
Abstract
Introduction:
Closed drains have traditionally been placed after partial nephrectomy because of risks of bleeding and urine leak. We sought to study the safety of a nonroutine drain (NRD) approach after transperitoneal robotic partial nephrectomy (RPN).
Patients and Methods:
From a multi-institutional database, we have analyzed the data of 904 patients who underwent RPN. Five hundred forty-six (60.40%) patients underwent RPN by a surgeon who routinely placed drains. Three hundred fifty-eight (39.60%) patients underwent RPN by a surgeon who did not routinely placed drains. Perioperative outcomes, length of stay (LOS), and readmission rates were compared between the two groups. Baseline characteristics, perioperative, and postoperative outcomes were compared using Mann–Whitney U test, chi-square test, and Fisher's exact test.
Results:
Patients in the NRD group were more likely to have higher body mass index (30.10 kg/m2 vs 28.07 kg/m2; P < 0.001), higher tumor size (3.0 cm vs 2.5 cm; P = 0.001), and higher renal score (8 vs 7; P < 0.001). Rate of transfusion (0.00% NRD vs 0.56% RD; P = 0.157) and overall complication (7.33% NRD vs 7.82% RD; P = 0.782) were comparable. Median hospital stay is 1 day for both groups. Readmission rate was also similar (0.55% NRD vs 1.40% RD; P = 0.279). In a multivariable analysis, NRD approach was associated with shorter length of hospital stay (incidence rate ratio [IRR] – 0.72, P < 0.001).
Conclusion:
An NRD approach for RPN yielded a decreased LOS and similar perioperative outcomes. Placement of surgical drains should be based on individual circumstances, and not required on a routine basis.
Introduction
According to the guidelines, the reference standard treatment for localized renal masses is partial nephrectomy. 1 In the past decade, the robotic approach has become common to perform partial nephrectomy with comparable oncologic and functional outcome compared with open surgery. 2 Despite the promising perioperative outcome, known complications remain, including bleeding, hematoma, urine leak, and urinoma. 3 Traditionally, intraoperative drain has been placed routinely to diagnose these complications early or prevent fluid collections. However, these complications are relatively uncommon and it is unclear whether drain placement prevents perioperative complications and decrease readmissions.
For this reason, routine drain (RD) placement has been challenged in the urologic literature previously, with available randomized clinical trial data in the setting of robotic radical prostatectomy. These trials provided level one evidence regarding the safety of omitting drain placement postrobotic radical prostatectomy. 4,5 Although there are data on open partial nephrectomy, data are limited for robotic partial nephrectomy (RPN). 6,7 In this study, we sought to demonstrate the safety and efficacy of a nonroutine drain (NRD) approach by comparing with an RD approach using a large multi-institutional database.
Materials and Methods
Patients and data source
We used an institutional review board-approved multi-institutional kidney cancer database of patients who have undergone robot-assisted partial nephrectomy for analysis. We identified patients with complete data available on baseline and tumor characteristics, intraoperative and perioperative complications, and drain placement. All patients underwent transperitoneal RPN. All cases were performed between February 2008 and September 2019. Patients with polycystic kidney disease, multiple tumors, bilateral tumors, and solitary kidney were excluded from the analysis. Overall, 904 patients remained for further analysis-RD, n = 546 (60.40%) and NRD, n = 358 (39.60%).
Drain groups
Four surgeons placed drains routinely, two surgeons did not place drain routinely. One surgeon switched to an NRD approach over time and, therefore, had cases in both groups. Patients in NRD group had drains placed only in specific conditions at the surgeon's discretion such as highly complex excisions, sinus fat invasion, large renorrhaphy defects or anticoagulant use. Overall, 31 patients (8.68%) in NRD group had drain placed at the end of surgery. They were analyzed within the NRD group as an intent to treat analysis.
