
Abstract
Objectives:
Although there is no comparison study about the learning curves for holmium laser enucleation and other surgical modalities to treat benign prostatic hyperplasia (BPH), beginner urologists are hesitant to perform holmium laser enucleation because of its steep learning curve. Therefore, we investigated the degree of surgical difficulty of holmium laser enucleation by comparing its learning curve with that of transurethral resection.
Patients and Methods:
Two beginner urologists performed surgery for BPH: H.J.Y. performed holmium laser enucleation and K.H.K. performed transurethral resection. Of 141 patients, 72 were enrolled in the holmium laser enucleation group and 69 in the transurethral prostate resection group. After retrospectively reviewing medical records, we performed a cumulative sum analysis of resection speed (RS) and resected ratio (RR) to compare the learning curves of holmium laser enucleation and transurethral resection.
Results:
Both surgeons achieved RS competency with a speed <0.13 g/min. The surgeon who performed holmium laser enucleation achieved RR competency with a ratio <0.40, whereas the surgeon who performed transurethral resection achieved competency with a ratio <0.35. To achieve RS competency of 0.13 g/mL, the holmium laser enucleation and transurethral resection groups required 12 and 23 cases, respectively. To achieve RR competency of 0.35, the holmium laser enucleation and transurethral resection groups required 12 and 5 cases, respectively.
Conclusions:
Holmium laser enucleation is not a difficult procedure compared with transurethral resection in beginner urologists. Therefore, it is unnecessary to avoid holmium laser enucleation because the concerns that it may be difficult are unfounded.
Introduction
Even though holmium laser enucleation of the prostate (HoLEP) could replace transurethral resection of the prostate (TURP) as the current gold standard treatment for benign prostatic hyperplasia (BPH), 1 several urologists are hesitant to perform HoLEP because of its steep learning curve. 2 –7 Furthermore, HoLEP has not been readily selected as a surgical modality by beginner urologists for BPH because most previous reports of the learning curve associated with HoLEP have included only expert surgeons. To the best of our knowledge, there is no comparative study of the learning curves for TURP and HoLEP. Therefore, for beginner urologists, the concern that HoLEP may be a difficult procedure seems baseless. Because there has been no comparative study regarding the learning curves for TURP and HoLEP, the degree of surgical difficulty of HoLEP should be investigated by comparing the learning curves of HoLEP and TURP. Therefore, the authors attempted to determine the degree of surgical difficulty of HoLEP by comparing the learning curves and intraoperative results of HoLEP and TURP.
Materials and Methods
Procedure
Two beginner urologists performed surgical treatment of BPH after completing 2 years of fellowship training. H.J.Y. performed only HoLEP for BPH, and K.H.K. performed only TURP for BPH. H.J.Y. and K.H.K. were trained to perform HoLEP and TURP by two different experts. They had performed surgery under the partial supervision of their mentors during fellowship training, but they had not performed these procedures without supervision.
A 72-W OmniPulse (Trimedyne, Inc., Irvine, CA) was used for HoLEP, and the energy source consisted of a 72-W holmium:yttrium aluminum garnet laser with a 550-μm laser fiber. Enucleated prostatic tissue was removed by transurethral morcellation using a mechanical morcellator (Richard Wolf, Knittlingen, Germany) that was introduced through an offset rigid nephroscope. For TURP, a standard Richard Wolf rectoscope and working elements were used, and a bipolar technique was applied for all TURP cases.
Patients
One hundred forty-one consecutive patients underwent HoLEP or TURP to treat BPH. Of these 141 patients, 72 were enrolled in the HoLEP group and 69 were enrolled in the TURP group. HoLEP was performed by H.J.Y. between June 2014 and January 2018, and TURP was performed by K.H.K. between April 2016 and March 2018. After receiving institutional review board approval, we conducted a retrospective chart review of the included patients.
Clinical data and end points
Age at the time of surgery, International Prostate Symptom Score (IPSS), quality of life (QoL) score, the maximum urinary flow rate (Qmax), postvoid residual urine volume (PVR), total prostate volume, transition zone volume, intraoperative prostate-specific antigen (PSA), and body mass index were estimated as the preoperative variables for analysis. Resection speed (RS) and resected ratio (RR) were used as perioperative variables. RS was defined as the total amount of removed tissue after TURP or HoLEP in grams divided by the total operative time in minutes, 8 and RR was defined as the volume of resected tissue divided by the preoperative transition zone volume. The IPSS, QoL score, and Qmax, which were evaluated at 3 months after surgical treatment, were estimated to determine postoperative outcomes. Serum PSA for all included patients was assayed with a Cobas-e411 system (Roche Diagnostics), and the prostate volume and transition zone volume were estimated from transrectal ultrasound results using the prolate ellipsoid formula. 9,10 The end points of this study were RS and RR of TURP and HoLEP performed by two different beginner urologists.
