
Abstract
Objective:
To investigate the outcomes of retrograde flexible ureteroscopy in managing parapelvic renal cysts and speculate the factors affecting therapeutic efficacy.
Methods:
Thirty-eight patients with parapelvic renal cysts were recruited and underwent retrograde flexible ureteroscopy using holmium laser. Parapelvic cysts were divided into peripheral type and central type based on the position of cyst convex to the perirenal tissue. Feasibility and safety were retrospectively evaluated, and cases were analyzed to detect their distinctive characteristics. Independent-sample t-test and chi-square test were undertaken for continuous variables and categorical variables, respectively.
Results:
Radiologic evidence of success was achieved in 31 (81.58%) cases after a mean follow-up of 14.4 months (range 6–26 months). No significant perioperative complications were identified. There were seven cases with features of peripherally located parapelvic cyst. Four cysts shown as irregular protrusion were unable reduce to less half of previous size. Reductions were recorded in the other three patients with spherically peripheral protrusion. There was significant difference between these two types (p = 0.029). Among the 31 patients with centrally located parapelvic cyst, 28 of these have simple cysts that achieved radiologic success and 3 of the 31 patients were identified as failed cases indicated by renal pelvis enveloped by cyst on radiologic investigation. The success rate of simple cysts was significantly higher than that of the later type (p < 0.001).
Conclusion:
The location and shape of parapelvic cyst may play a critical role in the radiologic outcome of internal incision and patients with simple central or spherical peripheral cyst may benefit more from retrograde flexible ureteroscopy combined with laser incision.
Introduction
Most parapelvic renal cysts are incidental findings that are generally asymptomatic. As they are closely associated with the urinary system, they can be manifested as renal obstruction. The most commonly reported symptoms are lumbar discomfort, followed by urinary tract infection (9.5%) and hematuria (4.8%). 1 Other potential consequences of parapelvic cysts include renal calculi, vascular compression, renin-mediated hypertension and spontaneous hemorrhage. 2,3 Enhanced CT is the best method for the diagnosis of parapelvic cysts. Although laparoscopic renal-sparing cyst excision, de-roofing, decortication, and ablation are the most effective and minimally invasive methods for the treatment of renal cysts, 4 the specific anatomical structure of parapelvic cysts leads to increasing difficulty in operation and the associated surgical complications. Flexible ureteroscope and holmium laser for treatment of parapelvic cysts is a growing trend in recent years with increasing cases reported. 5 –7 The retrograde approach is effective and has a low complication rate. Other benefits include its minimally invasive nature and a short hospital stay after surgery. However, uncertainty now exists regarding which specific subgroups of patients will benefit more from this procedure and the outcome of this method remains unclear. To evaluate factors influencing surgical outcome and explore predictors of therapeutic effectiveness, we report our dynamic follow-up results of retrograde flexible ureteroscopy in managing parapelvic renal cysts.
Materials and Methods
Patients recruitment
Contrast-enhanced CT was performed to establish the diagnosis of parapelvic renal cysts in all patients preoperatively. One hundred and one cases with parapelvic renal cysts were included in our department from May 2017 to August 2019. Of those patients, 38 cases were selected and treated by retrograde flexible ureteroscopy using holmium laser. Parapelvic cysts were divided into peripheral type and central type based on the location of cyst convex to the perirenal tissue. Patients were further categorized into spherical or irregular group according to the morphology for those with peripheral type. The central type was also divided into simple or enveloped type based on the adjacent relationship between cyst and renal pelvis. Inclusion criteria were as follows: (1) presence of hydronephrosis caused by cyst or compression of the renal pelvis or calix; (2) presence of cyst diameter >3 cm; (3) presence of renal calculi or ureteral calculi; and (4) patients with complaints of flank pain, hematuria, and repeated infection. The study excluded patients with suspected ureteral strictures, urosepsis, ureteral/pelvic tumors, or those who could not tolerate lithotomy position. In addition, patients were excluded if they had severe cardiopulmonary disease or bleeding disease. The study was approved by the Ethics Committee of Ruijin North Affiliated Hospital of Shanghai Jiaotong University School of Medicine.
