
Abstract
Purpose:
To systematically explore the superiority of the transperitoneal approach in robot-assisted partial nephrectomy (TP-RAPN) and retroperitoneal approach in robot-assisted partial nephrectomy (RP-RAPN).
Methods:
Several databases were searched including PubMed, EMBASE, Cochrane Library, Web of Science, CNKI, CBM, Wan Fang, and VIP to identify relevant studies that reported the comparison of the TP-RAPN and RP-RAPN. Outcomes of data were pooled and analyzed with Review Manager 5.3 to compare the intraoperative and postoperative variables and postoperative complications. Based on the heterogeneity of the studies, odds ratios (ORs) and weighted mean differences (WMDs) with 95% confidence intervals (CIs) were calculated using a random-effect model or fixed-effect model. The sensitivity analysis and the subgroup analysis were used to minimize the effects of heterogeneity. And, publication bias was assessed by funnel plots.
Results:
In all, 16 studies met the inclusion criteria, including 2336 TP-RAPN patients and 1705 RP-RAPN patients. This meta-analysis reviewed 16 studies on RAPN, and the RP-RAPN showed shorter operative time (OT) (WMD 13.18 minutes; 95% CI 5.04–21.31; p = 0.001), shorter postoperative bowel function recovery (WMD 1.97 days; 95% CI 0.43–3.52; p = 0.01), shorter length of stay (LOS) (WMD 0.51 days; 95% CI 0.25–0.77; p = 0.0001), and lower estimated blood loss (EBL) (WMD 7.08 mL; 95% CI 1.41–12.74; p = 0.01) than the TP-RAPN. Additionally, no significant differences were found in other outcomes.
Conclusions:
In comparison, the RP-RAPN had significantly shorter OT, postoperative bowel function recovery time, LOS, and lower EBL. The RP-RAPN is associated with better value for posterior and laterally located tumors and is faster and equally safe and low costs for the patient.
Introduction
Renal cell cancer (RCC) is one of the common malignancies of the urinary system, representing 2% to 3% of all cancers. The morbidity of RCC varies worldwide, is higher in developed countries than in developing countries, and predominates in men, with the male-to-female ratio being 1.5:1.0. 1 At present, RCC is still one of the deadly malignant tumors of the urinary system. But the diagnosis and treatment of RCC obviously improved in the past two decades. With the development and popularization of imaging diagnostic techniques, the detection rate of renal masses has risen. Surgery has always been the main treatment choice for localized renal tumors. Partial nephrectomy (PN) is considered the “gold standard” surgical treatment of option for clinical T1-stage renal tumors and small renal masses. 2,3
The robot-assisted laparoscopic surgery system is widely increasingly being used in surgical treatment and has been shown to be safe and effective in renal tumors. 4 Compared with traditional laparoscopic surgery, robot-assisted partial nephrectomy (RAPN) has the advantages of good three-dimensional magnification and stereoscopic vision, extremely flexible manipulative robotic arm, stable camera, and easy operation. It can perform tumor resection and suture efficiently and safely, with less intraoperative estimate blood loss and shorter length of hospital stay. 5,6
RAPN can be performed via the transperitoneal approach in robot-assisted partial nephrectomy (TP-RAPN) or retroperitoneal approach in robot-assisted partial nephrectomy (RP-RAPN). Each approach has its own advantages and limitations, but without definitive evidence on which is the most appropriate approach for RAPN. The final selection of the surgical approach in clinical seems to be more the location and size of the tumor, personal expertise. 7 Therefore, it is necessary to carry out a meta-analysis to systematically explore the superiority of the TP-RAPN and RP-RAPN. We performed a meta-analysis of the published literature to compare the intraoperative and postoperative outcomes of two surgical approaches, providing evidence-based medical evidence for the selection of surgical approaches of PN for early renal tumors. Meanwhile, we scrupulously assessed the methodology and outcome reporting of the publishing literature in this field.
Materials and Methods
This meta-analysis was carried out in accordance to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) declarations, including the literature search strategy, inclusion and exclusion criteria, data extraction, and statistical analysis.
8
The protocol of this systematic review was published on the PROSPERO register (
Search strategy
Several databases were searched including PubMed, EMBASE, Cochrane Library, Web of Science, CNKI, CBM, Wan Fang, and VIP to identify relevant studies that reported the comparison of the TP-RAPN and RP-RAPN. We used the following search terms: (robot OR robot-assisted OR robotic OR robotic-assisted OR DaVinci) [Title/Abstract] AND (partial nephrectomy OR PN OR nephron-sparing surgery OR NSS OR nephrectomy)[Title/Abstract] AND (transperitoneal OR retroperitoneal)[Title/Abstract] (Supplementary Data). In addition, the reference lists of relevant articles were manually searched to identify related articles. The latest date of the search was on March 2, 2020.
Inclusion criteria and exclusion criteria
The following inclusion criteria were used: (1) The literature types are randomized controlled trials, case–control studies, retrospective matched-pair study design, and comparative studies from well-defined registries or databases. (2) The literature is about the comparison between the TP-RAPN and RP-RAPN. (3) Relevant outcome indicators are reported in the studies. (4) The literature was published in English or Chinese. The following exclusion criteria were used: studies were excluded for failing to meet one or more of the inclusion criteria.
Study selection and data extraction
Two reviewers identified the included studies and extracted data via reading full-text articles, respectively. The disagreement was resolved by discussion and negotiation until consensus. Sixteen studies published from 2013 to 2020 fulfilled the inclusion criteria and were included in the meta-analysis.
