
Abstract
Introduction:
Nephrolithiasis is a known risk factor for chronic kidney disease (CKD); however, it is unknown how CKD affects urinary parameters related to stone risk. The purpose of this study was to assess the relationship of diminishing glomerular filtration rate (GFR) and kidney stone-related 24-hour urine (24H urine) composition.
Materials and Methods:
A single-institution retrospective review of patients (n = 2057) who underwent 24H urine analysis was performed. The serum creatinine within 1 year of the first 24H urine was used to determine estimated GFR and stratify patients by CKD stage. We performed analysis of variance and multivariable linear regression to assess the relationship of GFR and urinary analytes.
Results:
Among all patients, there were 184 (8.9%), 1537 (74.7%), 245 (11.9%), 70 (3.4%), 17 (0.8%), and 4 (0.2%) in CKD stage I, II, IIIa, IIIb, IV, and V groups, respectively. On analysis of 24H urine composition, as CKD increased, changes in urinary parameters protective against crystallization included decreased calcium and uric acid (UA) (P < 0.001). In addition, parameters favoring crystallization included decreased citrate and magnesium (P = 0.002 and P < 0.001, respectively). The net effect with increasing GFR was decreasing supersaturation of calcium oxalate and phosphate. On linear regression, urinary excretion of calcium, oxalate, citrate, UA, phosphate, and ammonia all decreased with decreasing GFR (all P < 0.05).
Conclusions:
Higher CKD stage was associated with changes in urinary analytes that both promoted and inhibited stone formation, with the net effect of decreasing calcium oxalate and phosphate supersaturation. These patients may benefit from medical therapy that targets improving urinary citrate instead of lowering calcium or UA.
Introduction
Chronic kidney disease (CKD) and nephrolithiasis are increasingly common diseases worldwide with prevalence estimates of 13% 1 and 2%–15%, respectively. 2,3 Although the causes of CKD vary globally, diabetes and hypertension represent the main causes with the former projected to account for as much as 69% of CKD cases by 2030. 4
Comparatively, nephrolithiasis is a rare cause of end-stage renal disease (ESRD). Of the over 70,000 patients diagnosed with ESRD in the United States in 2017, only 12,048 (1.7%) have been because of urologic causes. 5 Among stone formers, the development of ESRD is similarly very rare with an estimated incidence of 3 in 100,000 stone formers. 6 Nephrolithiasis has been shown to be a risk factor for the development of CKD 7,8 ; however, it is unclear whether this is because of shared risk factors 9 –11 or other factors such as medication use, recurrent obstruction, or surgical interventions. 12 –16
The 24-hour urine (24H urine) test as a part of a comprehensive metabolic evaluation is recommended in high-risk kidney stone formers to identify modifiable risk factors and potentially select interventions to reduce risk of future stone events. 17 It is assumed that tested individuals have sufficient renal function to resorb and excrete analytes of interest. However, there is a paucity of data on how the 24H urine test should be interpreted among patients with varying levels of estimated glomerular filtration rate (eGFR) and how eGFR deterioration relates to risk of nephrolithiasis. A prior single-institution review showed decreased GFR was associated with reduced urine calcium, oxalate, citrate, and supersaturation of calcium oxalate and phosphate; however, the study included mostly patients with mild CKD. 18 If urine analyte excretion decreases with worsening CKD, there may be a need for GFR-specific cutoffs in 24H urine studies. This in turn may affect what dietary, behavioral, or medical interventions should be offered to patients with CKD. Utilizing our institution's cohort of kidney stone formers, we sought to examine how CKD impacts 24H urine composition.
Methods
Patient cohort
Our study was approved by our institutional ethics board (#181182). All patients seen in our urology clinic who completed a 24H urine study at our institution between 2006 and 2017 (n = 3625) were included. Urine testing was performed by a specialized laboratory (Litholink Corporation, Chicago, IL). For patients with multiple 24H urine studies, only the first was included. We then used an automated data extraction tool, in addition to manual chart review, to abstract demographic, clinical, and laboratory information on our cohort from the electronic medical record. 19,20 Only patients with a creatinine measurement within 1 year of their 24H urine were included. If there were multiple creatinine values, then the temporally closest value to the time of 24H urine was used.
The Modification of Diet in Renal Disease Study equation was used to calculate eGFR 21 and patients were categorized by their CKD stage. 22 All patients with CKD stage IIIb or higher were manually reviewed to ensure that the captured GFR remained persistent and was not because of a transient rise from obstruction. We excluded patients with inadequately collected samples (24-hour creatinine <800 mg for men and <600 mg for women). Our final cohort comprised n = 2057 individuals.
Outcomes
Our primary objective was to identify 24H urine parameters that were associated with decreasing eGFR (or increasing CKD stage). Our secondary objective was to examine the associations between clinical, demographic, and stone characteristics with CKD stage.