Methods
6F D-J tube (Cook) was placed in all patients at least 2 weeks before surgery. General anesthesia was carried out and patients were under lithotomy position. An 8/9.8F rigid ureteroscope (KARL STORZ) was inserted into bladder to remove the D-J tube with foreign body forceps. Afterward, a 12F ureteral access sheath (Innovex) was introduced over a guidewire (HWS-035150; Cook). Electronic flexible ureteroscope (11278V; KARL STORZ) was placed to locate the parapelvic cyst, then a 200 μm holmium laser fiber (VersaPulse®, PowerSuite™, Holmium 60 W; Lumenis) set at 0.8 J with 30 Hz was inserted to open the renal pelvis and cyst wall in turn. The place of the most proximity between parapelvic cyst and pelvis was identified as a bluish impression over the milky renal pelvic tissue. Ultrasonography was used to guide the direction when the location of the cyst cannot be identified endoscopically (Fig. 1). Typically, the membrane of renal pelvis is separated from cyst wall with loose fibrosis tissue (Fig. 2). Pyelotomy is performed to fully expose the cysts before the incision. In some patients, two layers were infused and could be incised simultaneously. The flexible ureteroscope was inserted to inspect the condition of cyst cavity and reveal no pathologic findings. Endoscopic de-roofing was performed to open the window of parapelvic cyst as large as possible using laser (Fig. 2). Lithotripsy was performed in advance for patients with ipsilateral renal calculi. Stone free was guaranteed before the intrarenal incision. Finally, a 6F D-J tube was placed in the affected ureter, and the catheter tip was introduced into the cyst cavity (Fig. 2). The catheter was removed 1 month later. All patients underwent surgeries under one surgeon with >10 years of surgical experience and had performed >1000 flexible ureteroscopy procedures.
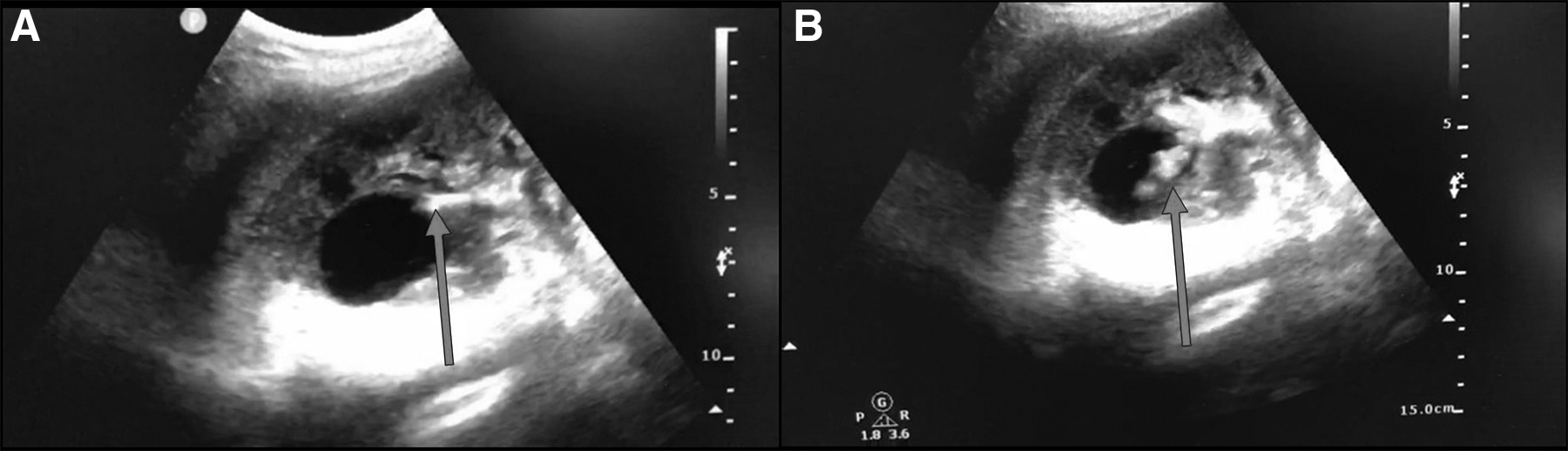
