
Abstract
Introduction and Objective:
Ureteroscopy (URS) and percutaneous nephrolithotomy (PCNL) are standard treatments for intermediate-size (15–20 mm) kidney stones but differ in their postoperative recovery, stone-free rates, and complication risks. We aimed to evaluate what affects patient treatment preferences.
Methods:
Patients with urinary stone disease completed a choice-based conjoint analysis exercise assessing four treatment attributes associated with URS and PCNL. A sensitivity analysis using a market simulator was performed, and the relative importance of each attribute was calculated. Differences in treatment preferences by demographic subgroup were assessed.
Results:
A total of 58 patients completed the conjoint analysis exercise. Stone-free rate was the most important treatment attribute, while the length of hospital stay and cosmesis were less important. Overall, sensitivity analysis based on market simulation scenarios predicted an almost equal preference for URS (52.4%) compared with PCNL (47.6%) for treatment of an intermediate-size stone. Older patients (>65 years old) expressed their stronger preferences for lower infection rates and shorter hospital stays, and were more likely to prefer URS (67.2%, 95% confidence interval [CI]: 52% to 82.5%) compared with younger patients (20–34 years old) (20.3%, 95% CI: 0% to 41.5%) who preferred higher procedure success rates and fewer repeat procedures.
Conclusion:
Conjoint analysis predicts nearly equal patient preference for URS or PCNL for the treatment of intermediate-size kidney stones. Older patients prefer the lower urinary tract infection risk and shorter hospital stay associated with URS, while younger patients prefer higher stone-free rates associated with PCNL. These results can help guide urologists in counseling patients and improve the shared decision-making process.
Introduction
Ureteroscopy (URS) and percutaneous nephrolithotomy (PCNL) are two standard surgical treatments for the management of intermediate-size (15–20 mm) kidney stones. 1,2 Each procedure differs in treatment attributes such as stone-free rates, postoperative recovery time, and complication risks. 2 –7 URS is often performed as an outpatient procedure and, compared with PCNL, has a lower risk of postoperative urinary tract infection (UTI) and bleeding complications. 2,8 –11 However, PCNL, which is typically performed as an inpatient procedure, is a highly effective treatment with reported stone-free rates ∼95% for 15 to 20 mm intrarenal stones, 3,4,12 and requires fewer repeat procedures compared with URS. 5,13 When facing treatment decisions, patients weigh the potential harms and benefits of each procedure before deciding on a treatment plan with their provider. Understanding how patient demographic factors influence treatment preferences can help guide providers in the shared decision-making process and ultimately enhance patient-centered outcomes. 14
There has been increasing attention in recent years on the role of patient preferences in the shared decision-making process. 14 Conjoint analysis is a method for studying patient treatment preferences and determining how much importance patients place on specific treatment attributes. This choice-based analytical exercise was initially developed in market research to study how product attributes affect consumer preferences. Participants are offered a series of hypothetical scenarios and asked to choose their preferred option. In the clinical setting, conjoint analysis has been effectively used across multiple medical specialties including oncology, orthopedic surgery, and urology to determine the relative importance of various treatment attributes and to elucidate how patient demographic factors affect treatment preferences. 15 –18
Herein, we apply conjoint analysis methodology to understand surgical treatment preferences in patients with urinary stone disease to identify which treatment attributes are most important to patients when they are choosing between URS and PCNL for management of an intermediate-size kidney stone. Furthermore, we sought to determine how patient demographic factors affect stone treatment preferences.
Patients and Methods
After institutional review board approval, patients with urinary stone disease undergoing treatment at an academic kidney stone center were invited to complete an online choice-based conjoint analysis exercise. The conjoint analysis assessed four treatment attributes associated with URS and PCNL, including: (1) length of hospital stay (outpatient surgery vs 1–2 days inpatient admission); (2) stone-free rate (70% vs 95%); (3) postoperative UTI (1% vs 5%); and (4) cosmesis (skin incision vs no skin incision). Levels for each attribute were selected based on published clinical outcomes after surgical treatment for intermediate-size (15–20 mm) kidney stones (Table 1). In addition, patients completed a brief questionnaire on demographic information (gender, age, race, marital status, education level, and income level) and past surgical treatment for urinary stone disease (e.g., URS, PCNL, or shockwave lithotripsy). The conjoint analysis was developed and administered using the Sawtooth Discover Web Application (Sawtooth Software, Inc., Provo, UT).
