UTIs after RARC.
Materials and Methods
We retrospectively reviewed our prospectively maintained institutional database of 616 RARCs for bladder cancer performed by two surgeons (K.A.G.: 592 RARCs between 2005 and 2019, and Q.L.: 24 RARCs between 2018 and 2019) (I-79606). All patients received one dose of prophylactic ertapenem 1 g at induction of anesthesia (levofloxacin 500 mg or clindamycin 900 mg in allergic patients) before RARC. Techniques for RARC, ileal conduit, and neobladder have been previously described. 10,11 Twenty-four patients did not have ureteral stents based on surgeon discretion. No prophylactic antibiotics were given at discharge or at the day of stent removal. Ureteral stents were generally removed on postoperative day 14 for patients who underwent ileal conduit. For those who received neobladders, stents were usually sutured to the Foley catheter and removed 3 weeks after RARC (after ensuring no leak on pouchogram). Patients were followed in concordance with the National Comprehensive Cancer Network (NCCN) guidelines. 12 Urine cultures were not routinely obtained unless clinically indicated.
Patients were divided into two groups: those who developed UTIs—defined as the presence of positive urine culture (≥105 cfu/mL with no more than two organisms) and at least one documented symptom, including fever (≥38°C), chills, flank pain, and abdominal pain—and those who did not. 13 Asymptomatic patients with positive urine culture were not considered UTI. All urine samples were collected by catheter insertion into the ileal conduit or neobladder. The UTI group was further classified according to the onset of the first UTI (within 30 days vs 31–90 days vs >90 days after RARC), number of UTIs (single vs multiple), and severity. Severe UTIs included urosepsis, which was defined in accordance with the 2001 International Sepsis Definition Conference as UTI in the presence of two or more of the following criteria: body temperature ≥38°C or ≤36°C; tachycardia ≥90 beats per minute; tachypnea ≥20 breaths per minute; respiratory alkalosis PaCO2 ≤ 32 mmHg; and leukocytes ≥12,000/μL or ≤4000/μL or >10% band forms. 14 Of note, diagnosis of ureteroileal strictures was based on loopograms and/or antegrade nephrostograms.
Data were reviewed for demographics, perioperative variables, onset, number, and causative organism and antibiotic sensitivity. The incidence of UTIs per year was depicted and the Cochran–Armitage test was utilized to determine if there was a significant trend. Pearson's chi-square and Fisher's exact tests were used to examine the association between categorical variables. Mean ± standard deviation and median with interquartile ratio (IQR) were used to describe continuous variables. The Kaplan–Meier method was used to depict time to first UTI. Multivariate stepwise logistic regression models were used to investigate variables associated with any UTI and multiple UTIs. All values reported are two-sided with p ≤ 0.05 considered statistically significant. All analyses were performed using statistical software analysis package SAS, version 9.4 (SAS Institute, Inc., Cary, NC).
Results
Six hundred sixteen patients underwent RARC with a median follow-up of 24 months (IQR 7–60). Two hundred forty patients (39%) were diagnosed with UTI after a median of 1 month (IQR 0.3–7 months) after RARC. Incidence of UTI did not significantly change over time (p = 0.09) (Supplementary Fig. S1). Patients who developed UTIs were younger (69 vs 71 years; p = 0.02), received neobladder more frequently (15% vs 6%; p < 0.01), had pN+ more frequently (29% vs 20%, p < 0.01), suffered more overall (85% vs 70%, p < 0.01), had high-grade complications (36% vs 18%; p < 0.01), and were readmitted more frequently (36% vs 22%; p < 0.01). They had longer median inpatient stay (8 vs 7 days; p < 0.01) and received adjuvant chemotherapy more frequently (24% vs 13%; p < 0.01). They developed postoperative hydronephrosis (21% vs 6%; p < 0.01), postoperative poor renal function (eGFR <60 mL/min) (22% vs 8%; p < 0.01), and ureteroileal strictures (15% vs 5%; p < 0.01) more frequently. Patients who underwent stented ureteroileal anastomosis developed UTIs more frequently compared with those who received stentless anastomosis (40% vs 4%, p < 0.01) (Table 1).