Ultrasonography-guided flexible ureteroscopic management of parapelvic renal cyst [the tip of flexible ureteroscope is shown by the arrow in
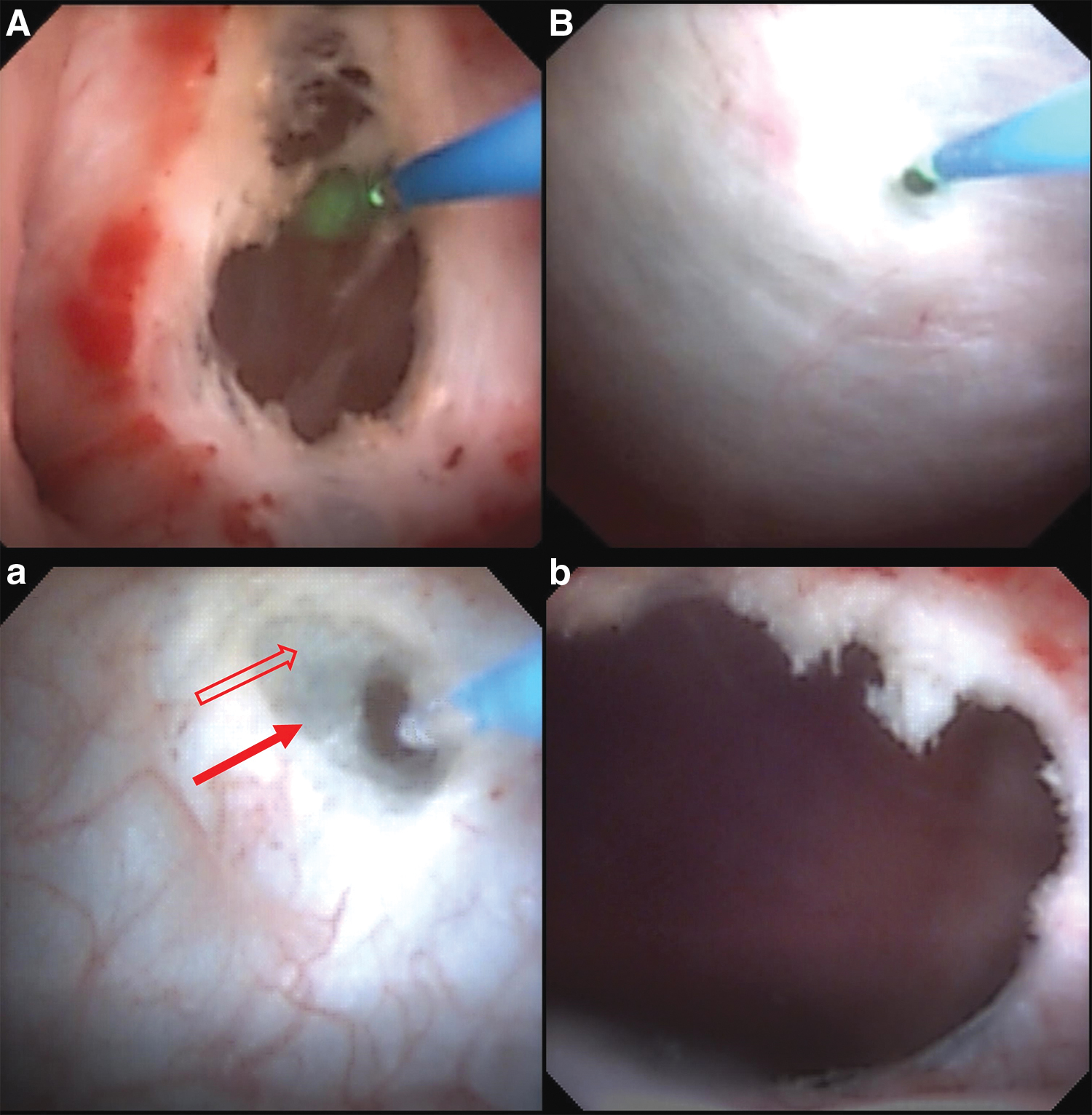
Endoscopic view of different adjacent relationship between cyst and pelvis.
All patients underwent follow-up in outpatient clinics. CT scan or Doppler ultrasonography was performed on the first day and 1 month postoperative, and then for an interval of every 6 months. Radiologic success was defined as a decrease in cyst size of at least half of the initial maximal diameter after a minimum of 6 months follow-up. 8
Statistical analyses
SPSS19.0 statistical software was used for data analysis. Continuous variables and categorical variables were expressed as mean ± standard deviation and n (%), respectively. Independent-sample t-test was carried for continuous variables and chi-square test for categorical variables. p < 0.05 was defined as a statistically significant difference.
Results
Baseline characteristics and perioperative events
The study recruited 38 patients who met the inclusion and exclusion criteria with 17 men and 21 women. Baseline characteristics of patients are seen in Table 1. All surgeries were uneventful. No severe hemorrhage, urosepsis, interruption of surgery, or conversion to open surgery was recorded in any patients. Blood clots in cyst cavity was shown in two patients on day 1 postoperative but were completely resolved during the following month. Ultrasonography guidance was required for the procedure in five cases. Of the 24 patients with urinary stones, we achieved one-procedure stone-free rate (SFR) of 95.83%. Significant relief of back pain was recorded in 9 of 11 patients (81.82%) 1 month postoperatively after removal of D-J tubes.
Initial Characteristics of Patients with Parapelvic Cysts Using Ureteroscope and Holmium Laser
SD = standard deviation.
