
Abstract
Background and Purpose:
Drainage of an obstructed kidney due to extrinsic ureteral obstruction (EUO) is imperative. Ureteral stents, commonly employed to facilitate drainage, often fail under EUO; this is usually attributed to external pressure over the ureter that occludes the stent lumen. We showed previously that external pressure and deformation of the ureter, alone, cannot explain frequent stent failure and speculated that colloids present in urine may play a critical synergetic role. In this study, we evaluate the role of colloidal fluid in ureteral obstruction under extrinsic compression.
Materials and Methods:
An in vitro ureter–stent model was employed using a latex tube to simulate a flexible ureter connecting simulated glass kidney and bladder units. The ureter was placed in deformed configuration of 40° with external pressure of 2000 g exerted over the deformed region of the stented ureter, representing extrinsic pressure. Four different ureteral stents were tested—4.8F, 6F, 7F, and 8F. Colloidal solution based on chicken albumin was injected through the simulated kidney into the stented ureter. Four replicates were performed for each stent diameter and straight stented ureters with no external pressure were used as controls. Stent failure was defined as kidney unit pressure over 10 cmH2O or complete obstruction of fluid flow; time to stent failure was measured.
Results:
Average failure time in 4.8F and 6F stents was 44 and 66 hours, respectively. The 7F ureteral stent failed in two replicates, after an average time of 75 hours, and continued to drain in the other two replicates. The 8F and control stents showed no change in kidney unit pressure in any of the replicates.
Conclusions:
Large-diameter stents are more effective in ureteral drainage under EUO in the presence of colloidal material in the fluid. Colloidal fluid may have a role in stent failure under EUO.
Introduction
Extrinsic ureteral obstruction (EUO) is usually caused by pelvic malignancies or metastases leading to hydronephrosis and renal failure. Drainage of the obstructed kidney under such circumstances is imperative to preserve renal function and facilitate chemotherapeutic treatments, and ureteral stents are employed commonly. These ureteral stents often fail, caused by what is usually attributed to external pressure over the ureter occluding the stent lumen.
Indeed, high rates of stent failure (defined as the inability of fluid to pass through a stented ureter) due to EUO have been well recognized decades ago, 1,2 yet little direct investigation of related risk factors has been reported.
Most existing studies of stent failure under EUO have focused on in vitro analysis of the effects of direct mechanical compression on stents and its presumed, potential, or actual role in stent failure. 3 –6 However, as shown by Shilo et al., 7 deformation and compression of the ureter alone, particularly under realistic degrees of compression, cannot generally account for the high incidence of failure of a stented ureter in clinical practice. Rather, we suggested that other factors, particularly the presence of colloids in the urine, may play a critical synergetic role with deformation and compression in stent failure.
Two key points of speculation are raised by Docimo and Dewolf 1 : they suggested (on the basis of analysis of stent properties, patient histories, and stent failure statistics) that stent obstruction/failure due to an EUO is caused by accumulation of debris in the urine, and as a consequence, they suggested that it is preferable to use the maximal stent diameter to reduce the likelihood of stent failure. In the current study, and based on the investigation by Shilo et al., 7,8 we examine these points in a systematic analysis with in vitro experiments. In this study, we use the term “colloid” to denote any type of debris in urine.
We evaluated the efficacy of different ureteral stent diameters under EUO in the presence of colloids. Building on the experimental protocols and insights reported by Shilo et al., 7 we developed an in vitro experimental setup of a stent within a ureter to investigate the effect of colloids on stents that are simultaneously subjected to ureteral deformation and compression.
Materials and Methods
Experimental setup
To examine an EUO, two structural features affecting the stented ureter must be considered, namely deformation and compression. Deformation refers to the overall curvature of the stented ureter caused by the presence of the EUO, while compression represents the potential partial (or full) closure of the stented ureter by reduction in diameter and/or change in (circular) cross section in the direct vicinity of the EUO. Building on the experimental design for the in vitro setup of a single stented ureter subjected to EUO, 7 we developed a system to enable simultaneous experimentation with 12 stented ureter units. We first describe a single in vitro stent–ureter–kidney–bladder unit and then the 12-unit system.
Each stented ureter unit consists of a stent placed within a natural latex rubber tube that simulates a ureter, connecting a renal unit to a bladder unit, as shown schematically in Figure 1. A latex tubing (NEWTEX, NewAge® Industries, Inc.), with an inner diameter of 3.175 mm and wall thickness of 0.79 mm, was determined (in comparison with several types of tubing) to feel most similar to the human ureter upon testing by different senior urologists. The use of latex tubing to mimic a ureter without peristalsis can be justified, further noting that stenting generally results in a pronounced reduction of ureteral peristalsis, 9 while accumulation of extracellular collagen in dilated ureters can lead to increased wall stiffness and reduced distensibility. 10

Schematic showing the experimental setup, with details of a single ureter–stent unit (including the angle of deformation, θ°).
