
Abstract
Introduction and Objective:
Robotic radical nephroureterectomy (RRNU) may offer advantages over laparoscopic radical nephroureterectomy (LRNU). The purpose of this study is to evaluate the overall survival (OS) of patients with upper tract urothelial carcinoma (UTUC) who underwent RRNU vs LRNU and identify factors that account for differences.
Methods:
The National Cancer Database was queried from 2010 to 2016 for patients with American Joint Committee on Cancer 6th/7th edition Stage I/II/III UTUC. Kaplan–Meier analysis compared LRNU and RRNU OS. Univariate analysis detected differences between the groups. Cox regression determined factors associated with mortality rate. Logistic regression identified predictors of a lymph node dissection (LND) and 90-day mortality rate.
Results:
A total of 2631 patients met the criteria, 1129 of whom underwent RRNU and 1502 LRNU, with a follow-up of 33 and 35 months, respectively (p = 0.063). RRNU had a median OS of 71.1 vs 62.6 months (p = 0.033). LRNU patients were older (72.7 vs 71.4, p < 0.001) and had no differences in comorbidities, pathologic T stage, or grade. The LRNU cohort was less likely to undergo LND (19% vs 35%, p < 0.001) and had a lower median lymph node yield (3 vs 4, p < 0.001). LRNU patients more likely underwent conversion to an open procedure, had longer hospital stays, and higher 30- and 90-day mortality rates. LRNU was independently associated with mortality rate (p = 0.030). Age, grade, positive margins, pT/pN stage were associated with mortality rate. Younger age, RRNU, surgery at an academic center, and neoadjuvant chemotherapy predicted an LND.
Conclusions:
RRNU demonstrated increased rates of LND and may offer a short-term morbidity benefit to LRNU. Survival differences may be due to improved characterization of disease through LND.
Introduction and Objective
Upper tract urothelial carcinoma (UTUC) comprises around 5% of all urothelial cancers and between 5% and 10% of renal tumors. 1,2 The standard of care for treatment of high-grade UTUC is open radical nephroureterectomy (ORNU) with bladder cuff excision. 2 Low-grade UTUC that meets specific criteria can be managed with minimally invasive endoscopy. 2 Over the past 30 years, the oncologic outcomes for patient's undergoing radical nephroureterectomy (RNU) have been stable. 3 However, advances in robotic radical nephroureterectomy (RRNU) and laparoscopic radical nephroureterectomy (LRNU) techniques have changed and continue to change practice patterns in the management of UTUC. 3
The benefits of minimally invasive surgery have been well described and include decreased blood loss, shorter hospital stay, and faster recovery. 4 There are multiple studies comparing ORNU and LRNU, many of which show comparable oncologic outcomes, particularly in patients with lower clinical stage disease. 5 –7 While LRNU has increased in popularity, there are studies suggesting inferior oncologic outcomes especially with more aggressive and bulky tumors. 8,9 The reasons for this finding, however, are unclear and some have hypothesized that management of the bladder cuff and lymphadenectomy accounts for these findings. 10,11
The role of lymphadenectomy at the time of RNU remains an open question. The European Association of Urology guidelines 2 offer limited guidance about when a lymph node dissection (LND) should be performed and the optimal template for this procedure. Furthermore, there is limited evidence on the effect of surgical approach on performance of a lymphadenectomy.
There is a paucity of evidence for evaluating the oncologic outcomes among the LRNU and RRNU approaches in UTUC. The purpose of this study is to compare the oncologic outcomes of these treatment modalities for clinically localized UTUC and identify factors that may account for differences between these groups.
Methods
The National Cancer Database (NCDB) is a clinical oncology database sponsored by the American College of Surgeons and the American Cancer Society that includes >70% of cancer diagnoses in the United States. 1 The NCDB, which is publicly available and IRB exempt, was queried from 2010 to 2016. Inclusion criteria included American Joint Committee on Cancer 6th or 7th edition Stage 0a, 0is, I, II, or III UTUC who underwent RNU with a laparoscopic or robotic approach. Patients with open, endoscopic, or unknown approach to clinically localized UTUC were excluded from analysis. Patients with unknown pT stage, nonlocalized disease, pathologic grade, surgical margin status, and performance of LND data were also excluded. A Kaplan–Meier survival analysis was utilized to compare overall survival (OS) between the LRNU and RRNU groups. Univariate analysis was performed to detect differences between the groups. A Cox regression analysis, including factors identified to contain differences on univariate and known cofounders, was utilized to determine predictors of mortality rate. A multivariate logistic regression was used to identify predictors of 90-day mortality rate as well as predictors of performance of LND. SPSS version 25 (IBM Corporation, Armonk, NY) was utilized for statistical analysis, with the significance set at p < 0.05.