Demographic information included age at urine testing, sex, body mass index (BMI), and race. Clinical characteristics extracted using ICD-9 and ICD-10 codes included history of inflammatory bowel disease, recurrent diarrhea, hypertension, gout, type 2 diabetes, osteoporosis, immobility, hyperparathyroidism, coronary artery disease, myocardial infarction, cerebrovascular accident, hyperlipidemia, gastroesophageal reflux disease, epilepsy, or migraine (Supplementary Table S1). In addition, we assessed whether subjects were prescribed any of the following medications at the time of 24H urine submission: potassium citrate, allopurinol, hydrochlorothiazide, indapamide, and chlorthalidone.
As not all patients underwent stone treatment, kidney stone composition was available in n = 1218 (59.2%) patients and classified by the highest percent component. These included calcium-oxalate monohydrate (COM) and calcium-oxalate dihydrate (COD), hydroxyapatite, uric acid (UA), and other (struvite, brushite, carbonate apatite, and ammonium urate).
We extracted 24H urine volume, calcium, oxalate, citrate, UA, sodium, potassium, magnesium, pH, phosphorous, chloride, sulfate, nitrogen, creatinine, and creatinine per kilogram. The supersaturation index of calcium oxalate (SSCaOx), calcium phosphate (SSCaP), and uric acid (SSUA) was also measured.
Analysis
Data were analyzed to detect differences between CKD stages. Continuous variables were analyzed with Students' t-tests or analysis of variance. Categorical variables were analyzed with chi-square test. Pairwise comparison of means by CKD stage was performed for select 24H urine analytes. Multivariable linear regression models were created to assess the association between eGFR and 24H urine analytes. These models were adjusted for risk factors of stone disease, including age, race, BMI, sex, and medical history of hypertension, coronary artery disease, type 2 diabetes, hyperlipidemia, and gastroesophageal reflux disease. To account for dietary acid ash content, we examined the difference of urinary ammonium to urinary sulfate (NH4-SO4). 23 A two-sided P-value of <0.05 was considered statistically significant. All analyses were performed using SPSS v25.
Results
Our cohort of n = 2057 patients included 184 (8.9%), 1537 (74.7%), 245 (11.9%), 70 (3.4%), 17 (0.8%), and 4 (0.2%) in CKD stage I, II, IIIa, IIIb, IV, and V groups, respectively. Thirty-five patients, 20%, 65.7%, 5.7%, and 8.6% of whom were in CKD stage I, II, IIIa, and IIIb, were excluded based on Cr-specific cutoffs, which were not significantly different than the study cohort (P = 0.105). Compared to patients in CKD stage I/II, patients in higher stages were older and more likely to have a history of hypertension, gout, type 2 diabetes, coronary artery disease/history of myocardial infarction, cerebrovascular accident, and hyperlipidemia (all P < 0.001, Table 1). These patients also had a higher proportion on allopurinol and no differences in thiazides or potassium citrate use.
Demographic and Clinical Characteristics of the Study Cohort
BMI = body mass index; eGFR = estimated glomerular filtration rate.
On univariate analysis of 24-hour urine composition (Table 2), there was no difference in urine volume detected. However, with increasing CKD stage, both urinary creatinine and the adjusted creatinine per kilogram per day measures decreased (Fig. 1). Additional changes that were protective against crystallization with advancing CKD stage were decreases in calcium and UA (Fig. 1). Factors that favored crystallization included decreases in citrate and magnesium as CKD stage worsened. The net effect appeared to be decreased supersaturation of calcium oxalate and phosphate with no effect on UA supersaturation. (Fig. 2).