Experiments were carried out using Double-J (pigtail) stents (Boston Scientific® Percuflex Plus) with 4.8F, 6F, 7F, and 8F diameters. The proximal pigtail end was inserted into a glass vessel representing a renal unit (volume ∼25 mL), while the distal pigtail was removed so that the stented ureter drained freely into a glass vessel representing a bladder unit (volume ∼30 mL). Note that the distal pigtail is not expected to have any effect on the dynamics investigated here given that the focus is on fluid and colloid flow dynamics from the inlet and through the critical region in the vicinity of the EUO-induced deformation and compression.
A piezometer connected to the renal unit allows measurement of pressure changes within the entire stented ureter system; the height of the outlet from the bladder unit is fixed to maintain a fully saturated system and stable piezometer measurements over time. The region of deformation and compression is established by passing the stented ureter through a molded, curved screw clamp design that controls the angle of deformation (set at θ = 40°, as shown in Fig. 1) and compression (set at 2000 g (≈19.6 N) over the clamped arc, about 3.5 cm in length, located in the region of maximum deformation). The clamping pressure was confirmed using a force meter (Lutron, Model FG-5000A). The angle of deformation and compressive pressure were prescribed on the basis of the analysis by Shilo et al. 7 Stented ureter units with no deformation or compression were also employed as controls for the experiments to clearly separate the effects of colloidal flow from those with synergy between deformation/compression and colloidal flow.
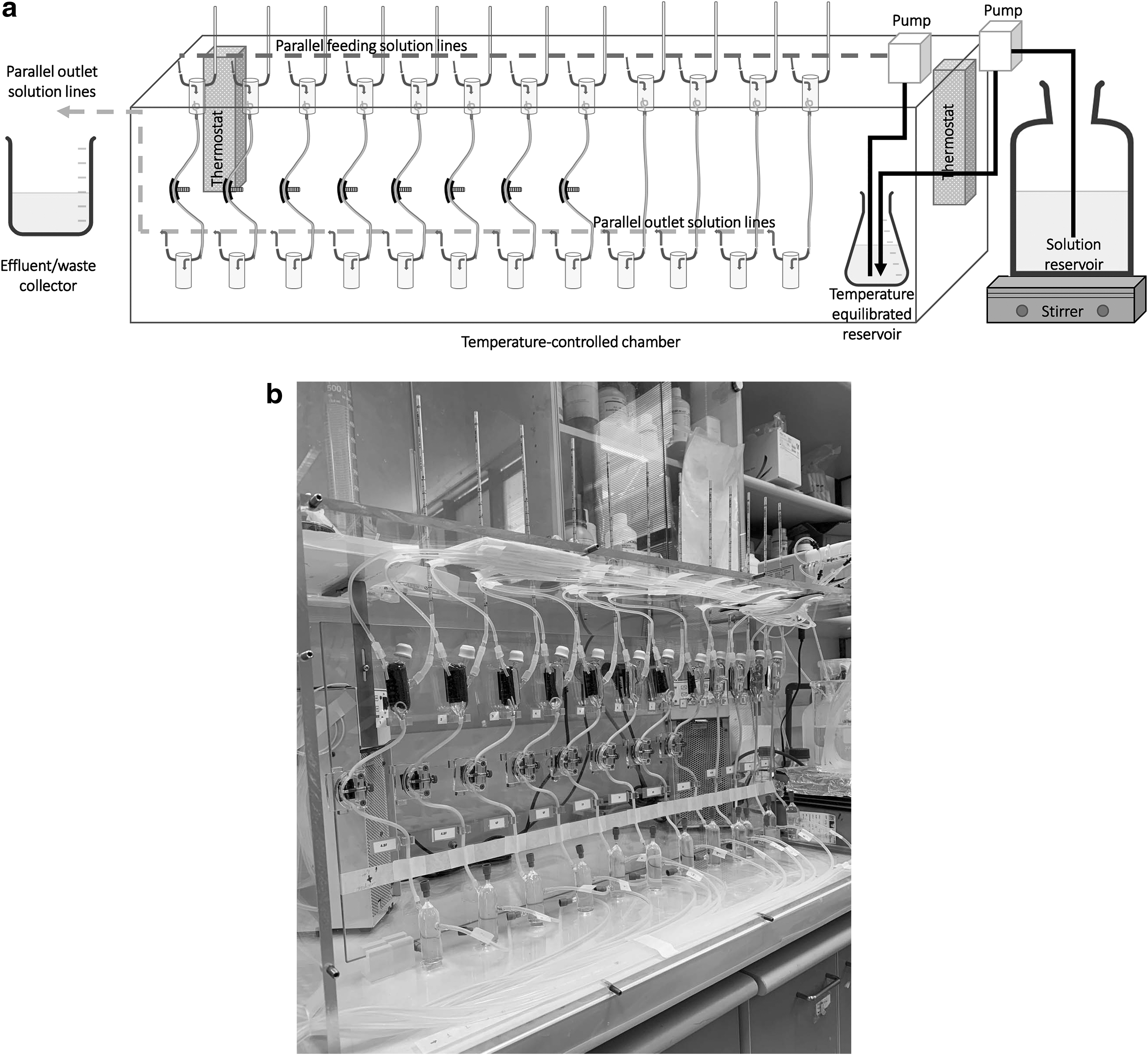
The 12-stent system is shown schematically in Figure 2a and as a photograph in Figure 2b. This system consists of 12 of the units shown in Figure 1. The units are placed within a temperature-controlled chamber, with two thermostat units that maintain the environment at 37°C. A large reservoir (6 L) supplies the colloidal solution to a smaller reservoir within the chamber, which then feeds each of the 12 units separately through a 12-channel peristaltic pump (Ismatec® Model IPC 12-channel pump). The fluid volume in the renal unit damped small pressure fluctuations induced by the pump.
Colloid flow experiment
A colloidal solution was used to examine synergetic effects between deformation/compression and the presence of colloids, with control systems involving ureter–stent units with no deformation/compression. The colloidal solution was double-distilled water (DDW) containing chicken albumin from egg white powder (Sigma A5253, molecular weight 44 kDa).