Results
A total of 27,861 patients were included in the NCDB data set. A total of 2631 patients met the inclusion criteria (Fig. 1), 1129 of whom underwent robotic and 1502 who underwent LRNU, with a mean follow-up of 33.3 and 35.1 months, respectively (p = 0.063). The percentage of cases performed robotically increased each year in the study period (Fig. 2), from 29% of minimally invasive RNU in 2010 to 53% in 2016. Patient demographics and clinicopathologic and clinical outcomes are reported in Table 1. Patients who underwent LRNU were older (72.7 vs 71.4, p < 0.001) and were more likely to be female (39.5% vs 34.4%, p = 0.007) There were no differences in Charlson–Deyo scores between the cohorts.
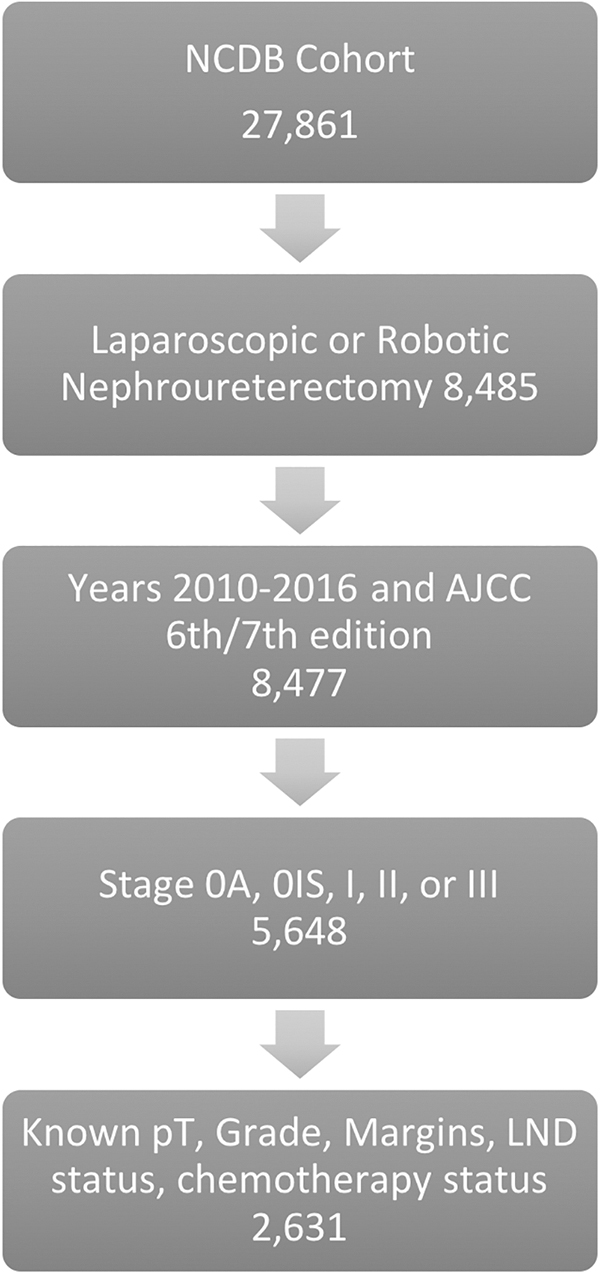
Selection of cohort. AJCC, American Joint Committee on Cancer; LND = lymph node dissection; NCDB = National Cancer Database.
