
Abstract
Purpose:
To report on the safety, technical results, and oncologic outcomes of computed tomography guided percutaneous microwave ablation of stage cT1b renal cell carcinoma.
Materials and Methods:
This single-center retrospective study investigated consecutive patients with T1b renal cell carcinoma who were treated with CT guided percutaneous microwave ablation between December 2015 and May 2019. Patient baseline characteristics, tumor biologic features, technical parameters, clinical outcomes, and complications were recorded and evaluated. Local tumor progression-free survival and overall survival rates were estimated using the Kaplan–Meier methods.
Results:
This study included 23 patients (18 men [mean age ± standard deviation, 74.6 years ±10.2; range 58–89 years] and 5 women [mean age, 71.6 years ±10.1; range 62–86 years]; overall mean age, 74.0 years ±10.0; range 58–89 years) with 23 T1b renal cell carcinomas. Primary technical success was achieved in 20/23 (87%) patients. Secondary technical success was achieved in 3/3 (100%) patients. Local tumor progression-free survival was 100.0%, 90.9%, and 90.9% at 1, 2, and 3 years, respectively. Overall survival was 95.2%, 85.7%, and 71.4% at 1, 2, and 3 years, respectively. There were 2 (8.7%) complications; both were classified as minor complications according to the Society of Interventional Radiology grading system.
Conclusions:
Computed tomography guided percutaneous microwave ablation for T1b renal cell carcinoma is associated with high rates of technical success, excellent local tumor progression-free survival, short-term survival and overall survival, and low complication rates.
Introduction
The incidence of small renal cell carcinoma (RCC) worldwide has increased in recent decades due to advances in abdominal imaging techniques and an aging population. 1,2 While partial nephrectomy (PN) is considered standard treatment for early-stage renal tumors, minimally invasive thermal ablation is a therapeutic option in select patients with early stage RCC, particularly in patients with significant comorbidities or those who are reluctant to undergo surgery. 3 Radiofrequency ablation (RFA) and cryoablation (CA) are the two most commonly used ablative technologies and have shown good clinical results in treating T1a renal tumors. 4,5 The American Urological Association currently recommends consideration of percutaneous thermal ablation with RFA and CA as alternative options to PN, radical nephrectomy (RN), or active surveillance for cT1a tumors <3 cm. 3 The same guidelines do not currently recommend percutaneous thermal ablation as an option for patients with T1b tumors, due to concerns of higher risk of recurrence or treatment failure. 3,6 While some emerging reports suggest that RFA and CA may be effective for T1b tumors, 7,8 the role of microwave ablation (MWA) for treatment of T1b tumors remains unclear. 9 The purpose of this study was to report on the safety, technical results, and short-term oncologic outcomes of computed tomography (CT) guided percutaneous MWA of stage T1b RCC.
Materials and Methods
The institutional review board approved this Health Insurance Portability and Accountability-compliant study.
Patients
An institutional database was used to retrospectively identify 23 adult patients with 23 biopsy-proven clinical stage T1b RCCs who were treated with CT-guided percutaneous MWA between December 2015 and May 2019 in our institution. All patients were seen in Urology and Interventional Radiology clinic and counseled on all treatment options, including PN, RN local thermal ablation, and surveillance. The decision to pursue thermal ablation was by consensus decision by Urology, medical oncology, and interventional radiology. The decision to use MWA, as opposed to other thermal ablative options, was at the discretion of interventionist performing the procedure. Before the ablation, the interventional radiologist reviewed preprocedure cross-sectional imaging to determine desired size of the zone of ablation based on tumor size and to determine whether a single or overlapping ablations were needed to create the planned ablation zone. In general, power settings of Watts and time were selected based on manufacturer recommendations that would create a zone of ablation that encompassed the tumor and extended a minimum of 5 mm beyond the tumor margins. In addition, preablation review of imaging was performed to determine if bowel was within 5 mm of the tumor margin in anticipation of possible hydrodissection to displace the bowel away to minimize the risk of nontarget organ injury, as previously described. 10 Similarly, if preprocedure imaging documented that the tumor was within 4 mm of the central collecting system, the procedures were planned to a Urologist present on the procedure day for temporary ipsilateral ureteral stent placement for pyeloperfusion during treatment, based on a previously reported technique for RFA of central RCC. 11 The number of cases in which hydrodissection and/or pyeloperfusion were used was recorded.