A few studies have specifically examined effects of colloidal material in urine, in vitro, with the major motivation and focus being on studying encrustation of catheters and ureteral stents. Three studies, in particular, employed a form of artificial urine that includes chicken albumin as the representative colloidal material. Cox et al. 11 employed a mixture of solutions containing urease and albumin to precipitate encrusting deposits, in vitro, on indwelling catheter materials in a reaction vessel. They reported that the deposits have the same chemical composition as that found on catheters with in vivo encrustation. The authors note that while albumin is not present in real urine, it can represent bacterial and cellular debris that are present frequently; moreover, albumin promotes mineral deposition that occurs in real urine and enables introduction of solutions with controlled and consistent colloid concentrations.
Tunney et al. 12 examined in vitro biomaterial encrustation on ureteral stent materials, depositing material similar to that found in vivo. A composition of artificial urine similar to that in the study by Cox et al. 11 was employed, but with a significantly lower concentration of albumin. In a study similar to that by Tunney et al., 12 Gorman et al. 13 examined dynamic biomaterial encrustation on catheter and stent materials in a flow-through system. These authors chose an even lower concentration of albumin specifically to avoid blockage of inlet tubes in the experimental setup. To summarize, all authors used a similar artificial urine composition, with chicken albumin in different concentrations as the representative colloidal material: Cox et al. 11 employed ∼10 g/L and Tunney et al. 12 chose 2 g/L, while Gorman et al. 13 used 0.4 g/L. We chose a chicken albumin concentration of 5 g/L in DDW (specific gravity of 1.001 at 37°C) given that our focus is on study of colloid aggregation and effects on the stented ureter, without effects of mineralization and deposition; these latter mechanisms are generally a somewhat slower process than aggregation, extending over weeks to months, and are thus less likely to account for ubiquitous ureteral stent failure within days due to EUO.
The temperature-controlled chamber (37°C) housed 12 stented ureter units, two each with 4.8F, 6F, 7F, and 8F stents under deformation/compression and one each with 4.8F, 6F, 7F, and 8F stents under no deformation/compression. Two sets of experiments were run, yielding four replicates of each stented ureter under deformation/compression and two replicates of each (control) unperturbed stented ureter.
The colloidal solution was injected through each stented ureter unit using the multichannel pump at a constant flow rate of 30 mL/hour. The volumetric flow was confirmed to be constant by measuring fluid volume at the outlets over time. In all cases, the maximum deviation from this flow rate at the system outlet was 1%. The fluid heights in the kidney unit piezometers remained constant, displaying only ∼1 mm (∼0.1 cmH2O) height variation due to the action of the peristaltic pump.