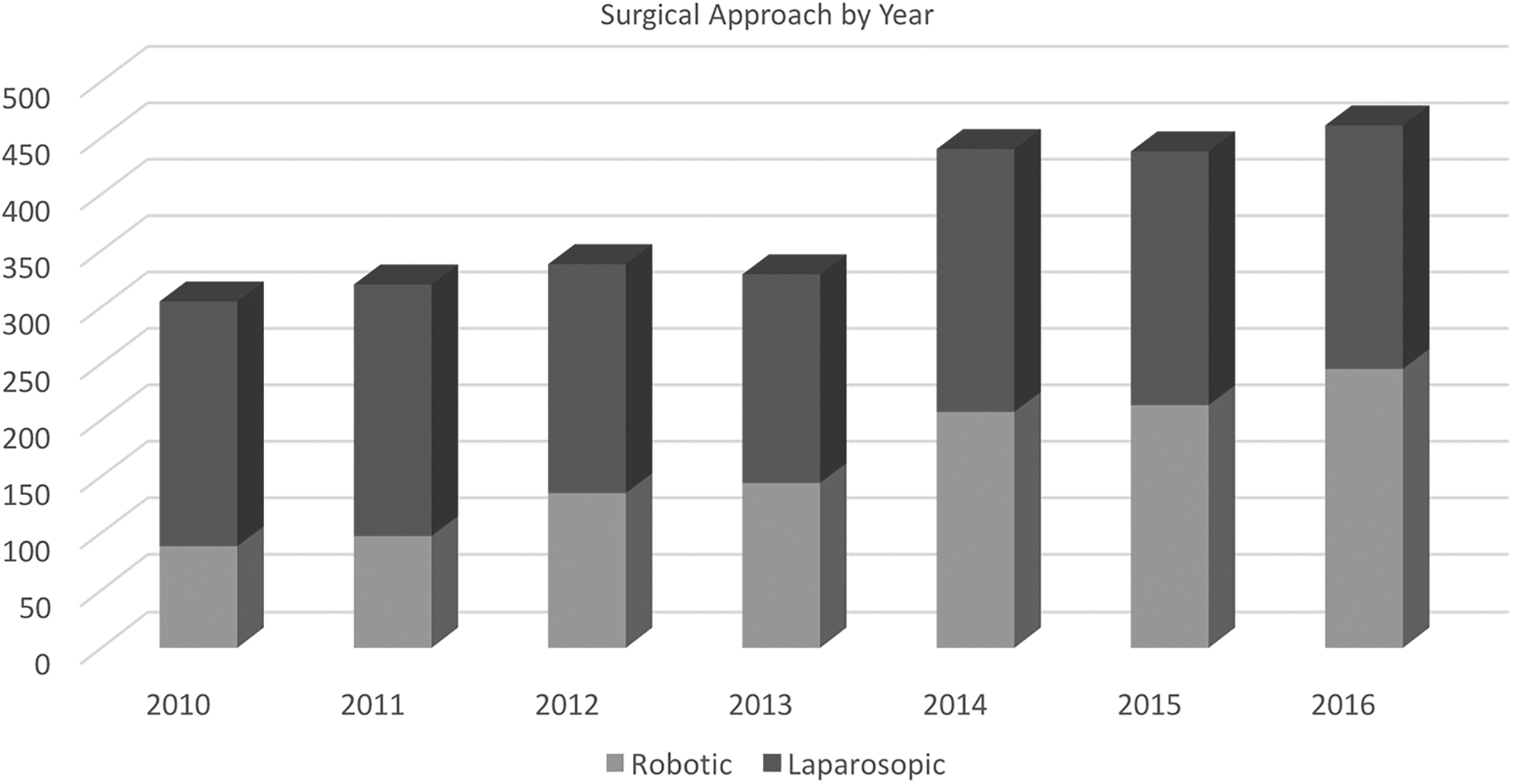
Surgical approach by year.
Comparison of Patient and Clinical Factors
Bold values indicate p < 0.05.
IQR = interquartile range.
There were no differences in the pathologic tumor stage between the groups. The patients who underwent LRNU had a positive margin rate of 12.3% vs 11.1% for the RRNU (p = 0.327). The RRNU cohort was more likely to have undergone LND (35% vs 19%, p < 0.001). While the lymphadenectomy template is not available in the NCDB data set, patients undergoing RRNU had a higher median yield than those in the LRNU group (4 vs 3, p < 0.001) and higher mean node yield (6.4 vs 4.5, p < 0.001).