Outcome
The main outcomes of interest were perioperative outcomes, including postoperative complication rates (any, major, and surgical), postoperative length of stay (LOS), and readmission rates. Complications were stratified according to Clavien–Dindo classification. Major complication is described as Clavien ≥3. 8
Variables
Between the two groups, baseline demographic and tumor-specific covariates were compared, including age, gender, body mass index (BMI), Charlson comorbidity index (CCI), 9 hypertension, diabetes mellitus, baseline estimated glomerular filtration rate, baseline chronic kidney disease stage, tumor size, hilar tumor, and RENAL nephrometry score. 10
Statistical analysis
Continuous variables were presented as medians, interquartile ranges, and ranges, whereas categorical variables were presented as counts and frequencies. Baseline demographic, clinical, tumor-specific characteristics, as well as postoperative complication rates (any, major, and surgical), postoperative LOS, and readmission rates were compared using Median test, Mann–Whitney U test, chi-square test of independence, and Fisher's exact test. A negative binomial regression was used to evaluate the relationship between LOS and drain use, controlling for all baseline characteristics. Statistical significance was determined at P-value <0.05, and all analyses was conducted using STATA Version 14.1 (College Station, TX).
Results
Baseline characteristics
Patients in the NRD group were more likely to have higher BMI (30.10 kg/m2 vs 28.07 kg/m2; P < 0.001), higher tumor size (3.0 cm vs 2.5 cm; P = 0.001), higher renal score (8 vs 7; P < 0.001), and higher American society of Anesthesiologist (ASA) score (Score 1, 1.25%; Score 2, 45.05%; Score 3, 52.01%; Score 4, 1.65%; P = 0.005). Age (P = 0.618), gender (P = 0.935), CCI (P = 0.370), hilar tumor (P = 0.697), and clinical stage (P = 0.638) were not significantly different between the nondrain and drain groups (Table 1).
Baseline Characteristics
Presented as median (interquartile range; range) and analyzed using Mann–Whitney U test or aMedian test.
Categorical variables are presented as count (frequency) and analyzed using chi-square test and Fisher's exact test
Values in bold are significant at P < 0.05.
ASA = American society of Anesthesiologist; BMI = body mass index; CCI = Charlson comorbidity index; kg/m2 = kilogram per meter square.
Perioperative outcomes
In Table 2, patients in the NRD group were more likely to have a higher EBL (100 mL vs drain, 50 mL; P < 0.001); however, transfusion rate was similar between the two groups (0.00% NRD vs 0.56% RD; P = 0.157). Although the median hospital stay is 1 day for both groups, the maximum length of hospital stay in the NRD group was 6 days and the RD group was 9 days; hence, the mean rank difference in length of hospital stay was significantly different (P < 0.001).
Perioperative and Postoperative Complications
Presented as median (interquartile range; range) and analyzed using Mann–Whitney U test.
Categorical variables are presented as count (frequency) and analyzed using chi-square test and Fisher's exact test.
Values in bold are significant at P < 0.05.
EBL = estimated blood loss; LOS = length of stay.
Complication rates, LOS, and rate of readmission
The rate of overall complication (7.33% NRD vs 7.82% RD; P = 0.782), major complication (1.83% NRD vs 2.23% RD; P = 0.671), and surgical complication (4.76% NRD vs 4.19% RD; P = 0.686) were not different between the groups. Similarly, readmission rate was also not significantly different (0.55% NRD vs 1.40% RD; P = 0.279). Types of surgical and major complications are summarized in Tables 3 and 4.
Surgical Complications Among the Nonroutine Drain Group
Major Complications Among the Nonroutine Drain Group
In the multivariable negative binomial regression model (Table 5), controlling for age, BMI, ASA score, CCI, tumor size, hilar tumor, RENAL score and clinical stage, NRD approach was associated with shorter length of hospital stay (incidence rate ratio [IRR] −0.74, 95% confidence interval [CI] −0.66 to 0.84; P < 0.001). ASA score of 4 (IRR −2.42, 95% CI −1.30 to 4.47; P = 0.005) and hilar tumor (IRR −1.19, 95% CI −1.02 to 1.38; P = 0.027) were more likely be to associated with a longer hospital stay. The distribution of length of stay is shown in Figure 1. Age, gender, BMI, CCI, tumor size, renal score, and clinical stage were not associated with length of hospital stay.