Extracted data included first author, year of publication, country, study design, inclusion and exclusion criteria, the number of patients in each group (no. of patients), average age, gender, patient body mass index, tumor size (average diameter), tumor location (anterior, posterior; hilar; upper pole, interpolar, lower pole), tumor side (right, left, bilateral), R.E.N.A.L. score, American Society of Anesthesiologist score, and outcomes indicators. We contacted the corresponding authors for the data that were missing or incomplete in the literature, but no one provided any additional information. Unavailable or incomplete data of the study were included in the review, not into the meta-analysis.
Comparison of outcome indicators in TP-RAPN and RP-RAPN
Intraoperative variable: operative time (OT), warm ischemia time (WIT), estimated blood loss (EBL), and conversion rate.
Postoperative outcomes: length of stay (LOS), estimated glomerular filtration rate (eGFR), and postoperative bowel function recovery.
Complications: overall complications and major complications (the Clavien–Dindo classification ≥3) and intraoperative complications.
Oncologic outcomes: positive surgical margin (PSM) rate, recurrence rate, and survival rate.
Quality assessment of studies
An assessment of the methodological quality of included studies was assessed independently by two authors (S.G. and L.C.) according to the Newcastle–Ottawa Scale, with some appropriate modifications to match this study. 9 The quality assessment of studies included three aspects: study group selection, comparability between groups, and outcome indicators. Zero to 2 points for each item, the full score is 9 points, studies achieving a score of ≥7 scores were considered to be of high quality.
Data analysis
This meta-analysis was performed according to the Quality of Reporting of Meta-analyses guidelines of the Cochrane collaboration. 10 The weighted mean differences (WMDs) and odds ratios (ORs) with 95% confidence intervals (CIs) were used to compare continuous and dichotomous variables, respectively. The continuous variables of studies that only reported the mean value has been included in the meta-analysis in the present study.
The chi-square test was used for the statistical heterogeneity test. The quantity of heterogeneity was evaluated using the I 2 statistic. A random-effects (RE) model was used to pool the results of studies with high heterogeneity (p < 0.10, I 2 > 50) between studies. Otherwise, a fixed-effects (FE) model was used. 11 We used the sensitivity analysis by excluding studies with at least one domain of adjudicative high risk of bias to minimize the effects of heterogeneity. Funnel plots were used to examine the existence of publication bias. All statistical analyses were performed using Review Manager Version 5.3, and all tests were two-sided with a significance level set at p < 0.05 (α = 0.05).
Results
Description and basic characteristics of the included studies
The literature selection flowchart is shown in Figure 1. In all, 934 records were identified after the initial database search. After screening, 16 studies 12 –27 consisting of 4041 patients (TP-RAPN: 2336 patients; RP-RAPN: 1705 patients) were considered as satisfied eligible studies, including 12 English literatures 12 –16,19–25 and 4 Chinese literatures. 17,18,26,27 All included studies were retrospective observational studies. A summary of the main characteristics of those available studies are listed in Table 1.
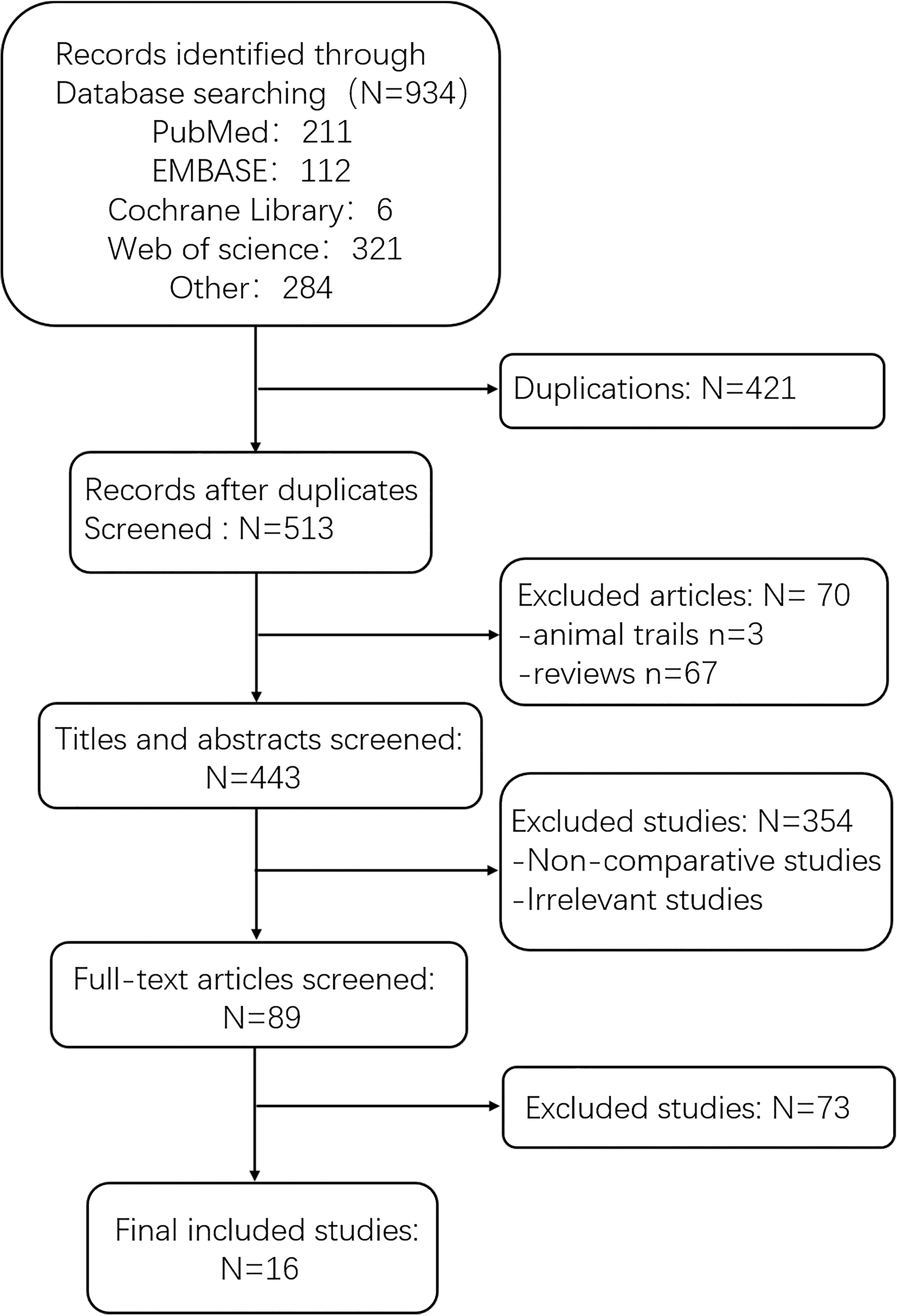
Flowchart diagram of the literature search.