Patients who underwent the LRNU were more likely to be converted to ORNU (9.9% vs 3.3%, p < 0.001). They also had a longer median hospital stay of 4 (interquartile range [IQR] 2–5) days vs 3 (IQR 3–6) days in the RRNU group (p < 0.001). Patients in the LRNU cohort had significantly increased 30-day (1.7% vs 0.6%, p = 0.028) and 90-day mortality rates (3.1% vs 1.3%, p = 0.009) than those who underwent RRNU.
There was no significant difference in the overall receipt of chemotherapy between the two groups (16.3% in RRNU and 14.9% in LRNU, p = 0.073). Those who underwent RRNU, however, were more likely to undergo neoadjuvant chemotherapy before surgery (4.5% vs 2.6%, p = 0.007). No data were available on chemotherapeutic agents utilized or specific patient comorbidities that could account for administration of chemotherapy.
Kaplan–Meier survival analysis found that patients in the RRNU group had a median OS of 71.1 months vs 62.6 months for those in the LRNU group, p = 0.033 (Fig. 3). On Cox multivariable analysis (Table 2), age, increasing Charlson–Deyo score, poorly differentiated disease, increasing pT stage, positive lymph nodes, and positive surgical margins were independently associated with mortality rate. When compared with RRNU, LRNU was also independently associated with all-cause mortality rate (hazard ratio 1.182, 95% confidence interval [CI] 1.016–1.375, p = 0.030). The year of diagnosis was not found to be independently associated with mortality rate, despite the increase in robotic utilization during the study period.
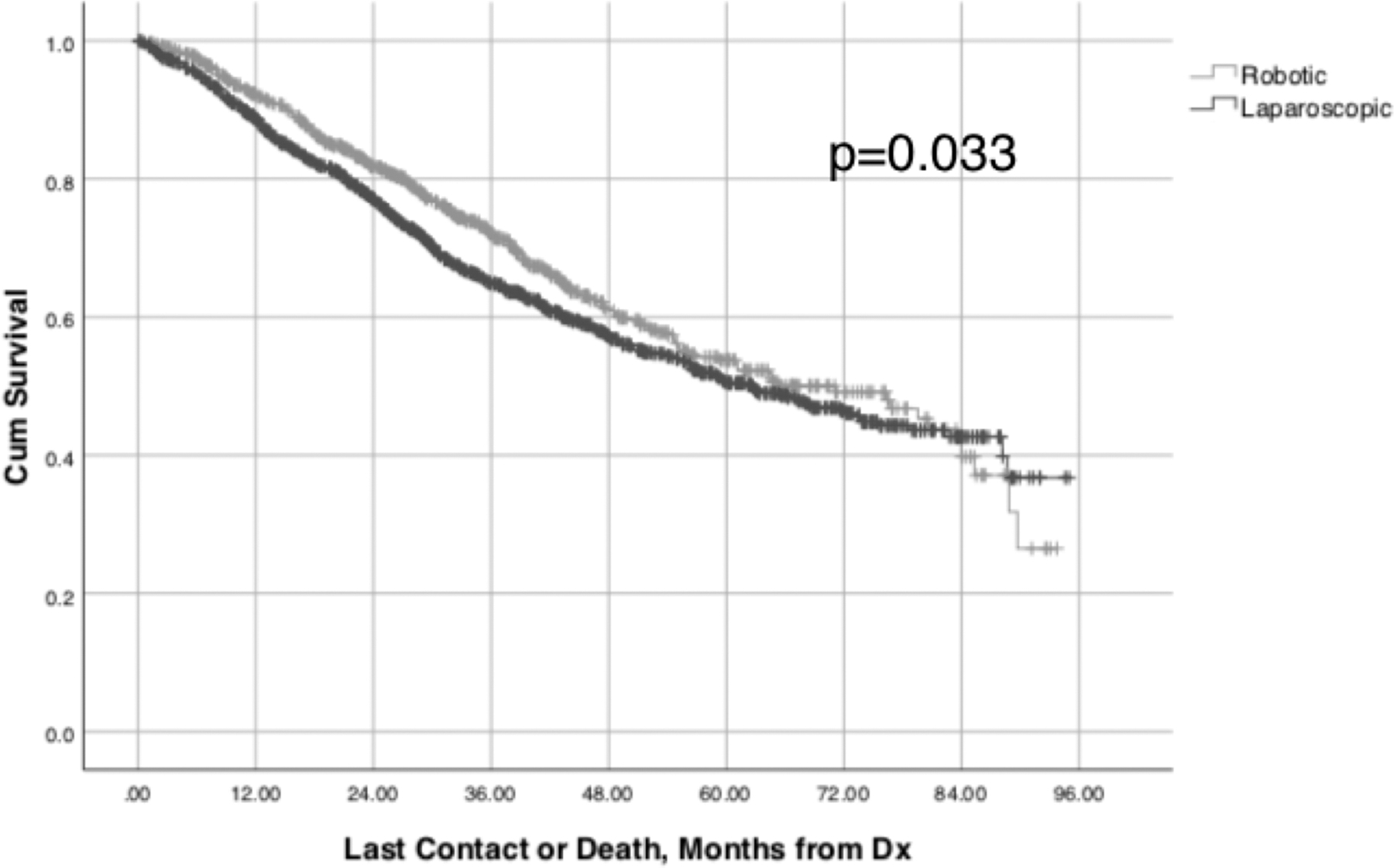
Overall survival by surgical approach.