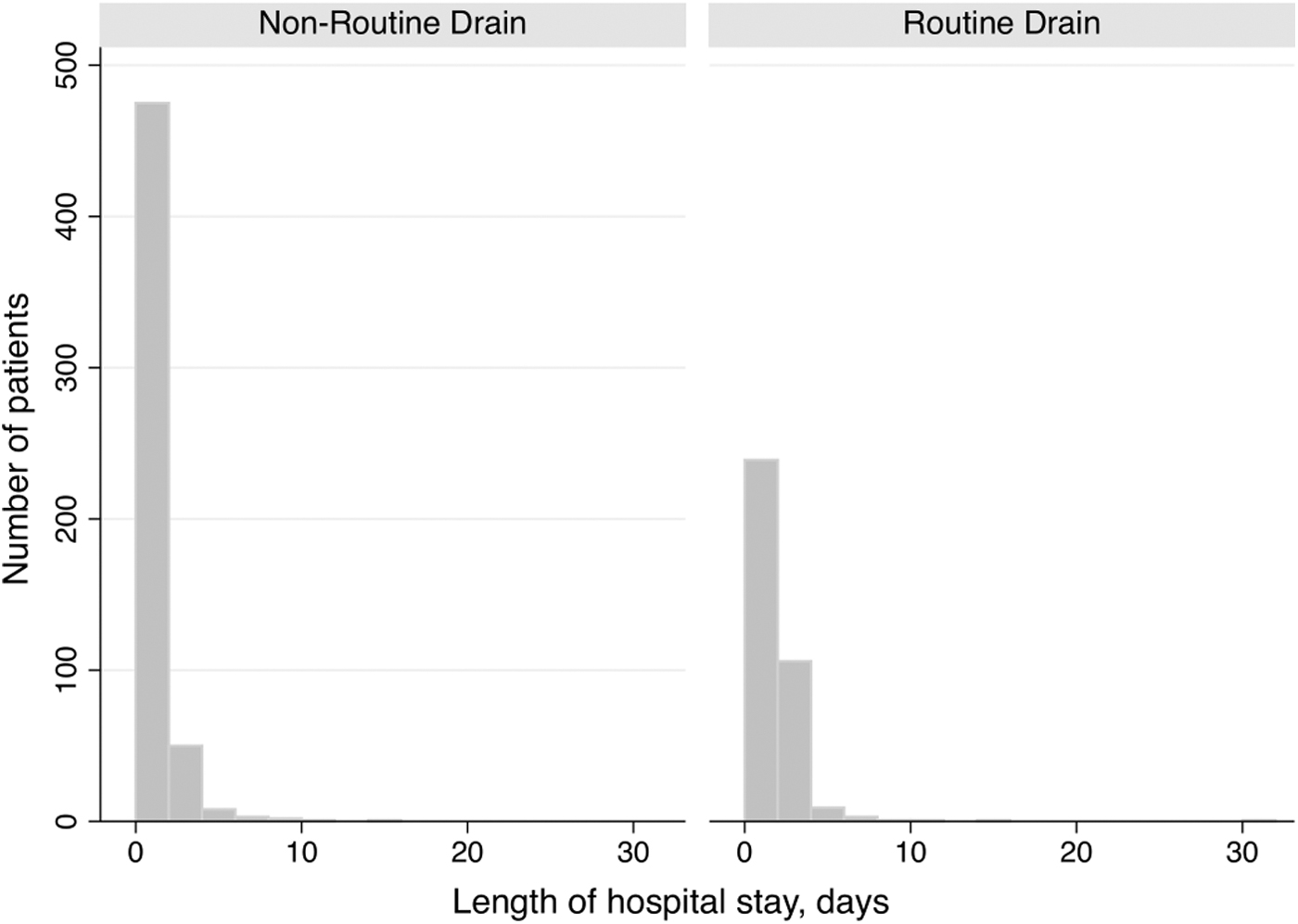
The distribution of length of hospital stay by drain use.
Relationship Between Length of Hospital Stay and Drain Groups
Values in bold are significant at P < 0.05.
CI = confidence interval; IRR = incidence rate ratio.
