
Abstract
Introduction:
With a rise in the incidence of stone disease, more research is needed to understand the lifestyle factors associated with it. We evaluate available evidence for association of smoking, alcohol, and exercise with kidney stone disease (KSD).
Methods:
A systematic literature search was conducted in CINAHL, EMBASE, Ovid Medline, Cochrane Library, Scopus, Clinicaltrials.gov, and Google Scholar. Different keywords were “smoking,” “cigarette,” “alcohol,” “spirits,” “exercise,” “physical activity,” “training,” “kidney stone,” “stone disease,” “nephrolithiasis,” “urolithiasis,” “renal stone,” and “urinary stone.” The main outcome of interest was the role of smoking, alcohol, and exercise in the development of KSD.
Results:
A total of 4921 articles were found on searching the databases, of which 14 met the criteria for inclusion in the final review. Studies assessed the following risk factors, physical activity (n = 6), alcohol (n = 6), and smoking (n = 9), and included 17,511 patients. The relationship of physical activity with KSD appears to be equivocal. In addition, only one study demonstrated a decreased risk of nephrolithiasis with alcohol consumption. On the contrary, four studies found a significant association between smoking and renal stone formation.
Conclusions:
While smoking is one behavioral factor that seems to have some association with KSD, no clear effect of alcohol and physical activity has been demonstrated. To avoid KSD, awareness of the possible detrimental role of smoking should be considered and patients should remain vigilant about the importance of hydration with physical activity. While this represents the most appropriate guidance from the evidence available, at present there remain insufficient data to truly reveal the relationship between these three factors and KSD.
Introduction
The lifetime prevalence of kidney stone disease (KSD) is 14% and epidemiologic data have confirmed this is increasing. 1,2 Furthermore, at least 50% of the patients will experience a stone recurrence within 10 years. 3 The burden of KSD is far-reaching, both at an individual and society level. 4,5 As well as the detrimental effects on a patient's quality of life, the economic sequelae are also extensive. The annual cost is estimated to exceed $4 billion in the United States by 2030, notwithstanding the additional costs incurred by a patient for lost work. 4 Geraghty and colleagues reported the average stone episode in the United Kingdom to be as high as £2187, with the cost of KSD being comparable with the combined cost of bladder and prostate cancer. 5
While treatment methods have improved with regard to efficacy and safety, research and development are also required to continue understanding the etiology and preventative measures. 6 The association between an array of dietary factors such as salt, animal protein, and urinary stone formation is now well recognized. 7,8 Other lifestyle factors such as smoking, alcohol, and physical activity have also been incriminated to play a role in lithogenesis. 9 However, evidence and recommendations remain underreported. Each of these represents a modifiable risk factor and further attention is therefore warranted. This is especially true given the prevalence of poor lifestyle behaviors and choices. Of note, in 2010, it was reported that 28.1% of the population in China were smokers. 10 The possible implications and the potential for remedial action are therefore immense. This review aims to evaluate the available evidence for association of lifestyle factors such as smoking, alcohol, and exercise with KSD, with the intention that clinical recommendations can be drawn to help prevent primary and recurrent stone disease.
Materials and Methods
Evidence acquisition
Inclusion criteria
Studies in English language looking at the of role of smoking, alcohol, and/or exercise in KSD.
Studies over the past two decades.
Adult patients.
Studies that clearly recorded separate intake of alcohol and smoking to allow for subsequent analysis and possible identification of independent risk factors.
Exclusion criteria
Animal and laboratory studies.
Review articles and gray literature.
Studies looking at the role of dietary factors or volume of water intake in KSD.
Search strategy and study selection
A systematic literature search was conducted according to the Cochrane specifications and Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) protocol. 11 The search strategy was devised and conducted to find relevant articles from bibliographic databases, including CINAHL, EMBASE, Ovid Medline, Cochrane Library, Scopus, Clinicaltrials.gov, and Google Scholar. The search was confined to all English-language articles between January 2000 and January 2020. Search terms included (but were not limited to): “smoking,” “cigarette,” “alcohol,” “spirits,” “exercise,” “physical activity,” “training,” “kidney stone,” “stone disease,” “nephrolithiasis,” “urolithiasis,” “renal stone,” and “urinary stone.” Boolean operators (AND, OR) were used to augment the search. Two reviewers (S.S. and P.J.) identified all studies independently and any discrepancies were resolved by the senior author (B.K.S.). When additional information or clarification was needed, the primary authors of the studies were contacted directly. The main outcome of interest was the role of smoking, alcohol, and exercise in the development of KSD. Older articles, as well as animal and laboratory studies, and reviews related to the subject are described in a purely narrative manner and not included in the qualitative analysis.