Basic Characteristics of Included Studies
Comparability variables: 1 = age, 2 = gender, 3 = body mass index, 4 = tumor size, 5 = tumor side, 6 = tumor position, 7 = clinical stage, 8 = American Society of Anesthesiologist scores, 9 = abdominal surgery history.
NA = data not available; NSD = no significant difference between the two groups; RP = retroperitoneal; TP = transperitoneal.
All included studies were published between 2013 and 2020. Included studies were conducted in the United Kingdom, United States, South Korea, China, and Japan. Eight studies 13,14,16,19,20,22,24,25 had no significant differences between the two groups in basic characteristics of the patients, which scored ≥7 and were considered to be of high quality (Table 1).
Outcomes of the meta-analysis
Meta-analysis of intraoperative outcomes
Pooled data from 10 studies 13,16 –20,22,24,26,27 that reported the mean OT were suitable for this meta-analysis. The RE model was used for analysis as there was a prominent degree of heterogeneity (p < 0.00001, I 2 = 85%). The results show that OT was slightly shorter in the RP-RAPN than in the TP-RAPN (RE: WMD 13.18 minutes; 95% CI 5.04–21.31; p = 0.001) (Fig. 2A). In all, 15 studies reported about WIT. Ten 13,14,17 –20,22,24,26,27 of these studies had data that were considered suitable for this meta-analysis. There was a prominent statistical heterogeneity (p = 0.002, I 2 = 66%) by the RE model. There was no statistical difference in the WIT between the two cohorts for RAPN (RE: WMD 0.13 minutes; 95% CI −0.39 to 0.65; p = 0.64) (Fig. 2B). Data from seven studies 13,17,19,22,24,26,27 that reported the mean EBL were considered suitable for this meta-analysis. The RE model was used for analysis as there was a moderate degree of heterogeneity (p = 0.02, I 2 = 62%). The results support the RP-RAPN cohort, which had a lower EBL than the TP-RAPN cohort (RE: WMD 7.08; 95% CI 1.41–12.74; p = 0.01) (Fig. 2C). Three studies 14,21,24 that had data on conversion to radical nephrectomy rates were suitable for this meta-analysis. The FE model was used for analysis as there was a low degree of heterogeneity (p = 0.90, I 2 = 0%). There were no statistically significant differences between the two groups (FE: OR 1.57; 95% CI 0.75–3.27; p = 0.23). Only two studies 12,24 that had data on conversion to open operation rates were suitable for this meta-analysis. The FE model was used for analysis as there was a low degree of heterogeneity (p = 0.50, I 2 = 0%). There were no statistically significant differences between the TP-RAPN and RP-RAPN cohorts (FE: OR 0.81; 95% CI 0.16–4.16; p = 0.80).