During the experiments, the fluid heights in each piezometer were monitored over time. Stent failure was defined as renal unit pressure over 10 cmH2O or complete obstruction of fluid flow; time to stent failure was measured. It was found that pressures beyond this point continued to rise, reaching the oft-defined obstruction pressure of 20 cmH2O defined by the Whitaker test. 14
Results
First, in a preliminary analysis using the experimental setup and protocol of Shilo et al., 7 we confirmed that the 8F stent shows absolutely no decrease in flow (or increase in renal pressure) up to 5000 g compression. We showed previously in tests with 4.8F, 6F, and 7F stents that deformation and compression alone are not generally sufficient to lead to stent failure under EUO. 7
Based on the two complete sets of experiments, monitoring four replicates of stented ureters under deformation and compression and two replicates of the control (unperturbed) stented ureters, the average time for stent failure in the 4.8F and 6F stents was 44 hours (range 31–59 hours) and 66 hours (range 24–92 hours), respectively, as shown in Table 1. The 7F ureteral stent failed in two of the repetitions after an average time of 75 hours and continued to drain in the other two repetitions with a mild rise in renal unit pressure throughout the experiment. The 8F ureteral stent showed no change in renal unit pressure in any of the repetitions. Significantly, none of the control stents with no deformation or compression (4.8F, 6F, 7F, and 8F) exhibited any change in renal pressure in any of the replicates. It is noted that throughout the experiments, small rises (as much as 1–1.5 cm)—and then falls—were observed in some of the piezometers, evidently as pressure builds up and colloids are then released or rearranged in the stented ureter system.
Time to Stent Failure (Blockage) Under Deformation of 40° and Compression of 2000 g in the Region of the External Ureteral Obstruction
Entries with “—” indicate no failure.
Exhibited mild rise in cmH2O (∼4–5 cm) in the renal unit.
For experiment duration of 100 hours.
Discussion
The fact is that polymeric ureteral stents often fail under EUO. 2 While it may be intuitive to attribute stent failure to deformation of the ureter and external pressure, which lead to occlusion of the stent lumen, it appears that reality is more complex. We showed previously 7 that deformation and compression alone do not generally cause stent failure, at least over periods of days. Other authors 1 suggested that colloids or debris play a role in obstructing stents and thus stent failure. In this experiment, based on the control stented ureter system, we find that colloids alone do not cause stent failure over the same duration. Rather, it is the combination of external pressure, deformation, and colloid concentration that can lead to stent failure. For a stented ureter under EUO, the main path for urine to flow down into the bladder, in the vicinity of the EUO, is through the ureteral stent lumen. We find that the 4.8F stents fail consistently, as do the 6F stents. The 7F stent also shows a tendency to failure, while the 8F stent is not prone to failure (at least relative to the time scales for failure of the other stents). Variability in time to failure is evident, even among stents with the same size: this behavior is reasonable given the random nature of colloid inflow, aggregation, and trapping within the stent lumen and within the ureter–stent annular lumen, as well as the possible impact of the stent side holes and their potential blockage. These findings, which support the use of large lumen stents in EUO, are consistent with opinions of other authors 1,15 who concluded that the use of stents with maximal diameters is preferable as they are more resistant to (or less likely to suffer from) obstruction.
The advantage of larger luminal stents under EUO may be related to several possible explanations, but largely to the fact that flow is facilitated through stents with a larger inner diameter. Noting that urine can flow along (often interconnected) pathways through the stent (intraluminal) and through the ureteral lumen (between the stent and the ureter wall, extraluminal), for example, Brewer et al. 15 measured intraluminal, extraluminal, and total flow rates of urine in stented ureters of minipigs through in vivo experiments. These authors noted that larger luminal stents had higher intraluminal and total flow rates compared with narrower stents. Additionally, in this context, the authors emphasized the significance of the internal stent diameter rather than its external diameter. This fact should be emphasized given reported differences of ureteral stent wall thicknesses among different manufacturers, and even among various sizes of stents by the same manufacturer, which lead to stents of the same (e.g., 6F) size having different internal diameters. 7,16
Another advantage of large luminal ureteral stents under EUO derives from the influence of external pressure over the stented ureter. Because the internal diameter improves luminal flow, it is important for the stent to be resistant to outer and radial pressure to prevent partial occlusion of the stent. Hendlin et al. 17 noted that larger luminal stents are less resistant to radial compression that can lead to stent occlusion. However, their model used a two-point opposing pressure rather than areal pressure, which was placed directly on the stent rather on a stented ureter. Davis et al., 16 on the other hand, showed a 6F ureteral stent to be more resistant to radial pressure than a 4.8F stent, underlining the resistance of larger ureteral stents to radial compression; the wall thickness of the 4.8F stent, too, was smaller than that of the 6F and 7F stents.