Evidence Used to Select Treatment Attributes and Levels for Conjoint Analysis
PCNL = percutaneous nephrolithotomy; URS = ureteroscopy; UTI = urinary tract infection.
Patients were given eight questions regarding treatment attribute levels and asked to rank the desirability of each attribute (Undesirable, Somewhat Desirable, Very Desirable). They then answered seven choice-based conjoint exercise questions in which they are offered two hypothetical treatment scenarios and prompted to choose their preferred option. The treatment scenario questions included random combinations of treatment attributes and were designed to assess how much importance patients placed on each attribute (Fig. 1).
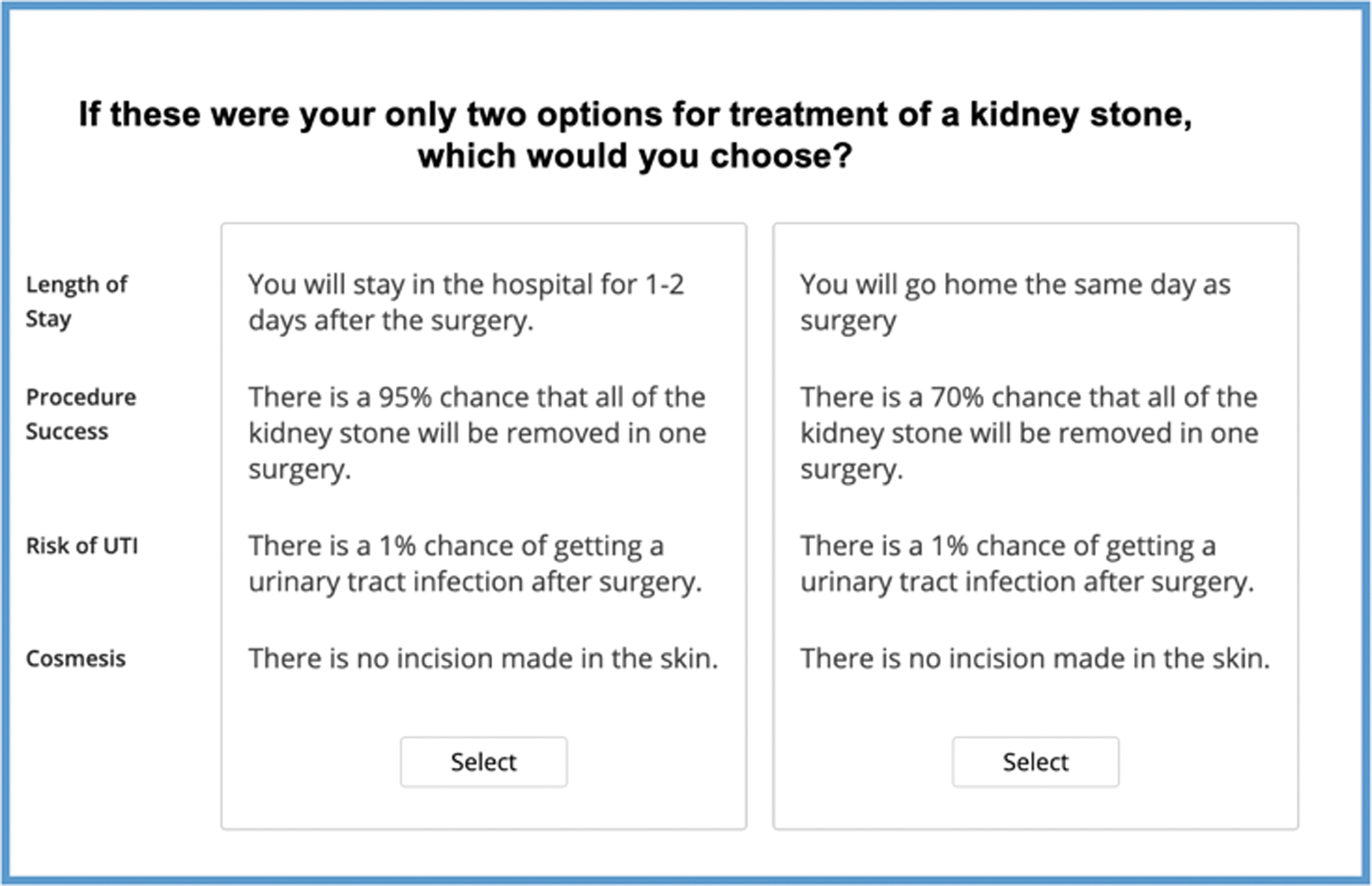
Example of a choice-based conjoint analysis scenario question.