Analysis
A narrative approach was adopted to analyze the data given its heterogeneous nature. It was determined by mutual consensus between the authors that it was not appropriate to carry out a formal meta-analysis using, for example, a global estimate effect. The wide range of cutoff values would also likely impact this. The Newcastle/Ottawa Scale (NOS) was implemented for quality appraisal. 12
Results
A total of 4921 articles were found on searching the databases, of which 140 abstracts were reviewed, and 14 articles met the criteria for inclusion in the final review (Fig. 1). Of them, 11 were case/control and the remainder were cohort studies. All of these applied a questionnaire as an assessment tool. In total, data from 17,511 patients were included. Studies assessed the following risk factors: physical activity (n = 6), alcohol (n = 6), and smoking (n = 9) (Table 1).
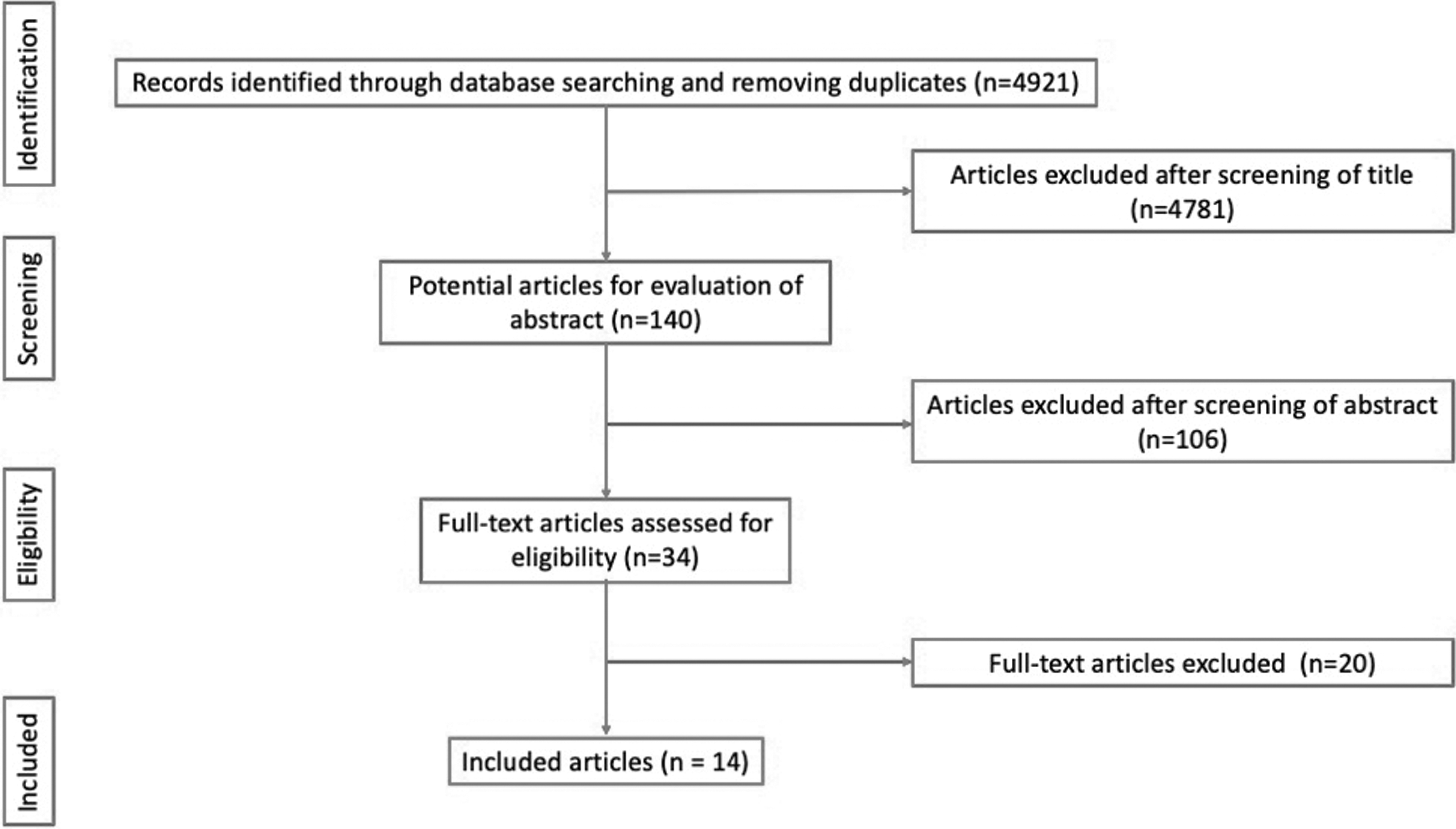
PRISMA flowchart of the included studies. PRISMA = Preferred Reporting Items for Systematic Reviews and Meta-Analyses.
Study Profiles, Patient Demographics, and Lifestyle Factors Associated with Kidney Stone Disease
aHR = adjusted hazard ratio; CI = confidence interval; KSD = kidney stone disease; NR = not recorded.