Discussion
Our results showed similar perioperative outcomes between RD placement and NRD placement. There were baseline differences between the two groups favoring the RD group, including lower BMI (30.10 kg/m2 vs 28.07 kg/m2), smaller tumor size (3.0 cm vs 2.5 cm), lower RENAL score (8 vs 7), and lower ASA score. Despite these statistical differences, the outcome of the NRD group remained comparable. Nonetheless, these differences were adjusted in a multivariate model for the analyses. Perioperative complication and readmission rates were similar between the two groups. However, RD placement was associated with a higher LOS.
Abaza and colleagues previously reported one of the earliest RPN series with a no drain approach. Drain was omitted in 93% of patients. Comparison of drain vs no drain groups revealed similar postoperative complications. 11 However, groups were uneven and the study was limited to a single surgeon series. Peyronnet and colleagues published their multi-institutional series of 636 RPN patients and showed similar complication rate (21.9% vs 20.2%, P = 0.67) and decreased LOS in the no drain group (4.5 vs 5.5 days). 12 Their results were comparable with ours. However, despite the respectable sample size, only 22% of their cohort were in the no drain group. Kahn and colleagues compared 260 consecutive patients with drain vs 100 consecutive patients without a drain. Baseline characteristics were unfavorable in the drain group with higher RENAL score (9 vs 8, P < 0.001) and longer warm ischemia time (21 vs 18 minutes, P = 0.004). After adjusting for baseline differences, they did not see any difference in terms of LOS and (OR: 1.5, P = 0.31) and major complications (OR: 1.49, P = 0.63). 13 Although our results contradict with each other, our study has a substantially larger sample size.
Based on our results and the prior literature review, a solid argument can be made against RD use. Intra-abdominal drains predispose a patient to infections, can increase wound complication risk, 14 and increased pain. 15 Furthermore, the physiologic effects of drain should be considered as well. Tachibana and colleagues reported lower serum total protein and albumin levels in patients who had drain placement. Their results also showed a decreased elevation of neutrophils, lymphocytes, and monocytes in the drain group, which can imply the drainage of these cells through the drain. This could potentially impair the tissue healing process. 16 Finally, the urine leak rate in contemporary RPN series is shown to be <1%. 17 Significant postoperative bleeding is rare 3 and can be monitored with postoperative complete blood count measurement.
The argument for drain includes concern for fluid collection. Most fluid collections are self-limiting and asymptomatic. However, patients may feel discomfort in this period, especially because of retained air that can cause diaphragm irritation and shoulder pain. 18 Since patients are discharged soon after surgery, these minor concerns are not easily documented or analyzed. For this purpose, Tachibana and colleagues performed postoperative CT scan 2–3 days postminimally invasive PN. They have compared the perirenal fluid collection between 148 patients with drain and 46 patients without drain. Perirenal fluid collection was similar (20.3 mL vs 16.8 mL, P = 0.64) despite the average 214 mL fluid drainage in the drain group. 16
Despite these results, we do not imply that drain should be omitted in all cases. In our study, 8.68% patients in the NRD group had drain placed for various surgical reasons such as tumor complexity, large tumor size, and large defect after tumor resection. Furthermore, the comorbidities of the patient may warrant drain placement such as anticoagulant use. Ito and colleagues studied the factors associated with significant bleeding after RPN. Their results demonstrated that anticoagulation was associated with a higher risk of bleeding (OR: 2.19, P = 0.03). However, aspirin was not associated with postoperative bleeding, and increased risk of bleeding was attributed to clopidogrel use. 19 Therefore, the decision on drain placement should be individualized and drain should be considered in patients with higher risk of complications.
Our study is limited by the retrospective design and the inherent selection bias. To limit this bias, we only analyzed the data of surgeons with an RD placement approach or NRD approach. And thus, avoid the bias associated with placing drains in more challenging cases. It should be noted that the surgeons in this study have extensive robotic surgery experience. Therefore, the applicability of these results to low volume, or early practice, surgeons is unclear. A separate study of early practice surgeons is required to validate our results in that setting. In contrast, our results are strengthened by the respectable sample size and the multi-institutional design, which does increase the reproducibility of our results.
Conclusion
An NRD approach yielded a shorter hospital LOS, with similar perioperative outcomes compared with an RD approach. Therefore, RD placement is not required and should be placed on individual patient circumstance. Prospective trials are needed to validate our findings.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.