The conjoint analysis was performed using Market Simulator software within the Sawtooth Discover Web Application to predict the proportion of participants who would select each treatment option (URS vs PCNL). The details behind this approach have been previously published. 19 Conjoint analysis utilities of each attribute level were calculated. A conjoint analysis utility is a numerical score assigned to each attribute and used in conjoint analysis coding to measure how much an attribute influences a participant's decision. By measuring the range in utility of each attribute, the relative importance of each treatment attribute was calculated. Demographic characteristics were selected for additional stratified analyses, and confidence intervals (CIs) between subgroups were calculated. Statistical significance was determined based on the degree of overlap of the 95% CIs between subgroups.
Results
Between December 2019 and March 2020, 64 patients were recruited to participate in the choice-based conjoint analysis exercise. The total analytic cohort included 58 participants after 6 patients (9%) were excluded for not completing all choice-based scenario questions. Half of the participants were female, the majority of participants were >50 years old (65%), and most participants had prior history of surgical treatment for urinary stone disease (71%). Demographic characteristics and treatment history are listed in Table 2.
Patient Characteristics
SWL = shockwave lithotripsy.
Participants rated stone-free rate as the most important treatment attribute in decision making (relative importance 42.5%, 95% CI: 37% to 47.9%), followed by risk of postoperative UTI (25.3%, 95% CI: 20.9% to 29.7%), cosmesis (17.3%, 95% CI: 12.9% to 21.8%), and length of hospital stay (14.9%, 95% CI: 11% to 18.7%) (Fig. 2). Utility associated with the PCNL procedure success rate (95% stone-free rate) was 80.9 (95% CI: 68.2 to 93.8), significantly higher than any other treatment attribute utility. There was no significant difference in average utility or relative importance of treatment attributes between the treatment naïve patients and patients with history of prior surgeries for urinary stone disease. The relative importance of stone-free rate was 39% (95% CI: 31.2% to 46.9%) in patients with prior history of URS, compared with 45.9% (95% CI: 38.3% to 53.5%) in patients without prior history of URS. Prior history of URS did not appear to affect treatment preference between URS and PCNL. Patients with prior history of URS had nearly equal preference for URS compared with patients with no prior history of URS (53.2% and 51.5%, respectively).

Relative importance of four treatment attributes for surgical management of intermediate-size kidney stones.
Despite participants valuing stone-free rate as the most important treatment attribute, other attributes also played a role in the treatment decision-making process. Overall, conjoint analysis predicted an almost equal preference for URS (52.4%) compared with PCNL (47.6%) for the treatment of intermediate-size kidney stones. However, treatment preferences varied significantly by age group with the oldest cohort (>65 years old) preferring URS (67.2%, 95% CI: 52% to 82.5%) and the youngest (20–34 years old) preferring PCNL (79.7%, 95% CI: 58.5% to 100%) (Fig. 3). While all age groups preferred higher stone-free rates, younger patients had a stronger preference against lower stone-free rates (Utility −108.1 (95% CI: −125.6 to −90.6), suggesting that they are less likely to accept additional procedures. Conversely, patients ≥50 showed a significant preference for outpatient surgery and lower UTI rates.