Statistical analysis
Baseline characteristics of the HoLEP group and TURP group were compared using an analysis of variance (ANOVA) for continuous variables and a chi-square test for categorical variables. These were performed using SPSS Statistics version 20.0.0 (IBM Corp., Armonk, NY). Two-sided p < 0.05 was considered statistically significant. The cumulative summation (CUSUM) analysis 11 was used to determine the learning curve for each beginner urologist enrolled in this study.
CUSUM analysis
To perform the CUSUM analysis, four parameters must be defined: acceptable failure rate (p0), unacceptable failure rate (p1), type I error rate (α), and type II error rate (β). We considered an acceptable failure rate of 20% and an unacceptable failure rate of 40%. The probabilities of type I and type II (α and β) errors were set at 0.05 and 0.20, respectively. Using these parameters, two decision limits (h0 and h1) and the variables were calculated using the formulas shown in Table 1. 12
Cumulative Sum Equations and the Variables Used to Perform Cumulative Summation Analysis
Results
The baseline characteristics of the HoLEP group and TURP group are presented in Table 2. Regarding the preoperative variables, the HoLEP group was significantly younger than the TURP group (median 75.0 vs 77.0 years), and the HoLEP group had significantly larger prostate volumes (median 65.0 vs 57.0 mL) and transition zone volumes (median 41.0 vs 27.0 mL) than the TURP group. Regarding the perioperative variables, the RS of the TURP group was significantly superior to the RS of the HoLEP group (median 0.26 vs 0.22 g/min). Regarding the postoperative variables that were identified at 3 months after surgery, there was no significant difference in the urodynamic results of the two groups.
Preoperative, Perioperative, and Postoperative Outcomes at 3 Months
HoLEP = Holmium laser enucleation of the prostate; IPSS = International Prostate Symptom Score; PSA = prostate-specific antigen; PVR = postvoid residual urine volume; QoL = quality of life; RR = resected ratio; RS = resection speed; TURP, transurethral resection of prostate.
Postoperative complications within 3 months after surgery are presented in Table 3. In each group, complications with Clavien–Dindo classification grade III or more were identified in two cases; these complications were postoperative bleeding, and electric cauterization was performed under general anesthesia. At 3 months after surgery, 7 patients in the HoLEP group and 6 patients in the TURP group were treated with anticholinergics because of urgency.
Postoperative Complications Within 3 Months After Operation
UTI = urinary tract infection.
The overall learning curves are presented in Figure 1. Regarding RS, both surgeons achieved competency, with speeds <0.13 g/min. Regarding RR, the surgeon who performed HoLEP achieved competency with a rate <0.40, and the surgeon who performed TURP achieved competency with a rate <0.35. To achieve RS competency of 0.13 g/mL, the HoLEP group and TURP group required 12 and 23 cases, respectively. To achieve RR competency of 0.35, the HoLEP group and TURP group required 12 and 5 cases, respectively.
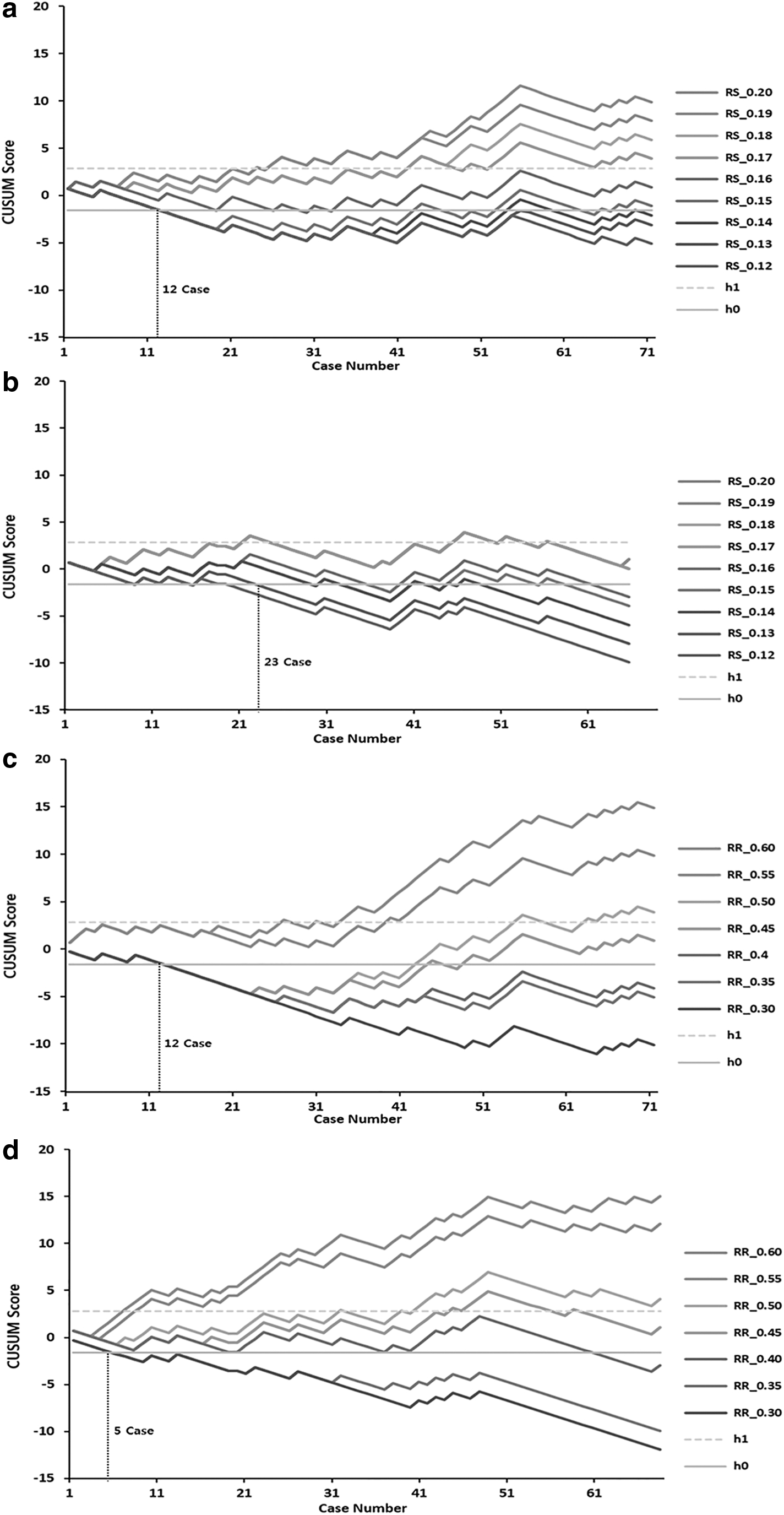
The overall learning curve.
Discussion
The CUSUM technique was originally developed to monitor the performance in the industrial field, and it has been adopted in the medical field to investigate the learning curves of surgical techniques. Several studies have reported using the CUSUM analysis in the urologic field. 13 –19