Physical activity
Three studies reported no effect of physical activity on KSD risk. 13 –15 In contrast, two groups reported a statistically significant protective role of exercise. 16,17 Sorensen and colleagues reported a reduction risk of stone formation associated with physical activity of women and this was independent of intensity of activity, caloric intake, and body mass index. 16 More specifically, compared with inactive women, the risk of incident stones decreased by 16% in women with the lowest physical activity level (adjusted hazard ratio [aHR] 0.84; 95% confidence interval [95% CI] 0.74–0.97). By increasing activity, the risk of incident stones declined further reaching a decrease of ∼31% (aHR 0.69; 95% CI 0.60–0.79). 16 Furthermore, Zhuo et al. showed that the duration of physical activity was an independent risk factor significantly associated with the occurrence of KSD (OR 0.840; 95% CI 0.808–0.973). 17 In contrast, Zhao and colleagues concluded that daily exercise greater than 30 minutes in duration could significantly increase the risk of KSD (OR 2.1; 95% CI 1.3–3.5). 18
Ferraro and colleagues suggested that the reason their nonrandomized study did not find any effect of exercise on KSD was due to unmeasured and/or unknown variables. 13 Maric and colleagues were also unable to add any reasoning for the lack of association. 15 The former study was limited by including a sample of nearly all Caucasian patients, no patients younger than 40 years, and no breakdown of stone composition. Five out of the six studies therefore showed no detrimental effect of exercise on risk of KSD, while one study found it detrimental but only in those who completed more than 30 minutes of physical activity. It may be therefore that overexercising and dehydration are risk factors for KSD.
Alcohol
Six studies determined no significant effect of alcohol intake on urinary stone disease. 18 –23 However, in a classic twin study analysis by Goldfarb et al., it was found that alcohol consumption in the past 2 weeks was associated with a decreased risk of nephrolithiasis (OR = 2.7; 95% CI 1.0–7.7). 24 Nonetheless, the same group found no significant association for lifetime consumption of at least 20 alcoholic beverages, daily intake of wine or hard liquor in the past 2 weeks, or alcohol intake in the past month. Finally, this study reported a hereditary link and a protective effect of coffee and perhaps tea, fruits, and vegetables.
Smoking
Five of the studies that investigated the effect of smoking on KSD showed no positive correlation. 15,18,19,21,25 However, the remaining four studies that assessed this did find a significant association. 14,22,23,26 More specifically, Hamano and colleagues demonstrated an increased significance of smoking risk for KSD in a multivariate logistic regression analysis (OR 4.29; 95% CI 2.68–6.86; p < 0.0001). 23 In addition, Liu and colleagues defined cigarette smoking as an independent risk factor (OR 1.66; 95% CI 1.11–2.50; p = 0.014) for calcium urolithiasis development. 22 Moreover, Tamadon and colleagues recorded a significant increase of nephrolithiasis risk with smoking (OR 2.06; 95% CI 1.06–4.01; p = 0.034). However, no significant difference in the number of cigarettes smoked (p = 0.830) and years of smoking (p = 0.536) between subjects with and without stones (p = 0.536) was found. 26 Finally, another survey study by Soueidan and colleagues showed that KSD patients had higher rates of smoking (7% vs 21%, p = 0.02) and were 8.5 times more likely (95% CI 2.2–32.2) to be current smokers. 14
Quality appraisal of studies
Overall, there was a good quality of evidence of included studies, as the scientific rationale and study objectives were clearly documented, and the selection and definitions for control groups were well done. Most case/control studies adequately drew the nonexposed cohort from the same community as the exposed cohort, rather than from a different source or not providing any description of their derivation at all. The average appraisal score using the NOS was 5.6/9 (range 5–7) (Table 2). Areas of weakness across studies included the method of outcome assessment. Few studies implemented an independent blind assessment. Instead, they used either self-report or provided no description.
Lifestyle Effect of Physical Activity, Smoking, and Alcohol and Quality Appraisal of the Studies
Where changes are statistically significant (p < 0.05).
BMI = body mass index; NOS = Newcastle/Ottawa Scale.
Discussion
Key findings
While the European Association of Urology (EAU) acknowledges lifestyle factors in the development of KSD, this is not expanded upon. 27 Given the known relationship between coronary heart disease (CHD) and KSD, in theory, it would be anticipated that risk factors for CHD could also contribute to KSD at least indirectly. 13 Similarly, the association between metabolic syndrome (which includes obesity, hypertension, high triglyceride levels, and diabetes) and KSD is well established, 8 while lifestyle factors such as physical activity, alcohol, and smoking, all, in part, directly or indirectly cause metabolic syndrome.