Predictors of Mortality Rate
Bold values indicate p < 0.05.
CI = confidence interval; HR = hazard ratio; LND = lymph node dissection.
Given the differences in OS between the RRNU and LRNU groups, logistic regression analysis was performed to investigate factors associated with perioperative mortality rate within 3 months of surgery (Supplementary Table S1). Advanced age (odds ratio [OR] 1.072, 95% CI 1.038–1.107) and laparoscopic surgical approach (OR 2.021, 95% CI 1.106–3.695, p = 0.022) were independently associated with higher risk of death at 90 days, while treatment at an academic medical center was independently associated with a lower risk of death (OR 0.394, 95% CI 0.157–0.986, p = 0.047).
Multivariate logistic regression was utilized to examine the association of covariates on performance of LND (Table 3). Younger age (OR 0.980, 95% CI 0.969–0.992, p = 0.001), treatment at an academic medical center (OR 2.080, 95% CI 1.313–3.297, p = 0.002) or at an integrated network cancer center (OR 1.741, 95% CI 1.061–2.856, p = 0.028), poorly differentiated disease (OR 1.915, 95% CI 1.427–2.569, p < 0.001), and receipt of neoadjuvant chemotherapy (OR 2.741, 95% CI 1.746–4.305, p < 0.001) were also strong predictors for lymphadenectomy. Robotic approach was also independently associated with the performance of an LND (OR 2.123, 95% CI 1.760–2.560, p < 0.001).
Predictors of Lymph Node Dissection
Bold values indicate p < 0.05.
OR = odds ratio.
Discussion
This study compares the effect of minimally invasive surgical techniques on oncologic outcomes of nephroureterectomy. RRNU patients are more likely to undergo an LND than those who receive LRNU. They may also have an OS benefit when compared with LRNU, although it is possible that cofounders could account for part of this difference. Patients who undergo RRNU are less likely to undergo conversion to an ORNU, have shorter hospital stays, and lower 30- and 90-day mortality rates.
The role of retroperitoneal LND in an RNU is controversial, given the complicated lymphatic drainage pattern and lack of an agreed-upon template to follow when performing a RNU. 3 Furthermore, there has been conflicting evidence on the oncologic benefit of lymphadenectomy. Roscigno and colleagues reported that patients with pT2–4 disease and unknown nodal status (pNx) had decreased 5-year cancer-specific survival (CSS) when compared with patients with pN0 disease. 12 Other studies have affirmed this finding, reporting increased lymph node yield correlating with improved CSS. 13,14 However, Lughezzani and colleagues evaluated patients without clinically evident nodal lesions and found no difference in oncologic outcomes between those with pN0 and pNx disease. 15 Furthermore, a study of 108 patients performed by Kondo and colleagues found that there was oncologic benefit with a greater extent of LND, but found no association with node yield. 11 Given the lack of consensus in the literature, guidelines remain vague on which patients might benefit from LND and what dissection template is preferred. 2
Although data on the dissection templates utilized among the patients in our study are not available, limiting our ability to definitively characterize the role of LND in clinically localized disease, the increased lymph node yield and higher rate of lymphadenectomy utilization demonstrate that the robotic approach may be favorable over a laparoscopic approach in those for whom a LND is deemed necessary. While the reasons for this finding cannot be elucidated from this data set, it does reinforce the hypothesis that performing a lymphadenectomy is easier robotically. The year of surgery does not appear to affect the choice of lymphadenectomy, adding strength to the argument that lymphadenectomy is related in fact to the surgical technique, rather than a practice change over time.