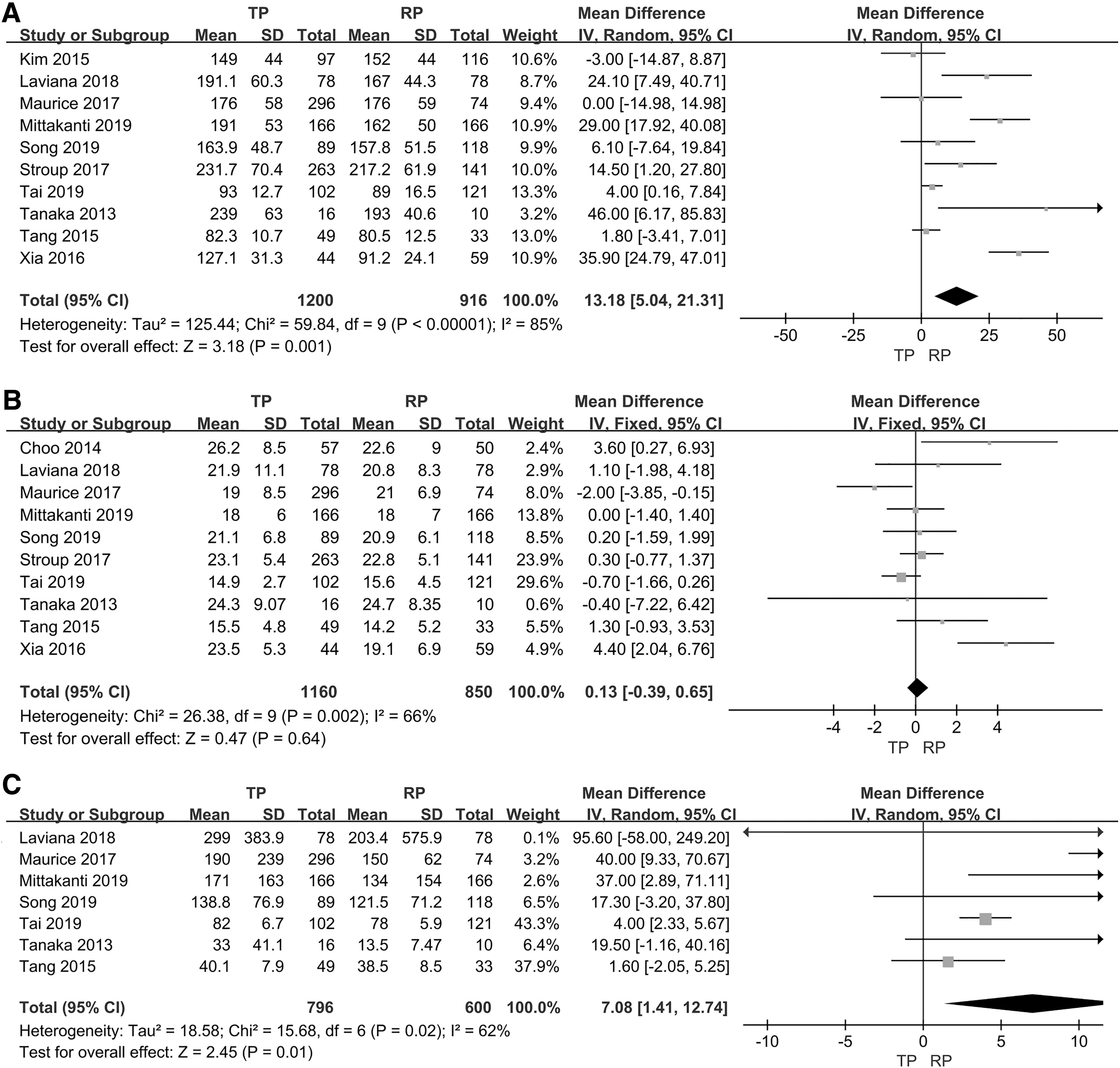
A meta-analysis of intraoperative variables of TP-RAPN vs RP-RAPN (forest plots).
Meta-analysis of postoperative and oncologic outcomes
Pooled available data from five studies 19,20,22,24,26 that reported the mean LOS were included for this meta-analysis. The RE model was used for analysis as there was a prominent degree of heterogeneity (p < 0.05, I 2 = 83%). The meta-analysis results showed that LOS was shorter in the RP-RAPN group than in the TP-RAPN group (RE: WMD 0.51; 95% CI 0.25–0.77; p = 0.0001) (Fig. 3A). Only two studies 26,27 reported the drainage tube removal time. The FE model was used for analysis as there was a prominent degree of heterogeneity (p = 0.02, I 2 = 81%). There were no significant differences between RP-RAPN and TP-RAPN in drainage tube removal time (RE: WMD 0.45; 95% CI −0.04 to 0.94; p = 0.07). Four studies 17,18,26,27 reported available data on postoperative bowel function recovery time. The RE model was used for analysis as there was a prominent degree of heterogeneity (p < 0.00001, I 2 = 99%). The meta-analysis results showed that the postoperative recovery time of the bowel function was shorter in the RP-RAPN group than in the TP-RAPN group (RE: WMD 1.97; 95% CI 0.43–3.52; p = 0.01).
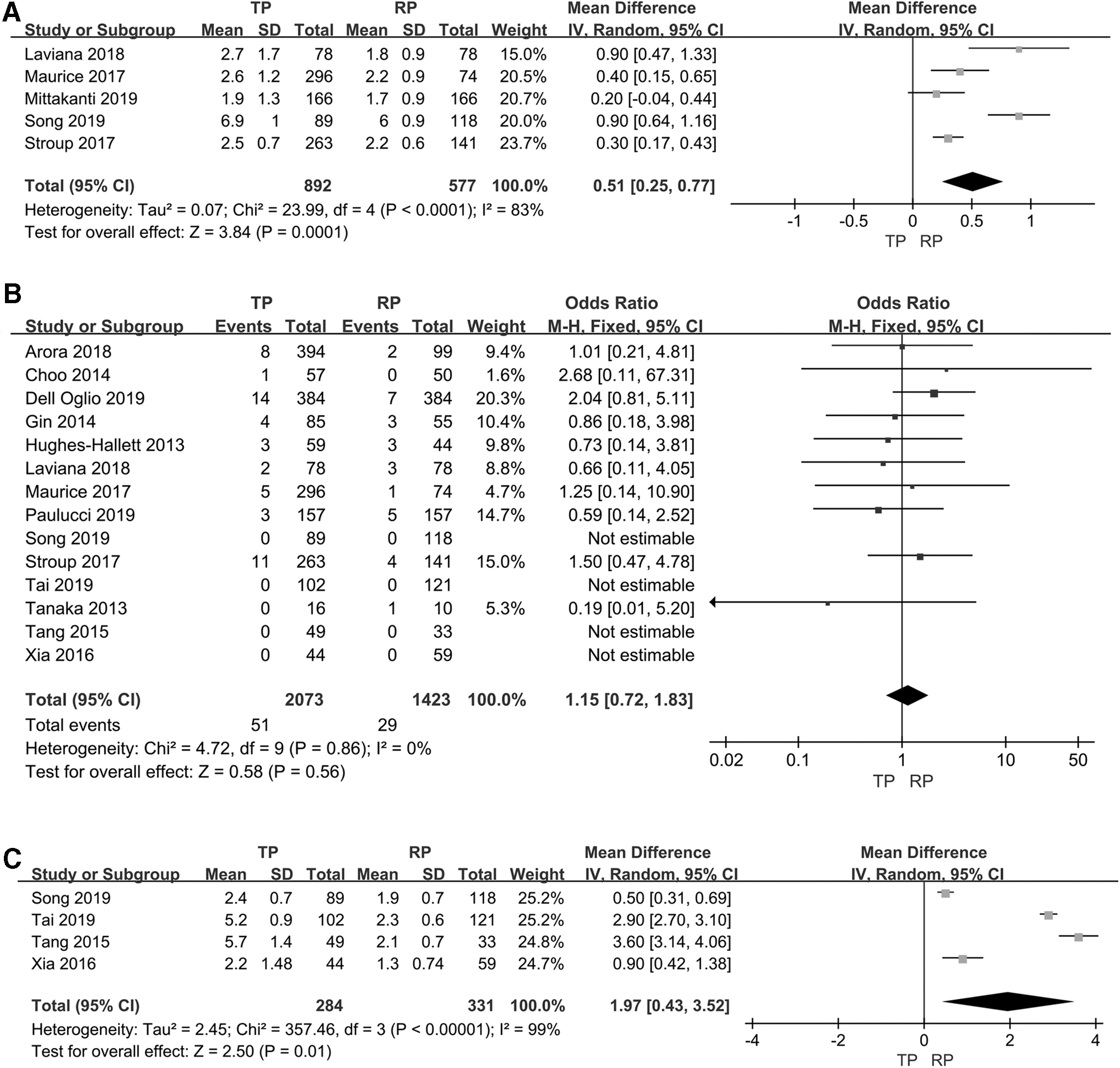
A meta-analysis of postoperative and oncologic outcomes of TP-RAPN vs RP-RAPN (forest plots).
Pooled available data from 14 studies 12 –15,17–23,25 –27 that reported PSM were considered suitable for this meta-analysis. The FE model was used for analysis as there was a low degree of heterogeneity (p = 0.86, I 2 = 0%). These studies did not show a significant difference between RP-RAPN and TP-RAPN (FE: OR 1.15; 95% CI 0.72–1.83; p = 0.56) (Fig. 3B). Only two studies 12,19 reported recurrence rate, and these outcomes were not suitable for this meta-analysis. These studies did not show a significant difference between TP-RAPN and RP-RAPN. None of the studies reported the survival rates, making it impossible to perform meta-analysis.
Meta-analysis of complications