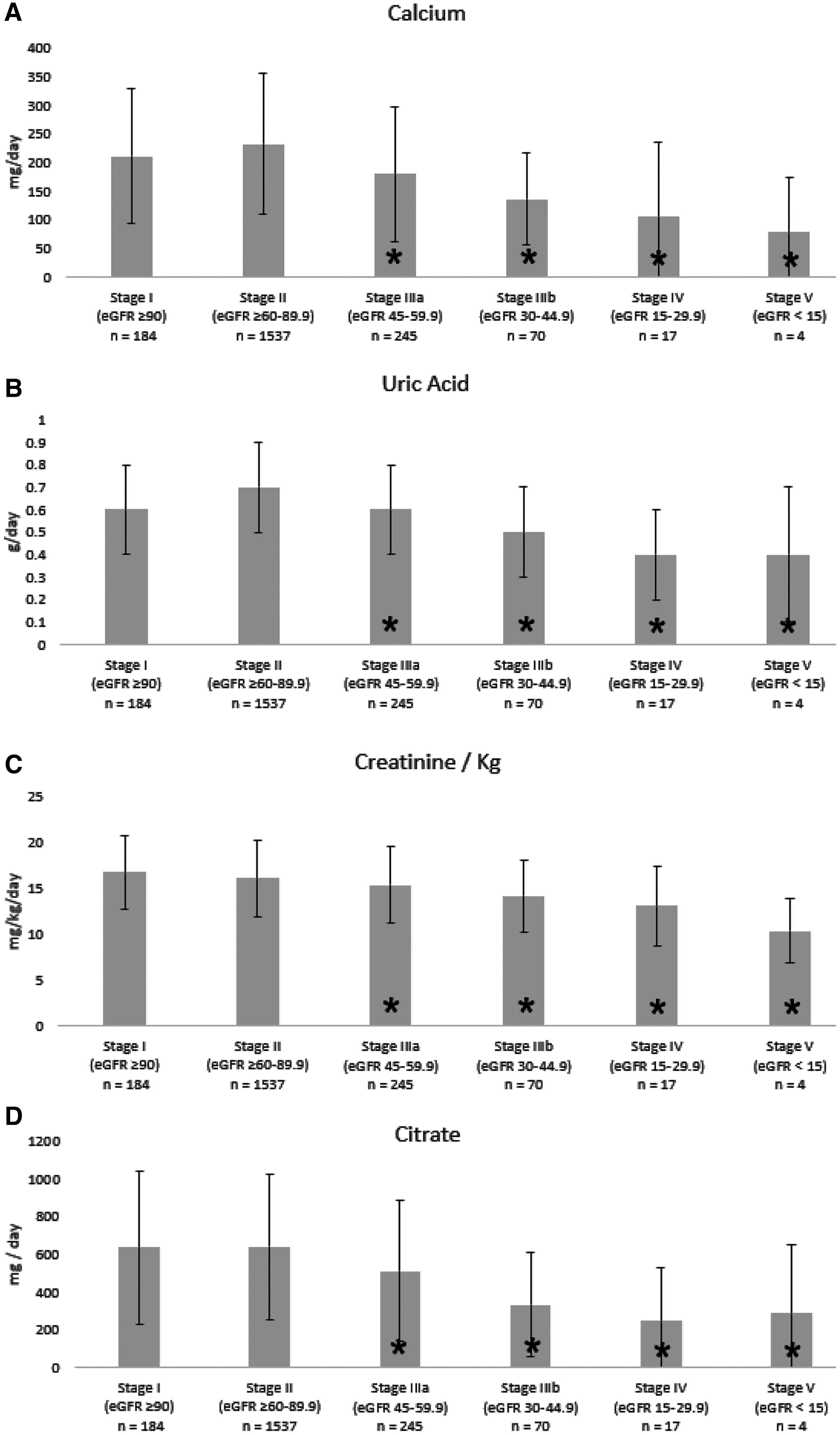
Changes in urinary

Supersaturation of
Comparison of 24-Hour Urine Analytes Across Chronic Kidney Disease Stages
Stone composition data were available in 59.2% (N = 1218) of patients (Table 1). The median time between 24H urine study and stone analysis was 94 days (IQR 45–374 days). COM stones were the most common across the CKD spectrum followed by hydroxyapatite. In stage IIIa and above, there was a higher proportion of UA stones and a lower proportion of COD and other stones.
On multivariable linear regression between eGFR and 24H urine analytes controlling for demographic and clinical cofounders, the supersaturation of both calcium oxalate (β = 1.077, 95% CI 0.740–1.413) and calcium phosphate (β = 3.253, 95% CI 1.999–4.508) was found to be significantly lower with decreasing GFR (Table 3). We found that excretion of urinary calcium, citrate, UA, phosphatem and ammonia also decreased with decreasing GFR. Urinary ammonium remained significant, even when correcting for dietary acid ash content (NH4-SO4).
Multivariable Linear Regression of 24-Hour Urine Analytes Controlling for Demographic and Clinical Factors
Models adjusted for age, race, BMI, sex, hypertension, coronary artery disease, type 2 diabetes, hyperlipidemia, and gastroesophageal reflux disease
SSCaOx = supersaturation index of calcium oxalate; SSCaP = supersaturation index of calcium phosphate; SSUA = supersaturation index of uric acid.
Discussion
In our study, we found that with worsening CKD stage excretion of most urinary analytes decreased, with concomitant decrease in supersaturation of calcium oxalate and phosphate. Patients at higher stages of CKD have several factors that are protective against crystallization such as lower urinary calcium and UA. However, there were also lower levels of urinary citrate and magnesium, which favor crystallization. The net effect of this, however, appeared to be a decrease in the supersaturation of calcium oxalate and phosphate with no effect on the supersaturation of UA.