Patient Demographics, Clinical, and Perioperative Characteristics
Boldface indicates statistical significance.
ASA = American Society of Anesthesiologists; BMI = body mass index; eGFR = estimated glomerular filtration rate; ICU = intensive care unit; IQR = interquartile ratio; RARC = robot-assisted radical cystectomy; SD = standard deviation; UTI = urinary tract infection.
Forty-eight percent of UTIs occurred within 30 days after RARC, while 17% and 35% occurred 30–90 and >90 days after RARC, respectively (Supplementary Table S1). UTI-free probability was 64%, 59%, and 55% at 1, 2, and 3 years, respectively (Fig. 1). Enterococcus faecalis was the most common causative organism, followed by E. coli and then Klebsiella pneumoniae. The highest antibiotic resistance was observed for penicillins and fluoroquinolones, while the highest sensitivity was observed for aminoglycosides, trimethoprim/sulfamethoxazole, and cefepime (Figs. 2 and 3). The fungal infections represented 30% of UTIs that occurred within the first 30 days after RARC, 13% of those that occurred 30–90 days, and 22% of those that occurred 90 days after RARC.
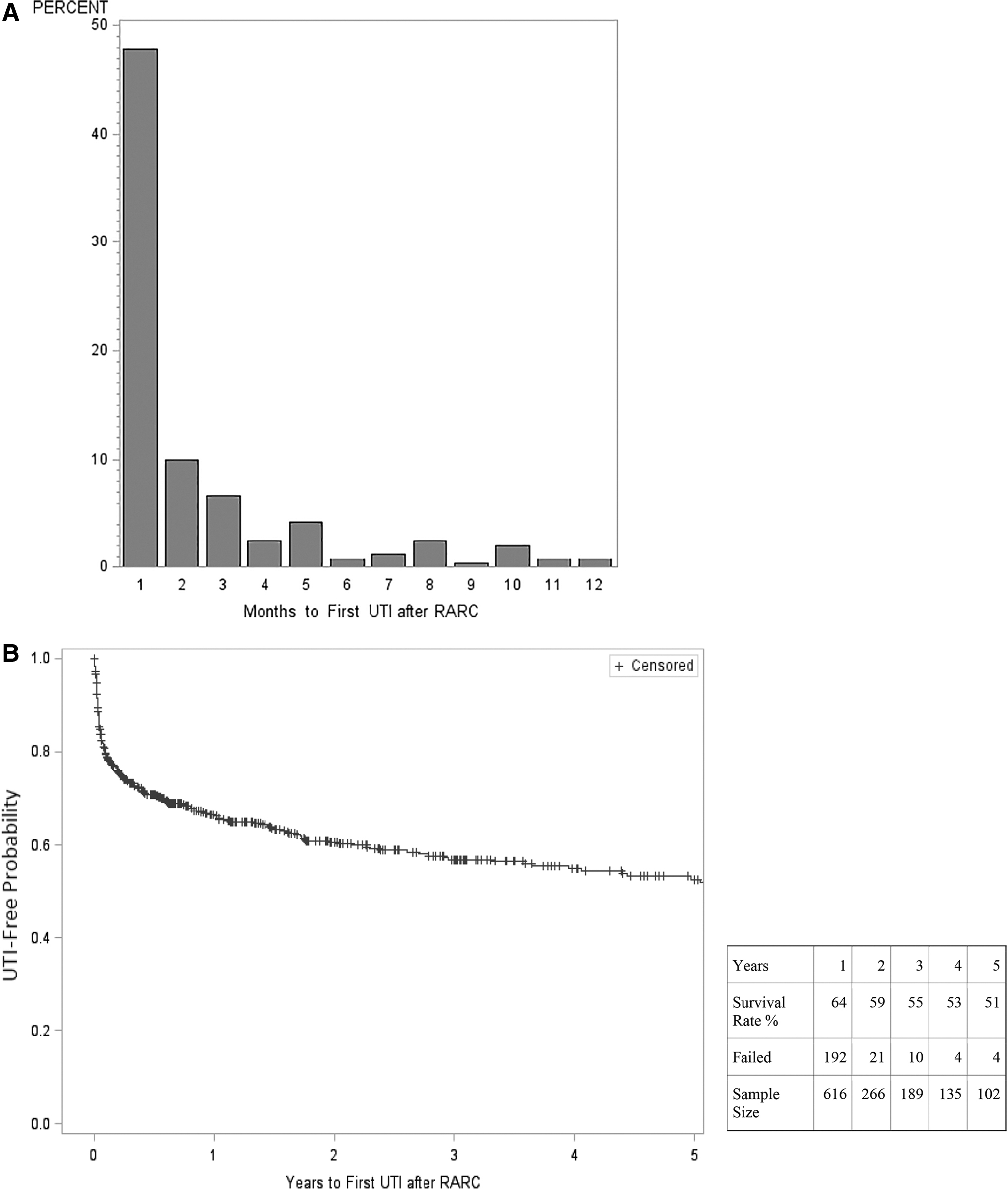
Time to first UTI and UTI-free survival. RARC = robot-assisted radical cystectomy; UTI = urinary tract infection.
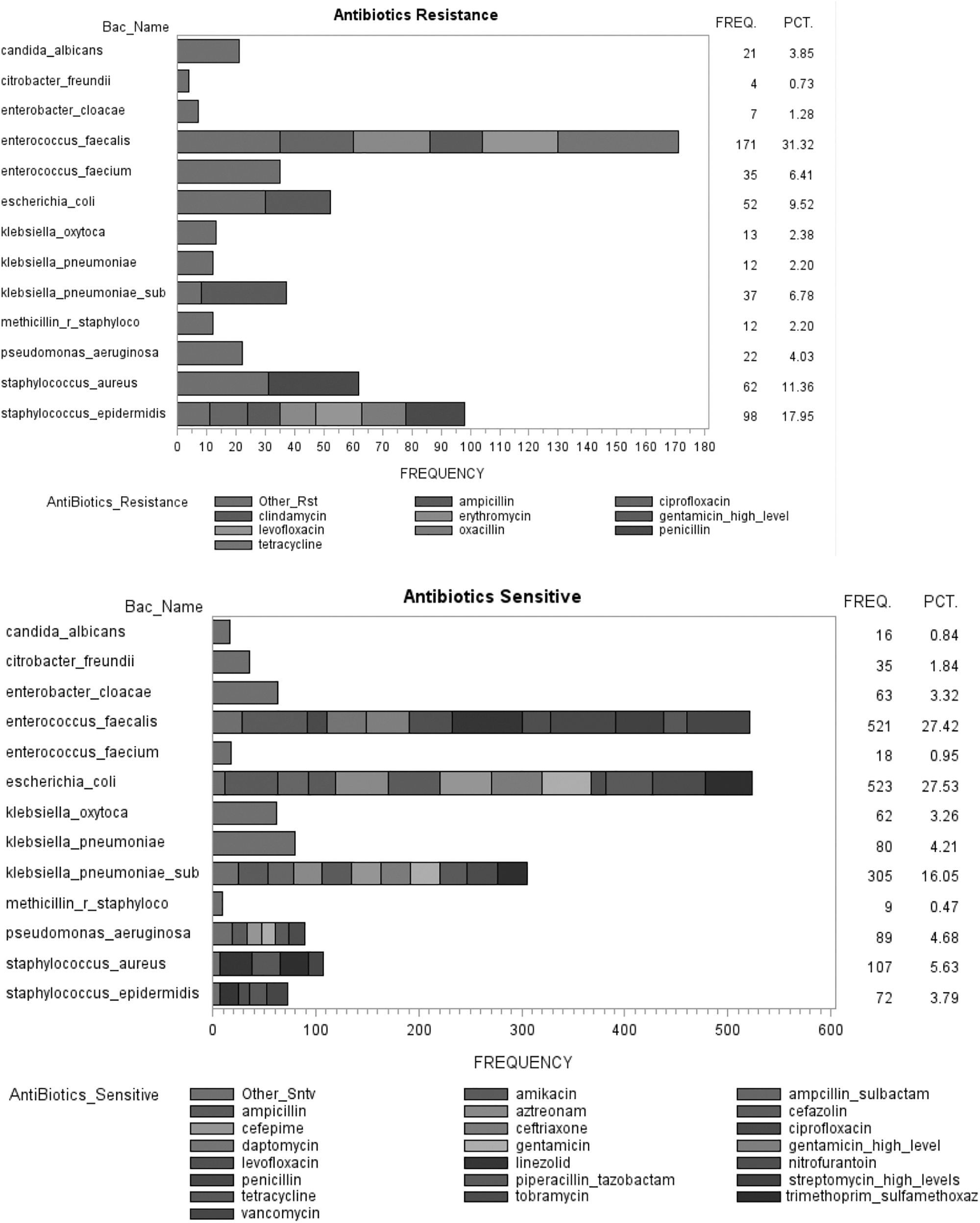
Antibiotic sensitivity and resistance.
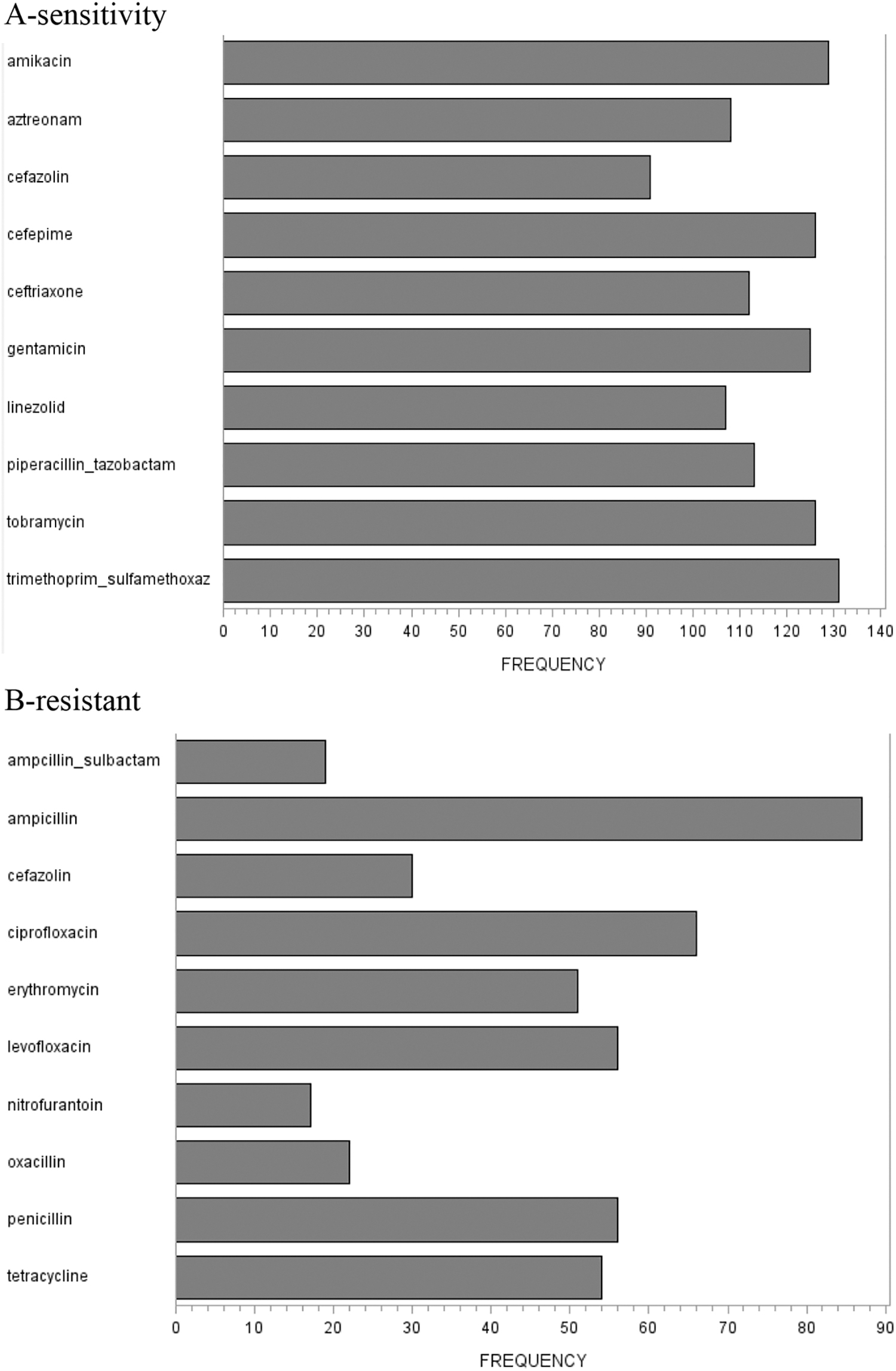
The frequency of overall antibiotic sensitivity and resistance.
Among those who developed UTI after RARC, 125 patients (52%) developed recurrent UTIs (>1 episode). These patients demonstrated postoperative hydronephrosis (27% vs 15%; p = 0.03) and ureteroileal strictures (20% vs 10%; p = 0.03) more frequently compared with those who had a single episode of UTI. They developed urosepsis more frequently (17% vs 6%; p < 0.01) and had earlier median time to first UTI (24 vs 69 days after RARC; p < 0.01) (Supplementary Table S2).