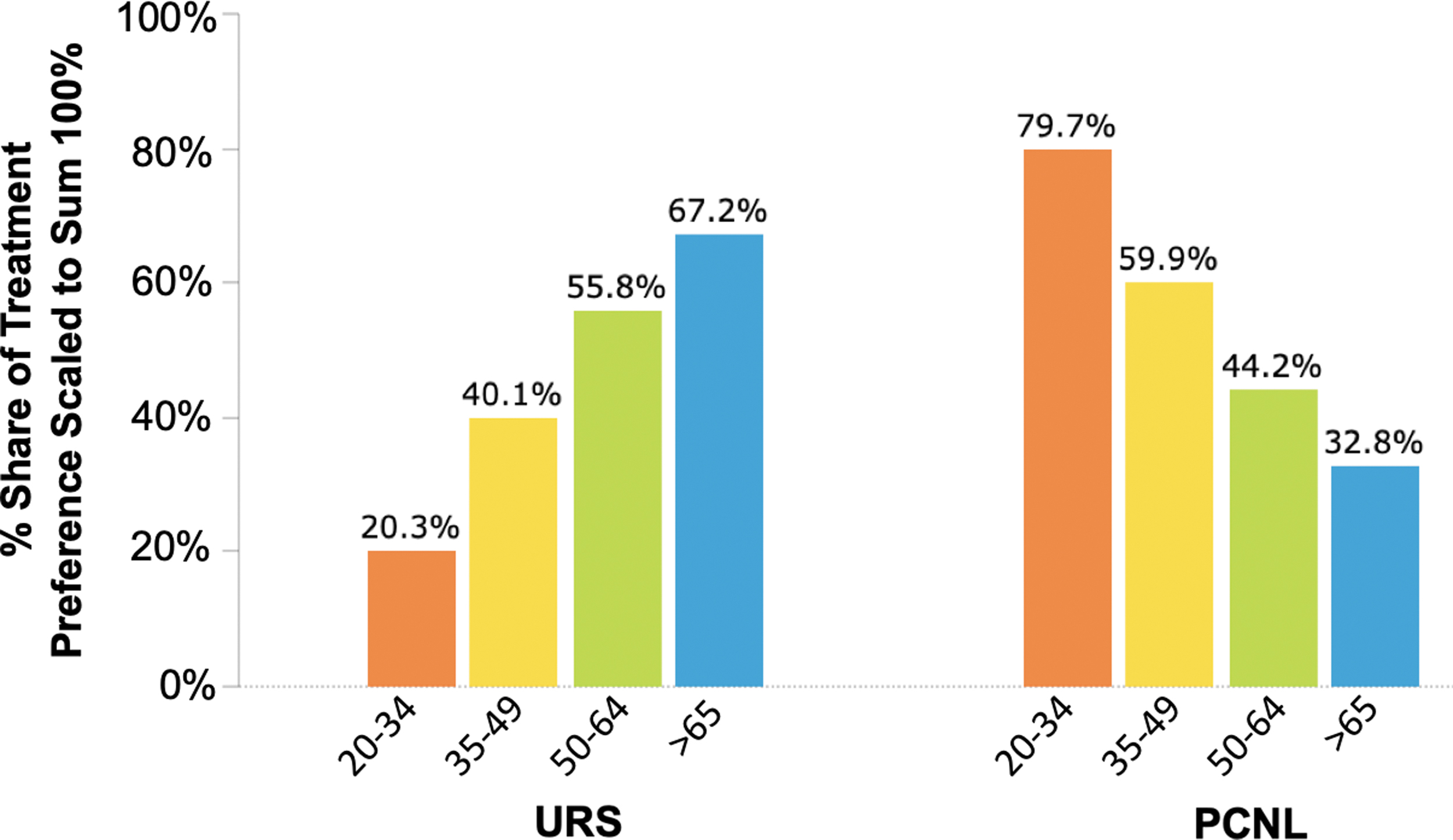
Predicted treatment preferences by patient age for management of intermediate-size kidney stones based on conjoint analysis.
Discussion
In this study, we find a nearly equal preference among participants for URS and PCNL (52.4% and 47.6%, respectively) for the treatment of intermediate-size (15–20 mm) kidney stones. Although PCNL is the recommended treatment for kidney stones >20 mm, the European Association of Urology (EAU) Guidelines recognize both URS and PCNL as recommended first-line treatment options for solitary kidney stones <20 mm in size. 1,5 The drawbacks of PCNL include higher postoperative complication rates and longer hospital stays, 2,6,9 –11 while the disadvantages of URS include lower stone-free rates and need for staged procedures. 2 –7 In well-informed patients, the advantages and disadvantages of each procedure appear to be counterbalanced, and as a result, neither procedure stands out as a clear favorite among our study participants. Decisions regarding the surgical approach for intermediate-size stones should incorporate individual patient preferences.
Our results show that patients consider the stone-free rate to be the most important treatment attribute. This relative importance of stone-free rate is observed across all demographic subgroups. Several systematic reviews have shown that the stone-free rate of PCNL is superior to URS for intermediate-size stones. 2,7,13,20 While stone-free outcomes will vary for patients depending on the exact stone size, location, and density, reported stone-free rates for PCNL in patients with 15 to 20 mm intrarenal stones can range from 90% to 98%, 3,4,12 while stone-free rates for single-stage URS range from 65% to 80%. 12,21,22 Urologists should take into consideration patient preferences as well as anatomical and stone factors that may alter stone-free rates when counseling patients.