Pooled available data from eight studies 12 –14,16,19,20,22,25 that reported the overall complication rate were included for this meta-analysis. The FE model was used for analysis as there was a low degree of heterogeneity (p = 0.88, I 2 = 0%). These studies had no statistical differences between RP-RAPN and TP-RAPN (FE: OR 1.23; 95% CI 0.91–1.66; p = 0.18) (Fig. 4A). Twelve studies 13,15 –22,24,25,27 that reported available data on major complication rates were suitable for this meta-analysis. The FE model was reported for analysis as there was a low degree of heterogeneity (p = 0.83, I 2 = 0%). There were no statistically significant differences between two RAPN groups (FE: OR 0.77; 95% CI 0.51–1.16; p = 0.21) (Fig. 4B). Only two studies 19,21 reported the intraoperative complication rate. The FE model was reported for analysis as there was a low degree of heterogeneity (p = 0.36, I 2 = 0%). There were no significant differences between RP-RAPN and TP-RAPN in the intraoperative complication rate (RE: OR 1.13; 95% CI 0.40–3.24; p = 0.81).
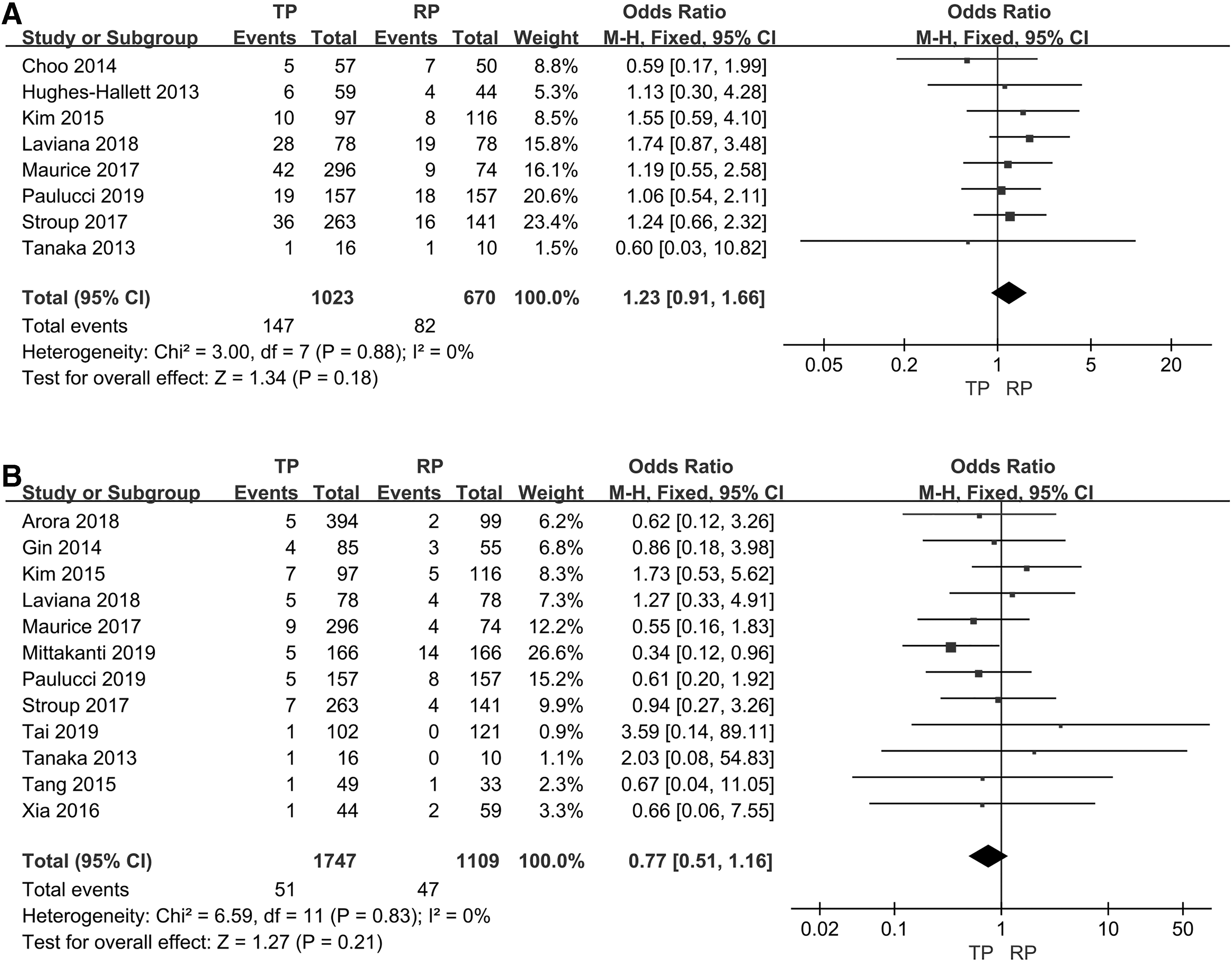
A meta-analysis of complicates of TP-RAPN vs RP-RAPN (forest plots).
Sensitivity analysis and publication bias
We removed each single study respectively to evaluate its effect on the mixed outcome indicator, and the sensitivity analysis indicated a relatively stable mixed result. By the sensitivity analysis and the subgroup analysis of high-quality retrospective control studies, the pattern of differences was similar to the initial analysis of meta-analysis (Table 2). The sensitivity analysis for OT was significantly lower in the RP-RAPN group than in the TP-RAPN group. In the sensitivity analysis of the mean EBL (WMD 5.67; 95% CI 0.57–10.77: p = 0.03), the number of patients in the sensitivity analysis was close to the whole analysis. Meanwhile, the sensitivity analysis result was close to the critical value. Further subgroup analysis was performed (Fig. 5); the results showed that statistical heterogeneity significantly reduced (p = 0.77, I 2 = 0%) and that EBL was significantly lower in the RP-RAPN and TP-RAPN groups in the United States (WMD 39.89; 95% CI 17.33–62.45: p = 0.0005). Similar to the United States, there was a low degree of heterogeneity (p = 0.21, I 2 = 35%) and had statistical differences between the two groups in China (WMD 3.42; 95% CI 0.72–6.12; p = 0.01). After a comprehensive evaluation, the results of EBL used by the subgroup analysis were discussed. For the LOS, the statistical heterogeneity significantly reduced when we removed the two studies 22,26 (p = 0.52, I 2 = 0%). It is suggested that these two studies had the high possibility of the origin of heterogeneity between studies. Due to the limited number of included studies, meta-regression analysis was not performed.