Link to activity
There have been few studies investigating the relationship between physical activity and KSD. Given the widely known cardiovascular benefits of regular exercise, in theory, it should serve a protective role as it also decreases the risk of metabolic syndrome and improves hypertension. 28 While the findings by Zhao and colleagues at first seem contradictory to this logic, a closer review reveals why this is likely the case. 18 Their study would infer a patient's overexercising and perhaps not hydrating sufficiently. The urine would, therefore, be concentrated and this could potentially increase the risk of crystallization and stone formation. This is supported by earlier studies that found marathon runners to be at greater risk of KSD. 29 Given that prolonged immobility and the resultant bone mineral loss are associated with KSD, 30 it serves that moderate exercise should be recommended for KSD patients.
Link to alcohol
While most of the clinical studies have not shown an increased risk of KSD development with increased alcohol intake, there exists disagreement as to whether alcohol consumption should induce stone formation or be protective. Siener found that subjects consuming alcohol excreted more calcium, which resulted in transient hypercalciuria that could lead to greater chance of calcium oxalate stone formation. 31 Animal studies have shown that rats treated with ethanol develop crystal formation. 32 Alcohol is also suggested to increase the production of uric acid and may contribute to uric acid stones. 33 In addition, alcohol consumption can cause oxidative stress to renal tissue, which can lead to lithogenesis. However, red wine contains antioxidants, and this could offset this harm. 34 Arguments for a protective role are largely derived from the dilution of metabolites in blood and urine. The known diuretic effect can increase urinary output, which is a protective factor and can reduce the risk of KSD. 35 In general, there are a limited number of clinical studies investigating this topic, given that alcohol consumption is lower in certain countries for cultural or religious reasons.
Link to smoking
Smoking is postulated to increase the risk of KSD through a multitude of factors. 23 One hypothesis is related to the increase in vasopressin levels, a strong antidiuretic, which can lead to poor urinary flow and a low urine output, which is further associated with greater risk of KSD. 36 Moreover, increasing levels of urinary metallic elements such as strontium and mercury, which are present in higher levels in smokers, may be of significance, but their relevance is inconclusive at present. 22,25 It was also found that smoking decreases the level of urinary calcium excretion, which is proven to be a risk factor of KSD. 36 Smoking also causes the release of reactive oxygen species and resultant oxidative stress on the kidneys. This renal injury can accelerate the onset of chronic kidney disease, which is an established risk factor for lithogenesis. Workers in certain construction industries who experience chronic exposure to cadmium are known to carry a higher risk of KSD. Cigarettes raise the plasma concentration of cadmium and this may also contribute to increased risk. 37
Strengths, limitations, and areas of future research
This is the first systematic review to assess different lifestyle factors, including smoking, alcohol, and exercise, and their impact on developing KSD. It has been prepared according to the Cochrane guidelines and PRISMA checklist, summarizing available data on this topic. It gives an overview of the studies on the link of KSD with lifestyle factors, although none of them was randomized control trials. Furthermore, a lack of heterogeneity of included studies precluded a formal meta-analysis. We could not establish or compare the level of activity, pack-years of smoking, units, and duration of alcohol intake from the studies. The possible presence of many uncontrolled or unknown confounding variables was also likely to impede proving direct causation of smoking, alcohol, and exercise. As well as possible selection bias, we also acknowledge the publication bias and that the conclusions drawn are only as robust as the included studies. Furthermore, some studies included only male or female patients, which is a further limitation on the possible conclusions.
One of the additional problems that are highlighted among many of the epidemiologic studies is that behavioral habits such as smoking and alcohol consumption are often coupled, and it is difficult to carry out subgroup analyses to separate these as independent risk factors. The nature of the assessment method in all studies using questionnaires introduces recall bias. Of particular relevance to this review is the role of social desirability bias as patients may have unconsciously underreported their smoking or drinking habits as well as overestimated physical activity. Rzewnicki and colleagues reported that overestimating physical activity in questionnaire studies is common. 38 Although no randomized studies exist, this would arguably be unethical to be done in the context of smoking and alcohol. An assessment of the association between warm weather, exercise, and hydration is perhaps also warranted. 39 Further longitudinal multicentric studies are still needed, however, to give further insight into additional factors such as exercise intensity, hydration levels, pack-years of smoking, units of alcohol consumed, and quality of life of these patients. 40 Future studies should also aim to investigate the relationship between the risk of stone formation and also the risk of stone recurrence.
Conclusion
While smoking is one behavioral factor that seems to have some association with KSD, no clear effect of alcohol has been demonstrated, and physical activity although helpful was negated by dehydration and hence increased the risk of KSD. To avoid KSD, awareness of the possible detrimental role of smoking should be considered and patients should remain vigilant about the importance of hydration with physical activity. While this represents the most appropriate guidance from the evidence available, at present there remain insufficient data to truly reveal the relationship between these three factors and KSD.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.