Almost a quarter of the patients presented with severe UTIs. These patients were more likely to have perioperative renal failure (40% vs 17%, p = 0.01), shorter time to first UTI (18 days vs 39 days, p = 0.01), and more frequent episodes (2 vs 1, p = 0.01) (Supplementary Table S3).
On multivariate analysis, neobladder (odds ratio [OR] 2.80; 95% confidence interval [CI] 1.50–5.20; p < 0.01), longer hospital stay (OR 1.06; 95% CI 1.03–1.08; p < 0.01), adjuvant chemotherapy (OR 2.20; 95% CI 1.40–3.60; p < 0.01), postoperative poor renal function (eGFR <60 mL/min) (OR 2.30; 95% CI 1.30–3.80; p < 0.01), postoperative hydronephrosis (OR 2.50; 95% CI 1.40–4.50; p < 0.01), stented ureteroileal anastomosis (OR 9.35; 95% CI 1.23–71.19; p = 0.03), and ureteroileal anastomotic stricture (OR 2.90; 95% CI 1.50–5.70; p < 0.01) were significantly associated with developing UTIs after RARC (Table 2). Moreover, age (OR 0.96; 95% CI 0.94–0.98; p < 0.01), female gender (OR 1.80; 95% CI 1.10–2.80; p = 0.02), longer hospital stay (OR 1.10; 95% CI 1.03–1.08; p < 0.01), adjuvant chemotherapy (OR 1.70; 95% CI 1.01–2.90; p = 0.04), postoperative poor renal function (OR 2.20; 95% CI 1.30–3.90; p < 0.01), postoperative hydronephrosis (OR 2.60; 95% CI 1.50–4.70; p < 0.01), and ureteroileal anastomotic stricture (OR 3.20; 95% CI 1.70–6.20; p < 0.01) were significantly associated with developing recurrent UTIs.
Multivariate Logistic Regression Analyses to Estimate the Risk Factors for Any Urinary Tract Infection and Recurrent Urinary Tract Infections After Robot-Assisted Radical Cystectomy
Discussion
UTIs are among the most common early complications after RARC. The prevalence of clinically significant infection is relatively lower and varies widely among studies. 15 Prior reports were limited by the lack of standardized definition for UTI, where many included asymptomatic bacteriuria as well.