MWA procedures
All MWAs were performed by a board-certified interventional radiologist with more than 22 years of experience in image-guided percutaneous thermal ablation of renal masses. All ablations were performed using CT guidance (16-slice Lightspeed; GE Medical Systems, Madison, WI). MWAs were performed using a 14-gauge antenna that operates at 2.45 GHz (AMICA™; HS Medical, Boca Raton, FL). Patients were treated with monitored anesthesia care. The number of overlapping ablations was mainly dependent on tumor size, tumor location, and expected margins. The goal of all ablations was to create a circumferential ablative margin of at least 5 mm around the tumor. An immediate postprocedure unenhanced CT scan was performed to assess for immediate treatment response and periprocedural complications. Adjuvant methods of hydrodissection with dilute contrast (20 mL Isovue® 300 [Bracco Diagnostics, Monroe Township, NJ], in 1000 mL of 0.9% saline) or pyeloperfusion with a 5F ureteral stent were performed to minimize the potential risk of nontarget injury to adjacent structures. Tumor volumes before and after ablation were calculated according to the formula: V = 1/2(length × width 2 ). After treatment, all patients underwent nursing observation for 2–4 hours before discharge from the hospital.
Follow-up
The first imaging follow-up with contrast material enhanced CT or MRI was performed ∼4 weeks after MWA to assess technique efficacy and to evaluate for complications. Thereafter, patients were reevaluated with CT or MRI at ∼6 month intervals for 2 years, then yearly thereafter. Postprocedural measures included technical efficacy, complications, and local recurrence.
Data collection
Patient demographics (age, sex, race, body mass index, and Charlson comorbidity index), procedural data, complications within 30 days, technique efficacy, and survival were evaluated. The Charlson comorbidity index was adjusted for age. 12 Based on preablation imaging, tumor complexity was graded according to tumor size, location, involvement of the renal sinus, and nearness to collecting system (Radius, Exophytic/Endophytic, Nearness to the collecting system, Anterior/posterior, Location relative to the polar lines [R.E.N.A.L.] score and Preoperative Aspects and Dimensions Used for an Anatomical [PADUA] score). 13,14 Complications were classified from A to F based on the Society of Interventional Radiology grading system. 15 Pre- and postprocedure estimated glomerular filtration rate was recorded.
Definition of terminologies
Terminologies used to evaluate the treatment outcomes and complications of MWA were based on previously published classification guidelines. 16 Technical success of MWA was effective completion of the ablation as planned. Oncologic outcomes included local tumor progression-free survival and overall survival (OS). Local tumor progression was defined as the appearance of a new tumor with enhancement or the enlargement of the ablated tumor within the ablation zone.
Statistical analyses
Categorical variables were summarized as frequencies and percentages. Continuous variables were expressed as means and standard deviations or medians with ranges. A two-tailed two related samples nonparametric test was used to compare pre- and postablation tumor volumes. One-way analysis of variance or nonparametric test was used to compare ablation protocol and clinical results between different tumor complexities according to the R.E.N.A.L. score and PADUA scores, respectively. The Kaplan–Meier method was used for local tumor progression-free survival and OS analyses. A p value of <0.05 was considered indicative of a significant difference for all statistical tests. Statistical analyses were performed using the SPSS software program (version 22; IBM SPSS Statistics).