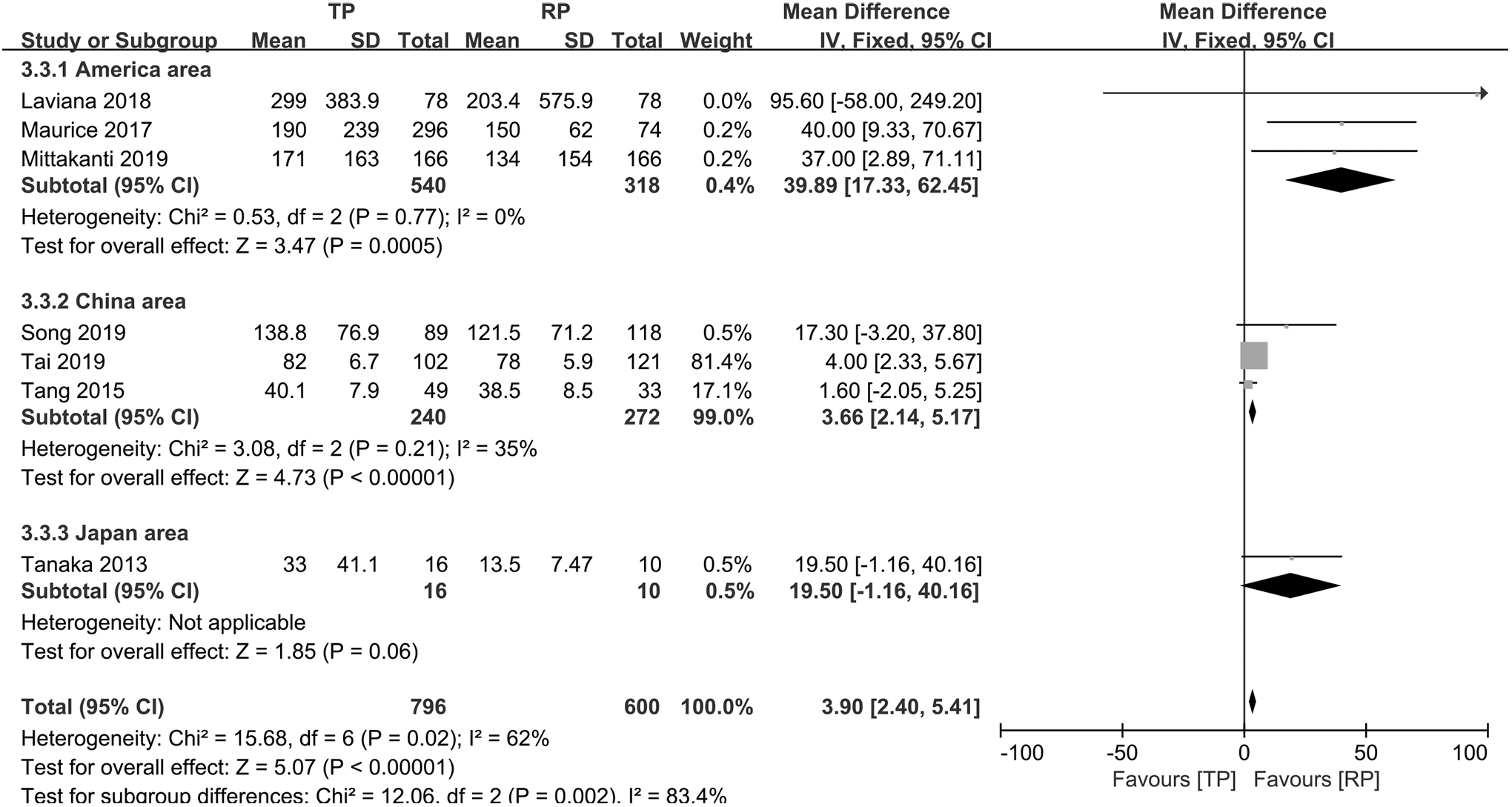
Subgroup analysis of EBL of TP-RAPN vs RP-RAPN (forest plots).
Sensitivity Analysis: TP-RAPN vs RP-RAPN
p < 0.05; ** p < 0.01; *** p < 0.001.
CI = confidence interval; MD = mean difference; OR, odds ratio; RP-RAPN = retroperitoneal approach in robot-assisted partial nephrectomy; TP-RAPN = transperitoneal approach in robot-assisted partial nephrectomy.
The funnel plot was used to test the existence of publication bias. The funnel plot for WIT is shown in Figure 6A. Three studies reported asymmetrical 95% CIs, indicating potential publication bias. The funnel plot for major complication rate suggested that all the studies were within the 95% CI and distributed basically symmetrical in the vertical direction, indicating that there was no significant publication bias in the included studies (Fig. 6B).

Funnel plots of outcomes.
Discussion
This meta-analysis included 16 studies. 12 –27 We pooled the presently available studies, with the comparisons of the clinical effects for the RP-RAPN group with the TP-RAPN group. The results showed that RP-RAPN had shorter OT, LOS, postoperative bowel function recovery, and lower EBL than TP-RAPN. There were no statistically significant differences between the two cohorts in other outcomes.
According to our initial meta-analysis, RP-RAPN had a shorter OT than TP-RAPN. As we all know, urologists selected the most appropriate surgical approach according to the size, location, and complexity of the tumor for patients. There are a large operative space and anatomical marks of the transperitoneal (TP) approach, which is easier to identify and operate. The integrity of the peritoneum in intraoperative is not needed to be protected. Therefore, for larger more complex tumors and tumors near the hilum, the TP approach is preferred. Thus, a difference of 13.18 minutes is to be expected based on clinical experience, although the retroperitoneal (RP) approach had a small working space and limited physiological landmarks. 28 However, the robot-assisted laparoscopic surgery system had an extremely flexible manipulative robotic arm especially applicable to RP-RAPN, it reduced the disadvantage of small space to some extent. 