In our experiments, visual examination of the obstructed stented ureter units indicated that colloids accumulated both within the stent (insertion of a guidewire released colloidal aggregates; measuring the length of the inserted guidewire confirmed the approximate location of the aggregates) and in the ureter–stent lumen, at and proximal to the region of compression as well as further proximal to it. In addition, larger colloids were seen to accumulate near the region connecting the renal unit to the stented ureter (the simulated ureteropelvic junction), particularly for the larger (7F, 8F, and in some cases, the 6F) stents. A possible explanation for this finding is that the lumen between the stent and the ureter is relatively narrow so that some larger colloids (and colloid aggregates) can accumulate in this region, while others can travel through the stent. In contrast, the wider lumen between the ureter and the 4.8F stent enables the passage of larger colloids. When considering colloids (and colloid aggregates), it should also be noted that hole diameters along the stent walls vary in size, being largest for the 7F and 8F stents, smaller for the 6F stent, and even smaller for the 4.8F stent. A combined (in vitro) experimental and computational fluid dynamics study by Mosayyebi et al. 18 demonstrated similar particle accumulation behavior in a stented ureter around inactive stent holes and ureteral cavities formed by occlusions. These obstructed regions, with low wall shear stress, facilitate encrustation, particularly at lower flow rates. Indeed, we believe that stent encrustation and incrustation may resemble the process in which debris and colloids obstruct the stent–ureter lumen.
Finally, we note that results obtained here for colloid accumulation, in both the stent and the stent–ureter lumen, are supported by the fluid dynamics theory. First, fluid flow in a curved annulus having a local constriction at the outer wall—such as in the case of a curved and deformed stented ureter subjected to EUO—is prone to significant variations in the pressure gradient and frictional resistance, which lead to a highly nonuniform flow pattern. 19 Second, and especially for strong laminar flow such as in our system, 7 quantitative analysis 20,21 of colloid suspensions in tubular flow shows that colloids can accumulate particularly in regions where curvature, deformation, and compression alter the cylindrical cross section of a tube and/or annulus (such as in the vicinity of an EUO in a stented ureter).
There are several limitations to our study. The latex tubing simulating a ureter has physical characteristics that are different from real ureteral walls (which vary among patients and in response to different treatments) and the lack of (even minimal) peristaltic motion may have some effect on the results. Moreover, dynamic ureteral responses caused by indwelling stents and EUO will likely further affect the flow dynamics over time, such as reflux or retrograde pressure transmission through and/or around the stent. Moreover, the results here are a function of the type and concentration of colloid material and the use of DDW containing no other salts, enzymes, and organic materials. As such, stent mineralization, various colloid aggregation properties, and biological activity remain unaccounted for. Clearly, the occurrence of blockage and the actual time to blockage (and variability among replicate experiments) are also affected by colloid concentration. Another limitation is our use of single polymer stents, while metal and tandem (polymer) ureteral stents are currently reported 22,23 to treat the EUO with encouraging success rates. On the other hand, larger diameter stents and tandem stents might be less tolerable for patients. Notwithstanding the above, we note that to the best of our knowledge, this is the first study to systematically measure effects of colloidal fluid flow in stented ureter systems, both under and without EUO, while also accounting for the relative impact on stents of different sizes.
Conclusions
The phenomenon of stent failure under EUO is commonly attributed to extrinsic pressure placed on the ureter and stent. We suggest that the presence of colloids in urine may play a critical synergetic role in stent failure. We evaluated the efficacy of different ureteral stent diameters under EUO in the presence of colloidal material in the fluid, demonstrating that large-diameter stents are more effective in ureteral drainage under EUO. We conclude that colloidal fluid may play a critical role in stent failure under EUO. These experiments may assist in selection of the most effective stent for drainage.
Future experiments using different colloid compositions and concentrations, and/or employing urine, as well as examining other types of ureteral stents (e.g., metal and [polymer] tandem) to further understand and confirm factors that control stent failure under EUO remain to be undertaken.
Footnotes
Acknowledgments
B.B. appreciates the support of a research grant from the Estate of Emile Mimran. B.B. holds the Sam Zuckerberg Professorial Chair in Hydrology. The authors thank Yacob Zilberstein for construction of the glass renal and bladder vessels and Prof. Jacob Karni for useful discussions on fluid dynamics and dispersion of colloidal suspensions.
Author Disclosure Statement
No competing financial interests exist. The choice of supplier for the stents was arbitrary, but consistent with those used in our previous publication.
Funding Information
No funding was received for this article.