Results
Patient baseline characteristics and procedure data
A single MWA antenna was used to perform all ablations. Single-session treatments were performed in 19/23 (82.6%) patients, and two-session treatments were performed in 4/23 (17.4%) patients. Of the 23 patients, 21 (91.3%) had biopsy in a separate procedure before the ablation, and 2/23 (8.7%) patients were performed biopsy in the same procedure as the ablation. Demographic and clinical characteristics are summarized in Table 1. The median number of overlapping treatments was 3 (range 1–8). The median duration of every overlapping power application was 10 minutes (range 1–15 minutes), and the median generator output power was 60 W (range 40–80 W).
Demographic and Clinical Characteristics (n = 23)
PADUA = preoperative aspects and dimensions used for an anatomical; R.E.N.A.L. = Radius, Exophytic/Endophytic, Nearness to the collecting system, Anterior/posterior, Location relative to the polar lines; RCC = renal cell carcinoma; SD = standard deviation.
Mean tumor size was 5.2 cm (range 4.1–6.6 cm). Median tumor volumes were 42.0 cm3 (range 21.5–120.6 cm3) before ablation and 37.3 cm3 (range 9.4–141.5 cm3) after the last imaging follow-up, respectively. The tumor volume after ablation was significantly smaller than that before ablation (Z = −2.833, p = 0.005).
Follow-up
Technical success was achieved in all 23 tumors (100%). The median follow-up time was 16.6 months (range 1.5–43.5 months).
Oncologic efficacy
Primary technique efficacy was achieved in 20/23 (87.0%) patients (Fig. 1). Three patients (13.0%) with residual disease that was first identified at the 1-month follow-up imaging evaluation were retreated, with secondary technique efficacy of 100%. No cases of metastatic disease or ablation-related deaths were identified. Four patients died from non-RCC related causes. Local tumor progression was identified in one patient at 17.5 months after the procedure. The 1-, 2-, and 3-year local tumor progression-free survival was 100.0%, 90.9%, and 90.9%, respectively (Fig. 2). The 1-, 2-, and 3-year OS was 95.2%, 85.7%, and 71.4%, respectively (Fig. 3).