We found that patient preferences for treatment of intermediate-size kidney stones vary across age groups. While patients of all ages prefer high procedure success rates, younger patients (<35 years) have the strongest preference for higher stone-free rates. Therefore, younger patients may be less willing to undergo staged URS procedures for treatment of intermediate-size kidney stones and more satisfied with the higher stone-free rate associated with PCNL. On the contrary, older patients (>50 years) appear to prefer to avoid hospital admission and postoperative UTI. While the underlying reasons for these preferences were not fully assessed in our study, aversion to hospital admission may be related to prior hospital experiences, concerns over hospital-acquired infections, or desire for autonomy at home. Given these preferences, older patients may be less inclined to choose the more invasive surgical approach of PCNL with its higher UTI rate and longer hospital stay.
Our results are consistent with previous decisional aid studies in urologic disease. Omar and colleagues found that when deciding between extracorporeal shockwave lithotripsy and URS in a hypothetical scenario of an 8 mm kidney stone, patients prioritize procedure success rate as the most important factor impacting choice of treatment. 23 Similarly, Hampson and colleagues applied a conjoint analysis model to men with urethral stricture disease, and found that procedure success is the most important treatment attribute in deciding between urethroplasty and endoscopic treatment. 17 However, they found that younger men preferred outpatient procedures for urethral stricture disease even at the cost of decreased efficacy, whereas we demonstrate that younger patients more often prefer the more invasive treatment for kidney stone disease.
Understanding and incorporating patient preferences into the shared decision-making process are becoming increasingly important in surgical fields. Patients who participate in shared decision making have higher treatment satisfaction, improved patient-centered outcomes, and decreased decisional conflict compared with patients who are not engaged in the decision-making process. 14,18 Before deciding on a treatment for kidney stone disease, urologists should consider discussing with their patients about expected stone-free rates and potential need for future surgical procedures, especially for younger patients. For older patients, a discussion of associated complication risks and anticipated hospital admissions will play an important role in helping them decide on their preferred treatment.
Our study has a number of limitations. Our cohort consisted of patients from a single institution where the majority of patients had higher socioeconomic status, and thus our findings may not be generalizable to patients from different geographic locations or of lower socioeconomic status. In addition, the online survey was in English; therefore, non-English readers and patients with low literacy are not represented in our cohort. Our cohort size is smaller than most conjoint analysis-based studies of similar design, and our subgroup analysis includes only four participants in the youngest age group (20–34 years). However, despite this small number, we noted a significant difference in treatment preferences between the youngest and oldest age groups, and showed a consistent trend in treatment choice over increasing age groups. We chose to include only URS and PCNL as treatment options for intermediate-size stones in our conjoint analysis and excluded other treatment options such as shockwave lithotripsy. In addition, our analysis did not account for variation in procedural techniques such as mini-PCNL or ambulatory PCNL, which may affect patient preferences. We chose to include only four treatment attributes and did not include other potential attributes, such as bleeding risk, procedure cost, or need for ureteral stent or nephrostomy tube. We decided to limit our analysis to only two treatment options and four attributes to reduce the time required to complete the conjoint analysis exercise for participants. This approach allowed us to prevent the survey from becoming too complex and allowed us to focus on easily understandable topics with clearly quantifiable attribute levels. Finally, most participants in our cohort had a previous history of surgical treatment for urinary stone disease, which may have introduced bias or affected treatment decision preferences. Although our analysis did not show a significant difference in utility or relative importance of treatment attributes between treatment naïve patients and those with a history of prior kidney stone surgery, the smaller size of our cohort may be inadequate for a comparison between these groups.
Despite these limitations, our analysis provides important information on which treatment attributes are most important to patients when they are deciding on surgical therapy for intermediate-size kidney stones. Patient preferences appear to be in line with the surgeon's aims to maximize stone-free rate while minimizing complications and length of hospital stay. Our results reveal differences in treatment preferences between age groups, and these results can help guide urologists in counseling patients with kidney stone disease. This conjoint analysis exercise may also be a useful tool for patients to promote education on treatment options, empower patients to share their treatment preferences, and ultimately improve shared decision making in the treatment selection process.
Conclusion
Conjoint analysis predicts nearly equal patient preference for URS or PCNL for the treatment of intermediate-size kidney stones. Most patients prefer a procedure that will result in stone-free status. Older patients prefer the lower UTI risk and shorter hospital stay associated with URS, while younger patients prefer higher stone-free rates associated with PCNL. These results can help guide urologists in counseling patients and improve the shared decision-making process.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding information was provided.