There have been several comparison studies between TURP and HoLEP 20 –27 that demonstrated that HoLEP was not inferior to TURP regarding postoperative urodynamic results, and that it was superior to TURP regarding catheterization duration and hospital stays. Therefore, it has been suggested that HoLEP could replace TURP as the gold standard treatment for BPH. 1
HoLEP is known to have a steep learning curve. 2 –7 El-Hakim and Elhilali compared the outcomes of HoLEP performed by an unexperienced urologist and by an expert urologist and suggested that extensive experience with transurethral surgery is essential for effective HoLEP. 7 Shah and colleagues performed a prospective study based on the experiences of surgeons who performed transurethral surgery for 150 cases; they suggested that urologists inexperienced with HoLEP could perform HoLEP with reasonable efficiency after performing 50 procedures. 6 Bae and colleagues reported that stable enucleation and morcellation efficiency could be achieved after performing 30 procedures and 20 procedures, respectively. 5 Brunckhorst and his colleagues reported a learning curve of 40 to 60 procedures for HoLEP in their retrospective study that was based on the experiences of a surgeon who performed transurethral surgery for 500 cases. 4 A recent report by Robert and colleagues demonstrated that 20 procedures are probably sufficient to motivate surgeons to continue choosing HoLEP as treatment. 2
If HoLEP has a steep learning curve that creates difficulty for urologists, then its difficulty level could be a major limitation that would prevent it from becoming the new gold standard treatment for BPH. Furthermore, HoLEP has not been readily selected as a surgical modality for BPH, especially by beginner urologists; most previous reports of the learning curve associated with HoLEP have included only expert surgeons. These factors have limited the widespread use of HoLEP. Therefore, a comparison study of the learning curves of HoLEP and TURP must be performed before HoLEP can replace TURP as the gold standard for BPH treatment. However, to the best of our knowledge, no comparison study of the learning curves of TURP and HoLEP has been performed.
This study indicated that it is easier to achieve an RS of 0.13 g/mL with HoLEP than with TURP, and that it is easier to achieve a more efficient RR (0.40 vs 0.35) with HoLEP than with TURP. After performing this comparison study of the learning curves of HoLEP and TURP with the CUSUM analysis, we suggest that HOLEP is not more difficult than TURP when performed by beginner urologists and that it is not necessary to avoid HoLEP because of its reputation as a difficult procedure.
This study had some limitations. It was retrospective. Because incontinence-related studies, such as pressure-flow study, had not been conducted after surgery, this study had the limitation that it could not present postoperative urinary incontinence accurately. The number of included patients was relatively small. However, we judged that the scale of this study, which involved ∼70 patients who underwent HoLEP or TURP, was adequate for evaluating the initial surgical experience because a learning curve of 20 to 60 procedures was shown to be necessary to sufficiently learn the HoLEP procedure. However, the results reported here need to be confirmed and validated by analyzing data from a prospective study.
Conclusion
HoLEP is not a difficult procedure for beginner urologists to perform. Therefore, it is unnecessary to avoid performing HoLEP because of its perceived difficulty.
Footnotes
Acknowledgment
This article was prepared with the assistance of EDITAGE, an English-language scientific editing company.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This study was supported by the “Soonchunhyang University Research Fund.”