We report overall a UTI rate of 39% after RARC, almost half of them occurred in the first month after surgery, 17% within 30–90 days, and 35% beyond 3 months after RARC. Twenty-three percent presented with urosepsis. Mano R. et al. reported a 33% symptomatic UTI rate within 90 days following RC, 10% at 3–6 months, and 8% at 6–12 months among patients who underwent RC and neobladder. 16 Clifford et al. reported a UTI rate of 11% within 90 days after RC. In the current study, 35% of UTIs occurred 3 months or more after RARC. While this finding highlights the importance of an extended follow-up, reporting UTIs up to 90 days only after RC may underestimate the actual burden of this common complication.
Patients who received neobladders were almost three times more likely to develop UTIs compared with ileal conduits in the current study. Parker et al. reported higher 90-day UTIs in patients with continent diversion. 17 Similarly, van Hemelrijck et al. found a higher rate of UTI in orthotopic neobladder compared with ileal conduits in a review of 7608 patients following RC in Sweden. 18 The higher incidence of UTIs among neobladders can be explained by the high postvoid residual urine in some patients with continent diversion, as well as the need for clean intermittent catheterization and higher rates of stone formation due to urine stasis; however, clear evidence is lacking. On the contrary, Clifford et al. and Al Hussein Al Awamlh et al. found no association between the type of diversion and postoperative UTIs. 19,20
Prolonged hospital stay was an independent risk factor for UTIs after RARC in our cohort. Longer inpatient stay can lead to hospital-acquired infections, including UTIs. Mitchell et al. found that 2% of patients who were hospitalized for more than 2 days acquired a hospital-related UTI. 21 Hospital-acquired UTIs can be further predisposed by the presence of foreign bodies such as stents or urethral catheter, old age, extended antibiotic treatment, and patient general health status. 22,23
Postoperative hydronephrosis was found to be associated with UTI. It is usually caused by obstruction (such as ureteral stricture) or urine reflux after RARC; both can lead to urine stasis and subsequently UTI. Kaczmarek et al. found no association between the preoperative hydronephrosis and UTI rate after RC. Preoperative hydronephrosis may be relieved after surgery due to removal of the obstructing tumor. 24 Ureteroileal anastomotic strictures were significantly associated with UTIs. Most of the ureteroileal strictures are asymptomatic in their earlier course and many present with UTI. 25 Ureteroileal strictures can lead to urine stasis and deterioration of renal function, which also explains the association with poor renal function. We found that ureteroileal anastomotic strictures were associated with UTI incidence and number of episodes of UTI after RARC. Follow-up after RARC should include surveillance for upper tracts. If there is any suspicion of upper tract deterioration (recurrent UTIs, flank pain, deterioration of kidney functions, etc.), further workup as well as intervention to relieve the obstruction should be undertaken.