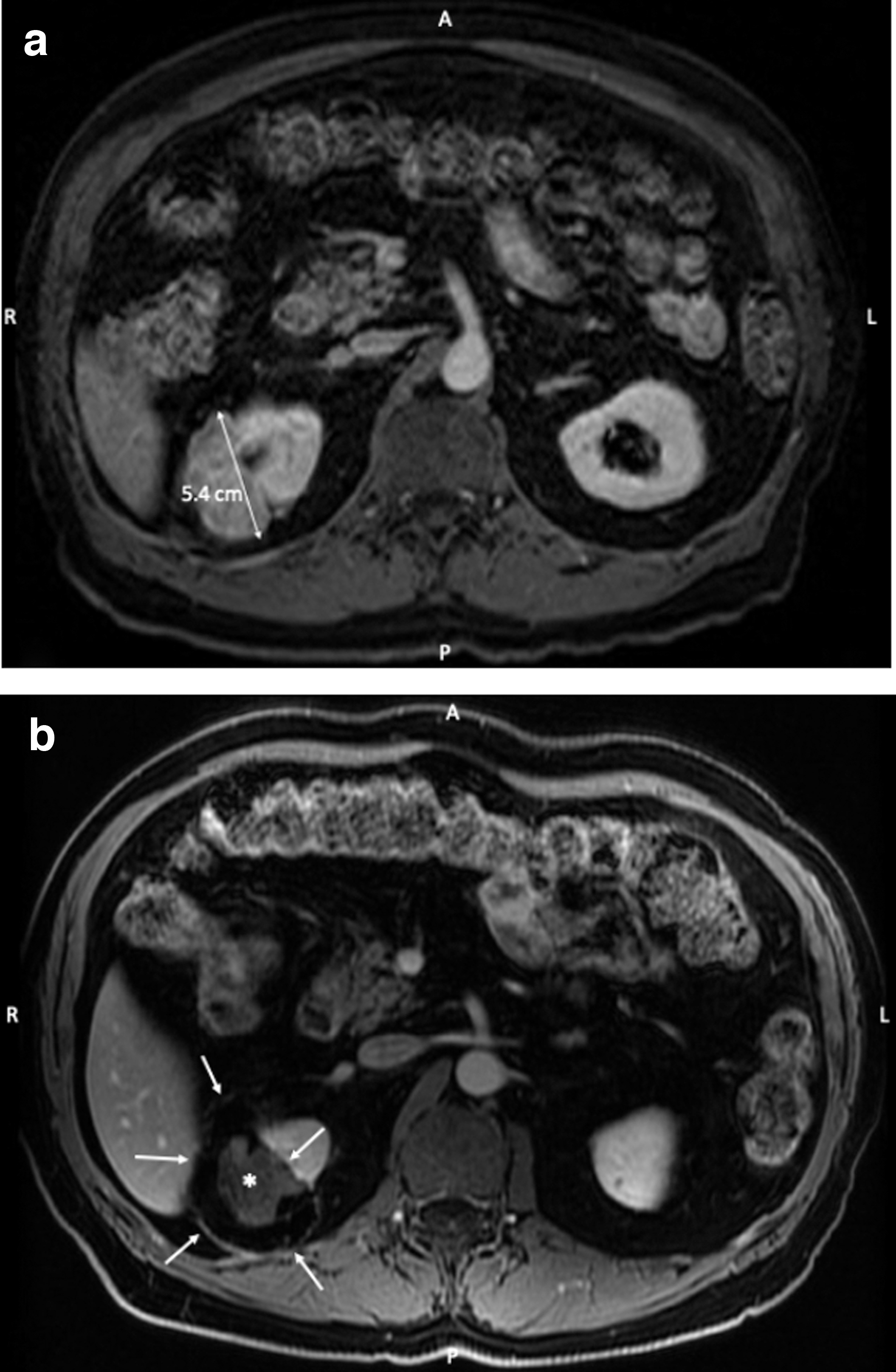
Images of a 75-year-old man with right renal cell carcinoma.
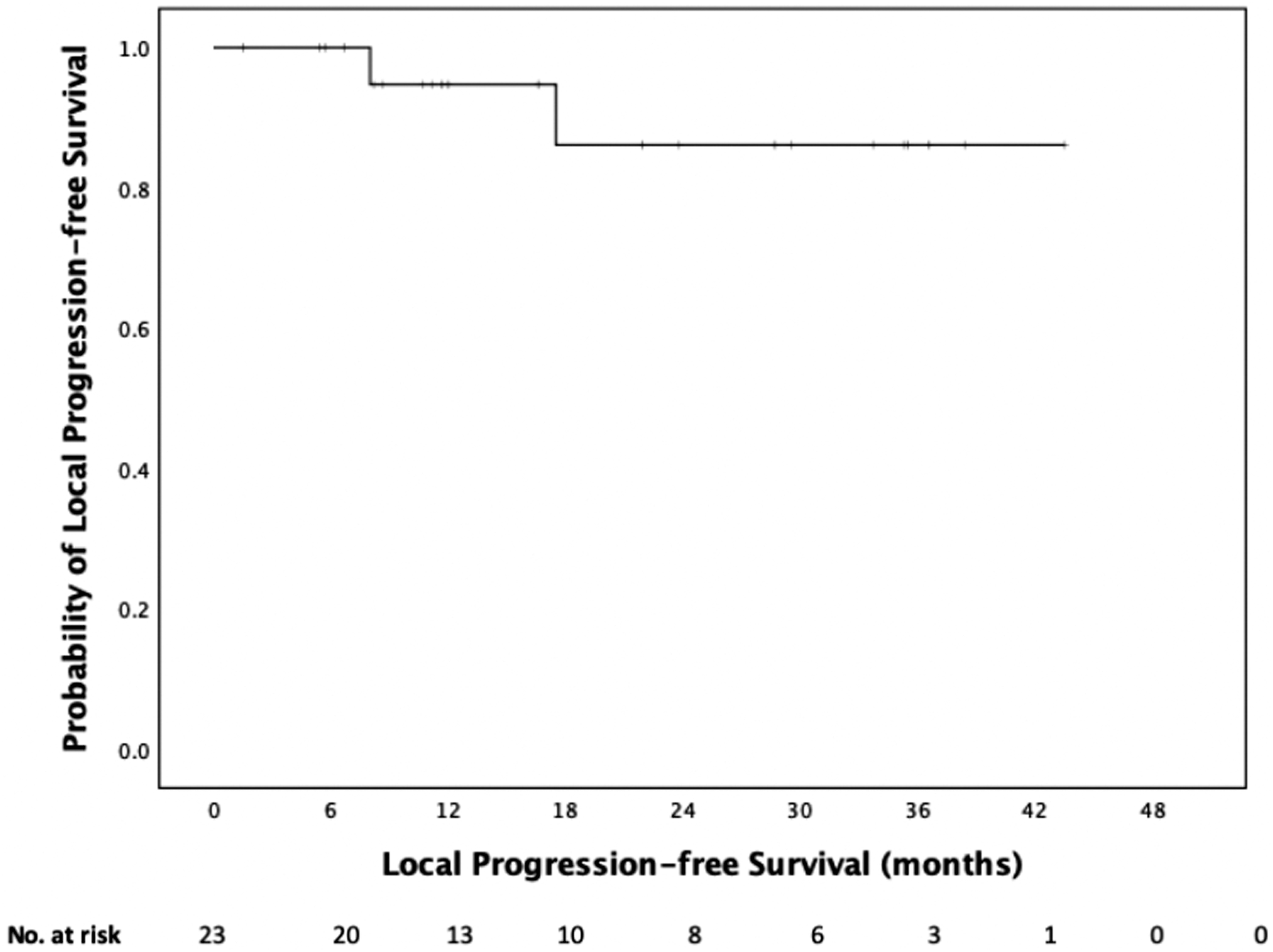
Kaplan–Meier curve demonstrating local tumor progression-free survival.
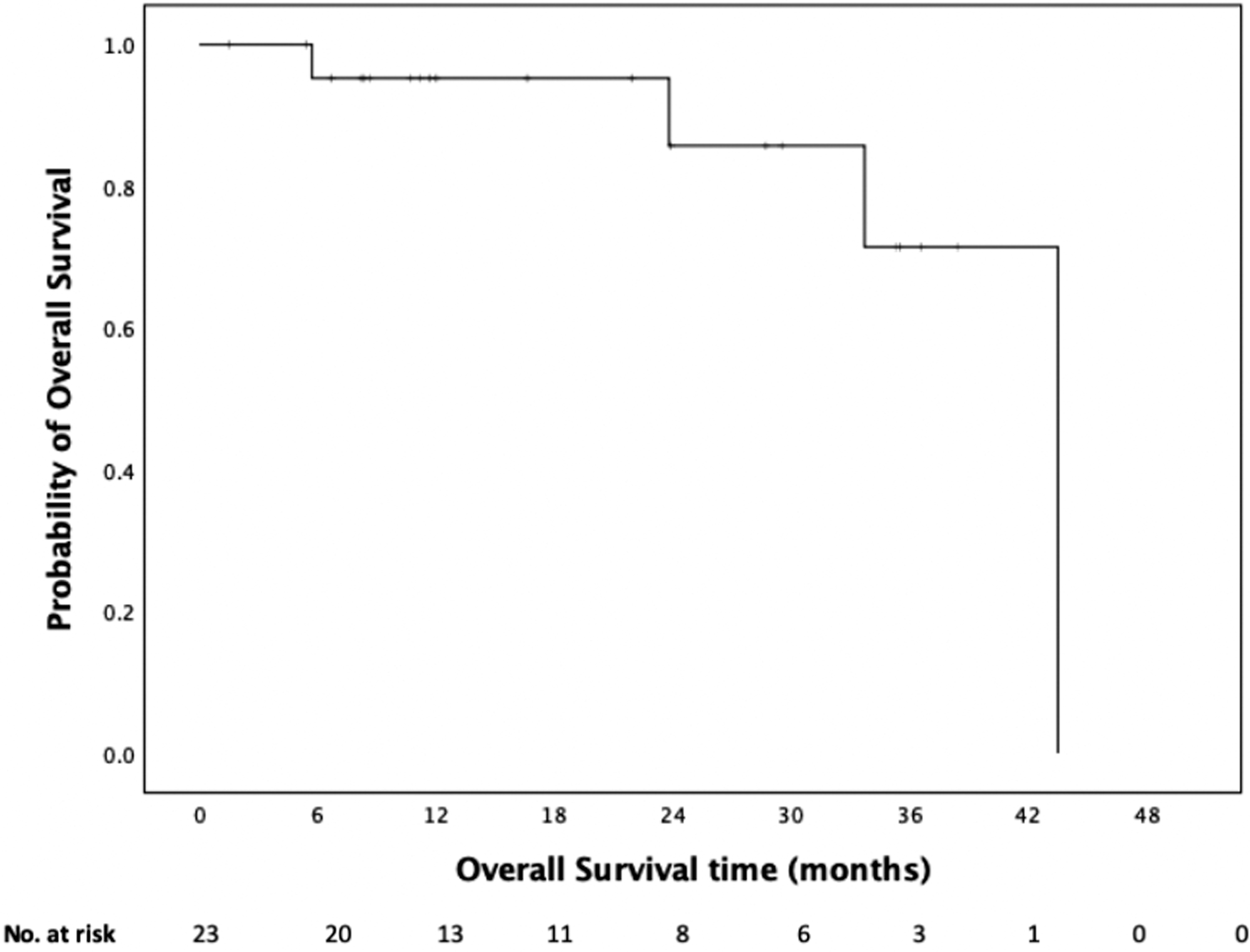
Kaplan–Meier curve demonstrating overall survival.
Complications
There were 2/23 (8.7%) minor complications (Class A and B). One patient developed an asymptomatic subcapsular hematoma, which was identified on the first CT scan 1 month after the procedure. The other patient who was on coumadin for atrial fibrillation developed a retroperitoneal hematoma within 24 hours after the ablation procedure and was admitted overnight for hemodynamic monitoring, as well as pain and blood pressure control. There were no class C–F complications.
Tumor complexity analysis
Based on R.E.N.A.L .and PADUA scores, there were similarities in the percentages of low complexity (26.1% vs 21.7%), moderate complexity (56.6% vs 52.2%), or high complexity (1724% vs 26.1%) tumors, respectively. No significant differences were noted with regard to tumor diameter and pre- and postablation tumor volumes between low, moderate, and high complexity tumors with either scoring system. Similarly, no differences between R.E.N.A.L. and PADUA scores were noted in terms of number of overlapping ablation, generator output, tumor ablation time, complication rates, or local tumor progression (Tables 2 and 3).
Tumor Complexity (R.E.N.A.L. Score): Ablation Protocol and Clinical Results
Compared using one-way analysis of variance test.
Compared using nonparametric two-independent samples test.
Compared using χ 2 test.
Tumor Complexity (PADUA score): Ablation Protocol and Clinical Results
Compared using one-way analysis of variance test.
Compared using nonparametric two-independent samples test.
Compared using χ 2 test.