Another important finding in this analysis is the significantly increased morbidity and potentially decreased survival associated with LRNU. Patients who underwent LRNU are more likely to have an open conversion of their procedure, although some element of this finding could be due to coding error in which an open bladder cuff excision is documented as “conversion to open.” Regardless, it makes sense that open conversion or open bladder cuff excision could prolong the hospital stay, which is observed in our study. In addition, the LRNU technique appears to be significantly associated with the 90-day mortality rate, although it is unclear what is driving this difference, given there is no difference in 30-day readmissions between the groups. Surgery at an academic center was associated with survival at 90 days, and could be due to the fact that these institutions tend to treat more upper tract disease. In terms of 90-day mortality rate, however, patients who underwent LRNU were older and this may have had some confounding effect on the mortality rate numbers. That said, the laparoscopic approach was independently associated with mortality rate on both Cox regression and 90-day mortality rate logistic regression. The OS findings should be received cautiously. The cohorts were not matched in terms of age and there was a trend toward neoadjuvant chemotherapy administration in the robotic group, and these potential confounders alone could explain this difference in the short-term and overall mortality rate.
While these findings have clinical utility, there are some limitations to this study. The study is retrospective and thus subject to possible selection bias. As is the case with all large population-level data sets, we have little information as to why a particular surgical technique was chosen. Given the inclusion criteria of the study, both techniques were available during the duration of the study period. Utilization of the robotic technique, however, increased over that time period from 29% of minimally invasive RNU in 2010 to 53% in 2016. The robotic data may reflect some element of the learning curve for the surgeons transitioning from the laparoscopic to robotic techniques.
A particular strength of this study is what it reveals about practice patterns. Patients who received RRNU were nearly twice as likely (35% vs 19%) as those undergoing LRNU to receive a lymphadenectomy in clinically node-negative patients and had increased node yield. Patients who underwent surgery at academic and integrated network cancer centers had improved survival, likely due to more experience with a relatively rare disease such as UTUC. It is also interesting that academic centers are more likely to perform an LND at the time of RNU. It is possible that those at academic centers are more convinced of the data indicating that value of lymphadenectomy may be attributable to better characterization of disease.
Our study also found that neoadjuvant chemotherapy was a significant predictor of performance of LND. The rapidly changing landscape of perioperative chemotherapy may change prevailing thinking on the value of LND at the time of RNU. The POUT trial 16 has demonstrated a nearly 20% improvement in disease-free survival (OS data not yet reported) in patients who receive adjuvant chemotherapy following RNU. These investigators noted this effect even among patients with node-negative disease. As adjuvant chemotherapy has become the standard of care, questions remain regarding the prognostic value of nodes removed at the time of RNU.
The increasing use of neoadjuvant chemotherapy before RNU may also affect the decision whether to perform concomitant LND, as noted in our observation that neoadjuvant chemotherapy is an independent predictor of LND. Eastern Cooperative Oncology Group (ECOG)-8141 (Ref. 17 ) demonstrated a 14% complete pathologic response rate at time of RNU among those who received neoadjuvant chemotherapy. Going forward, it will be important to determine if lymphadenectomy among these patients confers additional benefit given the receipt of consolidative therapy before surgery. However, given the lack of granularity in our data set, we are not able to address these questions of ideal timing and administration of chemotherapy.
Conclusions
RRNU demonstrated increased rates of LND and may be associated with improved short-term morbidity and possibly mortality rate robotically. Improved OS may be due to better characterization of the disease burden with LND. Further prospective studies are needed to determine the role of LND and timing with regard to chemotherapy in clinically localized UTUC.
Footnotes
Author Disclosure Statement
There are no disclosures pertaining to this article.
Funding Information
No funding was received for this article.
Supplementary Material
Supplementary Table S1
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.