We found that recurrent UTIs were associated with same variables as any UTI in addition to age and gender. The association between younger age and recurrent UTIs could be explained by the fact that neobladder, which is associated with recurrent UTIs, is usually offered for younger patients. Also, younger patients usually have a longer life expectancy, and therefore, they are more likely to live longer and develop other complications such as strictures that are associated with UTIs. 17 The female gender is a well-known risk factor for UTI in the general population; young sexually active women have ∼0.5 episodes of acute cystitis/year. 26 In case of neobladder diversion in women, short urethra and its proximity to the perineal area most likely play a major role for recurrent UTI occurrence. Factors such as malnutrition and adjuvant chemotherapy after RC may weaken the immune system and thereby facilitate the presence of recurrent UTIs. 9
In our cohort, the most common overall causative organisms were E. faecalis, followed by E. coli and then K. pneumoniae. Enterococcus was found to be highly resistant to macrolides and fluoroquinolones, while E. coli and K. pneumoniae were resistant primarily to penicillins. These results can help with the choice of appropriate empiric antibiotics for prophylaxis after RARC or in case of active UTI before urine culture results. Based on our antimicrobial sensitivity pattern, TMP, nitrofurantoin, and ampicillin/sulbactam seem attractive options for antibiotic prophylaxis in high-risk patients for UTIs, although antibiotic sensitivities may differ between different institutions. Clifford et al. reported similar causative organisms and aminoglycoside sensitivity range for patients who underwent open RC (91%) and RARC (9%). 19 Parker et al. similarly found high rates of Enterococcus and E. coli as well as Staphylococcus aureus and Pseudomonas aeruginosa. 17 It is notable that within the first 30 days after RARC, we found that fungal infections were the second-most common causative organism after E. faecalis. The presence of foreign bodies such as the Foley catheter, drains, or ureteral stent in the first 2–3 weeks after the surgery may allow for such fungal (opportunistic) infections. 27 Fungal cultures should be always considered, especially in the case of lack of clinical response to antibiotic treatment, particularly in the first month after RARC.
Routine cultures from stents were previously suggested by some groups. Despite the fact that the incidence of stent colonization exceeds 90%, a minority of patients with positive stent cultures develop symptomatic UTIs, the incidence of which increased when indwelling time exceeded 90 days. 28 In our study, stents were generally removed after 2 weeks in patients who received ileal conduits or after 3 weeks in those who received neobladders. The effect of ureteroileal stenting on UTIs after RC remains controversial. 29 In the current study, ureteroileal stenting was nine times more likely to develop UTIs compared with stentless procedures. However, the small number of patients who received stentless ureteroileal anastomosis and the extremely wide CI make it hard to draw any conclusions.
Patients who developed UTIs suffered from more overall and high-grade complications and readmissions. Also, a quarter of these patients had urosepsis. Our study highlights the importance of UTI and its significant impact on the health care burden and the added costs. Thus, studies have investigated the role of prophylactic antibiotics after RARC. A prospective study was initiated as a quality measure to decrease the rate of UTIs after RC. Antibiotic prophylaxis was started and compared with a cohort of patients before implementing antibiotic prophylaxis. Antibiotic prophylaxis resulted in a decrease in the rate of UTIs from 36% to 12% (p < 0.004) and a decrease in the rate of readmissions from 17% to 2% (p = 0.02). Thirty percent of patients who did not receive antibiotic prophylaxis developed UTI 1 day after ureteral stent removal, while none had a UTI after implementing antibiotic prophylaxis. 9 These results suggested a benefit for prophylactic antibiotics after RC; however, a randomized-controlled trial is still needed.
To our knowledge, this study is the first study that described UTIs after RARC. However, some limitations exist. First, the retrospective study design has known limitations. Second, despite us reporting the majority of complications and readmissions even if we were outside our institution, there is still a possibility of underreporting. Third, the robotic approach seems to have no impact on the rate of UTI generally. However, we cannot really discern this relationship due to the lack of an open arm. Fourth, our causative organisms and antimicrobial sensitivity pattern may not be generalized to other institutions. Fifth, ureteral stents were removed 2 or 3 weeks in ileal conduit or neobladder urinary diversion after RARC, respectively, in the majority of our patients; however, the precise time of removal is not captured in our database. Finally, only a few patients did not have stents, making it difficult to discern the effect of stenting the ureteroileal anastomosis on UTIs.
Conclusion
UTI is a common cause of complications and readmissions following RARC and urinary diversion, mostly within the first month after surgery. Suppressive prophylactic antibiotics might help patients who are receiving neobladder diversion, have prolonged hospital stay, are receiving adjuvant therapy, have postoperative hydronephrosis, have postoperative poor renal function, or are diagnosed with ureteroileal anastomotic stricture to decrease the rate of UTIs after RARC.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.
Supplementary Material
Supplementary Figure S1
Supplementary Table S1
Supplementary Table S2
Supplementary Table S3
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.