Discussion
The results of the present study show overall favorable oncologic outcomes for patients with T1b RCC treated with CT-guided percutaneous MWA. The local tumor progression-free survival reported in the present study of 100.0%, 90.9%, and 90.9% at 1-, 2-, and 3-year follow-up compare favorably with a cohort of nine patients with T1b RCC treated with percutaneous MWA reported by Wells and colleagues, who found no short-term local tumor progression. 17 Similarly, Gao and colleagues evaluated the efficacy of ultrasound guided percutaneous MWA of RCC adjacent to the renal sinus, including 12 T1b tumors. 18 The results of that study found that the estimated 1-, 3-, and 5-year disease-free survival was 97.0%, 81.8%, and 70.0%, respectively, 18 which are similar to results reported in the present study. In addition, the 1-, 2-, and 3-year OS was 95.2%, 85.7%, and 71.4%, respectively, in the study. Compared to CA for T1b RCC, the results of the present study show similar short-term local tumor control rates, 19 –21 suggesting that MWA is as effective as the more commonly reported CA for T1b RCC.
Radical nephrectomy remains the standard of care for treatment of T1b RCC [20 = 2]. The present study also compares favorably to reported 94% recurrence-free survival with nephron sparing surgery or laparoscopic RN. 22 –24
The results of the present study suggest that MWA may be a viable treatment option for larger renal tumors. Thermal ablation of T1b tumors is currently not recommended by available guidelines due to concerns of higher rates of local recurrence than PN. 3,25 –27
The American and European Urological Associations only advise RFA or CA as an alternate therapy only for unfit surgery patients with T1b RCC because of local recurrence following percutaneous treatment. 3,28 A previously published randomized controlled trial comparing open PN, laparoscopic PN, open MWA, and laparoscopic MWA showed that there was no difference in local recurrence-free survival with fewer complications with MWA compared to PN. 29 The present study suggests that similar outcomes may be achieved with the less invasive means of percutaneous access and faster recovery times. Comparison between PN and percutaneous MWA is difficult. However, local recurrence rates may not reduce the application of MWA for larger renal tumors, because repetitive ablation can improve efficiency and reduce the local recurrence-free rates. A recent meta-analysis showed that repetitive ablation could significantly improve the recurrence-free survival of thermal ablation compared to PN. 30
While MWA of T1b RCC can present more technical challenges based on tumor size, the present study shows that percutaneous CT-guided MWA of larger tumors can achieve a high rate of technical success (100%). In addition, the number of overlapping ablations, generator output, duration of ablation, local tumor progression rates, and complication rates were similar for low, moderate, and high tumor complexity in our study. The results of this study show that MWA is likely less affected by tumor size and complexity compared with RFA and CA. As reported in previous studies, there were many factors that may affect the technical success of RFA and CA, such as tumor size, location and relationship with renal sinus, and collecting system. 31,32 Some studies suggest that RFA and CA may be associated with more technical failure for treatment of larger tumors or more complex tumors. 32,33
The present study also found that the postablation tumor volume was significantly smaller than the preablation tumor volume. The presumed reasons are dehydration and collagen shrinkage in the tumors. Fewer complications may be an advantage of percutaneous MWA, compared with more invasive techniques. 34 In the present study, the overall rate of complications was not affected by tumor size or complexity.
There are also some limitations in the present study. First, the retrospective and single-center nature of this study is a limitation associated with inevitable technical and personnel bias. This is compounded by the use of a single manufacturer; thus, the results may not be generalizable to all microwave devices. Second, even though this study achieved good clinical and technique outcomes, it is still limited by a small sample size. Third, the small sample size limits that strength of the complexity analysis. A larger cohort would be required to further assess the impact of tumor complexity on outcomes. Furthermore, the short-term follow-up and noncontrol design were limited to assess the long-term clinical outcomes and objective efficacy compared with other options.
Conclusion
This study shows that CT-guided percutaneous MWA shows good oncologic outcomes and is associated with few complications when used to treat cT1b RCC. While these results are encouraging, additional clinical trials are necessary to carefully evaluate the long-term clinical and oncologic outcomes, as well as safety, to better define this technology as a potential thermal ablation option for treatment of cT1b RCC.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was provided for this article.