29 On the one hand, the RP approach can directly enter the surgical field without more free mesangium and peritoneal mesangium, less tissue separation, and intraperitoneal interference. On the other hand, they do not need to deal with bowel and abdominal organs; RP-RAPN provides direct and rapid access to the renal hilum. 28 There was no difference in WIT in this meta-analysis. In terms of the average EBL, we found that the RP-RAPN group had lower EBL than the TP-RAPN group. The reduction in EBL of the RP group was thought to be related to the surgical dissection and OT. For larger more complex tumors, and tumors near the hilum, the TP approach is frequently used. Thus, the RP-RAPN group had lower EBL than the TP-RAPN group, which is to be expected. The WMD of 7.08 mL is of no significance. Nevertheless, its clinical significance is not obvious. The advantage of the RP-RAPN is that after entering the retroperitoneum, more blunt separation along the nonvessel plane and provides direct and rapid access to the renal hilum. The separation range is relatively small, especially for the exposure and treatment of renal pedicle vessels is relatively easy. 27 Meanwhile, the results of the subgroup analysis showed that the difference in EBL in developed countries is more obvious than that in China. This may be related to the familiarity of the different surgical accesses. Urologists in China are more proficient at RP approach. Indeed, in European and American countries, the surgical approach for TP-RAPN remains a surgeon's preference. The transabdominal approach is utilized by most urologists due to the larger operating space and obvious anatomy, which makes it easier to deal with the renal hilum and ventral tumor directly, and it has better advantages in the treatment of large tumors and blood vessels. Futhermore, the RP-RAPN is necessary to guarantee integrity of peritoneum during the surgery. 7,21,30 Of note, in recent years, Tai et al. 27 lead new surgical approaches in recent years, with combined TP and RP access for RAPN. In the operation of this approach, there is a large operating space and it is easy to expose renal pedicled vessels. Meanwhile, the integrity of the abdominal membrane is not needed to be retained. At present, this type of approach has less international implementation, and more comparative studies are needed to confirm conclusions.