In practice, these patients with CKD and nephrolithiasis, who receive pharmacologic preventative therapy, may benefit from medications or interventions directed at increasing urinary citrate rather than pharmacologic interventions aimed at decreasing urinary calcium or UA. Supplementation must be performed with care in renal failure, however, as potassium citrate may increase serum potassium. Increasing urinary magnesium may also be a target; however, supplementation must be cautious in renal failure.
We did not detect a difference among CKD stages for urine volume, for which low urine volume is a consistent risk factor for stone recurrence. In addition, our finding of decreased urine creatinine and creatinine per kilogram per day with advancing CKD stage may point to a need for eGFR- or creatinine-specific cutoffs, although our excluded patients were not skewed toward higher or lower stages. We did find an increased proportion of pH-related stones in advanced CKD, likely driven by the decrease in pH with worsening GFR, although this was only demonstrated on univariate and not multivariate analysis.
Our study is largely consistent with prior studies and we report the largest cohort of patients across CKD stages, including 357 patients in stage III or above. 18,24,25 A prior study examined the in vitro total inhibitory activity of urine samples in 20 patients with renal failure compared to 11 healthy controls. 24 They found CKD was associated with lower urine creatinine, calcium, phosphorus, magnesium, sodium, chloride, potassium, and UA. These were similar to our findings, although we did not detect any difference in urine sodium (although it approached significance). This may be because of differences in dietary habits or sample size.
A prior review of 403 stone formers from 2 metabolic stone clinics also found significantly reduced urinary calcium, citrate, and supersaturation of calcium oxalate and phosphate. 18 However, our findings differed in several ways. We found that urinary magnesium decreased with worse CKD stage and a higher proportion of UA and hydroxyapatite stones in patients with advanced CKD. These differences may be explained by sample size as this review only included 80 patients with stage III CKD or above (only 1 of whom was stage IV) compared to our analysis of 336 patients with stage III CKD and 21 who were stage IV and V. Another study retrospectively reviewed 3266 stone formers, 115 of whom had solitary kidneys. 26 They found that patients with solitary kidneys had increased loss of renal function and on 24-hour urine analysis had lower urine calcium and lower supersaturation of all three stone-forming salts. Urinary ammonium has also been demonstrated to decrease with advancing CKD. 27
There is a growing body of epidemiologic evidence linking CKD and nephrolithiasis. 8,12,28 The development of CKD and nephrolithiasis is multifactorial with shared risk factors, including hypertension, obesity, dyslipidemia, and diabetes. 7,9 –11 Other mechanisms for this association include medications, recurrent urinary tract infections, surgical management, or recurrent obstruction. 7,12 –15 Regardless of the mechanism, stone formers have been observed to have worse renal function when compared against non-stone formers. 25,29 A case–control study examined the risk of developing CKD in 4774 stone formers in Olmsted County, Minnesota. 30 They found that not only was the risk for clinical diagnosis of CKD 50%–67% higher among stone formers but also the risk of sustained reduced eGFR was 22%–42% higher, independent of CKD comorbidities. Another study found an increased risk of ESRD in recurrent symptomatic vs incident symptomatic stones, 16 suggesting that recurrent stones may lead to incremental kidney injury with each stone event. However, our data would suggest that as CKD progresses, stone risk may decrease. Additional study is needed to confirm these findings, which would help inform the appropriate intensity of stone-preventative interventions among patients with advanced CKD.
Our study has several limitations. As a retrospective review of a tertiary care center, our patient cohort was subject to selection bias and likely comprised higher risk patients with kidney stone disease. Only each patient's first 24H urine was included, which would not capture changes in metabolic state over time. In addition, we could not assess the impact of diet, especially specialized diets in advanced CKD, which may have modified patients' 24H urine parameters independent of GFR. Although it is possible that transient decreases in eGFR may have been attributable to obstruction, we sought to address this limitation by manual review of selected patient medical records. Our patient population was also relatively homogenous and these data may need to be replicated in other racial groups. Finally, these findings may not be generalizable to patients with CKD and without kidney stones.
Conclusion
Although worse CKD was associated with changes in urinary analytes that both promoted and inhibited crystallization, the net effect was decreased supersaturation of calcium oxalate and phosphate. In practice, these patients may benefit more from medical therapy that targets urinary citrate or magnesium instead of lowering urinary calcium or UA. In addition, there may be a role for creatinine- or eGFR-specific cutoffs for 24H urine tests in patients with CKD.
Footnotes
Acknowledgment
The authors acknowledge Litholink/Lapcorp for data sharing.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
The project described was supported by CTSA award No. UL1TR000445 from the National Center for Advancing Translational Sciences. Its contents are solely the responsibility of the authors and do not necessarily represent official views of the National Center for Advancing Translational Sciences or the National Institutes of Health.
Supplementary Material
Supplementary Table S1
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.