Bowel mobilization potentially increases the risk of ileus, but there was no difference in complication rate for meta-analysis. Choo et al. 14 using matched-pair analysis showed no bowel-related complications that occurred for the patient by two surgical accesses. Laviana et al. 22 found that complications had no significant difference between two surgical approaches, although there was a trend toward fewer overall complications with RP RAPN. The reason may be due to that RP-RAPN does not require mobilization of the colon and the bleeding or urine leakage is isolated to the retroperitoneum. The eight studies 12 –14,16,19,20,22,25 in meta-analysis each had no significant difference in complications. Unfortunately, only one study 19 reported the overall complication rate with specific events, which may have introduced bias. These results cannot support that RP-RAPN is safer than TP-RAPN because the allocation to the treatment groups was decided by the physician and TP-RAPN is used more frequently in complicated cases. But our analysis showed that RP-RAPN is at least as safe as TP-RAPN. However, it is necessary to take into consideration that abdominal surgery influenced the postoperative recovery times of bowel function to some extent. There were statistically significant differences in postoperative recovery time of bowel function in this meta-analysis. The LOS was also significantly shorter in RP-RAPN than in TP-RAPN. Kim et al.'s 16 study via a single-institution retrospective comparison found that the RP-RAPN patients needed significantly fewer antiemetics drugs, showing that an earlier return of satisfactory oral intake and bowel function was able to reduce the LOS. Less LOS will reduce the financial burden of patients to some extent. The LOS has been shown as the most significant variable determining the overall cost of PN in Uzzo et al.'s study. 31 In addition, Laviana et al. 22 by using the time-driven activity-based costing (TDABC) model for renal masses found that the disposable instrument costs for the RP-RAPN group are slightly more than the costs for the TP-RAPN, but overall costs were $2337.16 less for the RP-RAPN group.
In our analysis, there were no statistically significant differences between RP-RAPN and TP-RAPN in intraoperative conversion to radical nephrectomy rate, complication rate, and PSM. Some studies 7,12,19,22 reported that the postoperative eGFR had no difference between the two groups. But in the latest study of Dell'Oglio et al., 23 which used a large global collaborative data set, propensity score matching and logistic and linear regression analyses found a statistically significant difference in postoperative eGFR. However, 1 year after surgery, no difference was recorded in the two groups. Therefore, the meta-analysis was not suitable for postoperative renal function owing to the paucity of studies reporting this specific outcome. And, the length of follow-up varied among studies, which might be a source of bias. Moreover, two studies 7,20 reported a similar Pentafecta rates for the RP-RAPN and TP-RAPN groups. And, two studies 12,19 reported that there were no significant differences in recurrence rate and survival rate between TLRN and RLRN; these outcomes were not applicable to meta-analysis. Therefore, long-term follow-up in future studies is needed to evaluate the complication rates and oncologic outcomes for two surgical approaches.
In these studies, we found that most urologists prefer the TP-RAPN to be used to the anterior and hilar tumors, and the RP-RAPN is used more for posterior and laterally tumors. This is one of the sources of bias. Several studies 16,19,22 have shown that two surgical approaches offered similar oncologic outcomes and safety profiles for posterior and laterally tumors of renal. Recently, Dell'Oglio et al.'s study 23 prominently reduced the influence factor of tumor location by design. It demonstrated that the RP-RAPN group is essentially no different with the TP-RAPN group regarding safety and effectiveness. And, the RP-RAPN group had a lower EBL than the TP-RAPN group. There were no differences in perioperative morbidity and functional and oncologic outcomes.
To the best of our knowledge, this meta-analysis provides the most up-to-date information in this field and is the latest and comprehensive meta-analysis comparing RP-RAPN and TP-RAPN. This study by rigorous meta-analytical methods performed multiple strategies to confirm the study results and evaluated the quality of the studies. We used the sensitivity analysis and the subgroup analysis to minimize the effects of heterogeneity. Compared to previous systematic reviews on this topic, the present study included the more recently published study that can provide evidence-based medical evidence for the surgical approach in RAPN.
Certainly, we must recognize some limitations in this meta-analysis. And, it should be considered when interpreting the results. First, all the studies were retrospective, and it was difficult to completely match all the basic characteristics of patients. The lack of random design and blinding also influenced the reliability of experimental data. Second, some studies did not report data and the number or proportion of patients who lost to follow-up, which also affected the credibility of the conclusion to some extent. Third, the degree of familiarity of the surgeons with the two surgical approaches in each study may affect the accuracy of the outcome indicators. Therefore, more high-quality, large samples, long-term follow-up, randomized controlled and case–control studies are still needed to further compare the clinical effects of the two surgical approaches in RAPN.
Conclusions
Both approaches have their advantages and limitations. Urologists are required to specialize in different approaches, considering which approach to be used based on tumor size, location, and maximum benefit for the patient. Compared with the TP-RAPN, the RP-RAPN had significantly shorter OT, postoperative bowel function recovery time, LOS, and lower EBL. No significant differences were found in other outcomes. And, RP-RAPN is associated with better value for posterior and laterally located tumors and is faster and equally safe for the patient.
Footnotes
Acknowledgment
We are grateful to Yaojun Xiao, PhD, for giving some advices.
Author Disclosure Statement
The authors declare that there are no conflict of interests. ORCID: S.G.:
Funding Information
This study was funded by the National Natural Science Foundation of China Youth Program (81500576).
Supplementary Material
Supplementary Data
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.