Outcome analysis
Radiologic success was achieved in 31 of 38 patients (Table 2). Among the seven cases with peripheral parapelvic cyst, four of them showed an irregular protrusion and cyst size did not reduce to half of the previous size (Fig. 3). However, optimal results were recorded in three patients with spherically peripheral protrusion. The difference was found to be statistically significant between these two types (p = 0.029). Thirty-one patients demonstrated centrally parapelvic cyst. For these cases, there were 28 patients who had reached the criteria for radiologic success. We also noted that three cases had an undesirable outcome with residual cyst >50% of original size and they were characterized with renal pelvis enveloped by cyst from both sides. (Fig. 4). The success rate of simple ones was significantly higher than that of later type (p < 0.001).
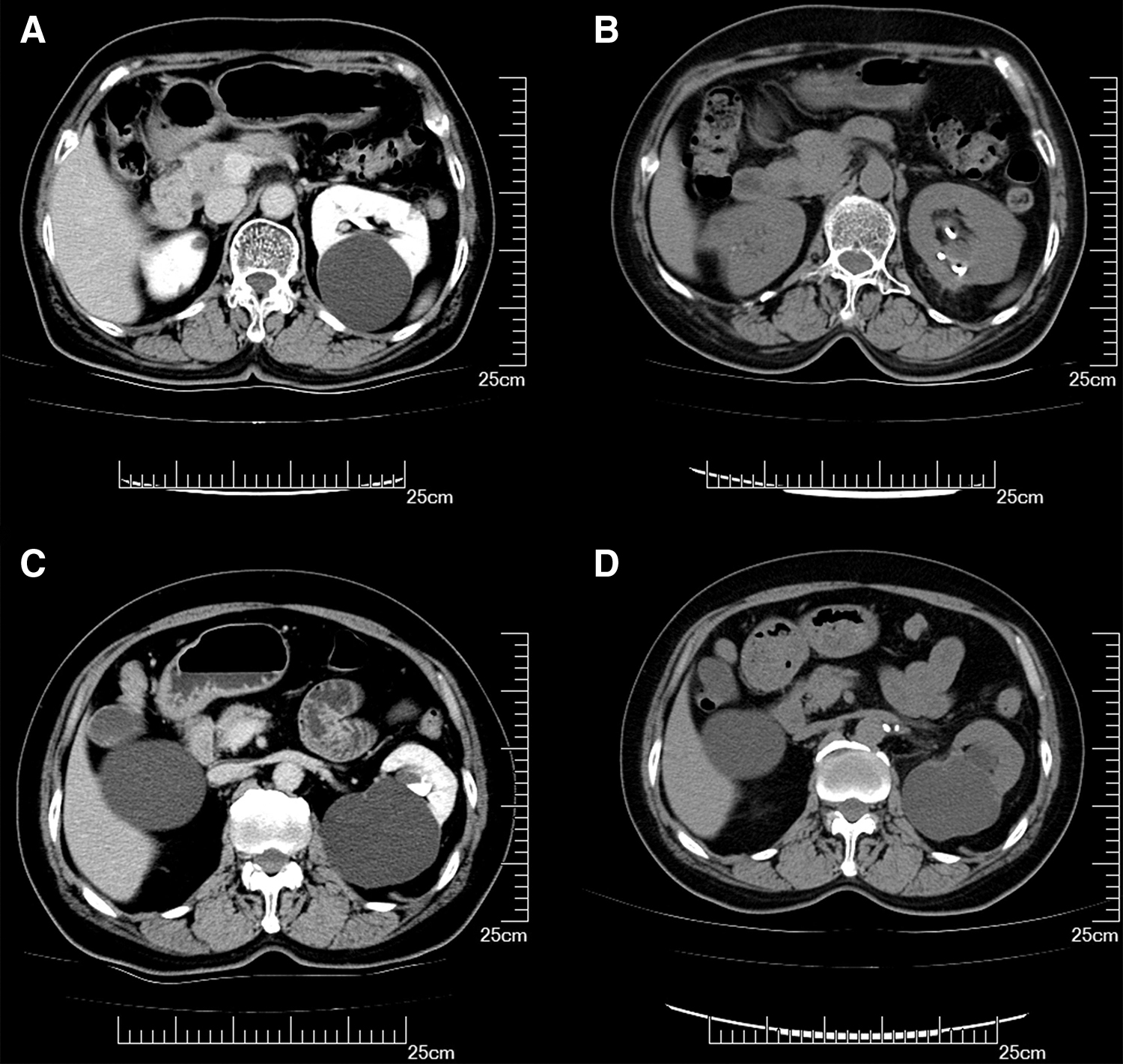
Pre- and postoperative CT scan for patients with peripherally parapelvic cyst shown as a spherical
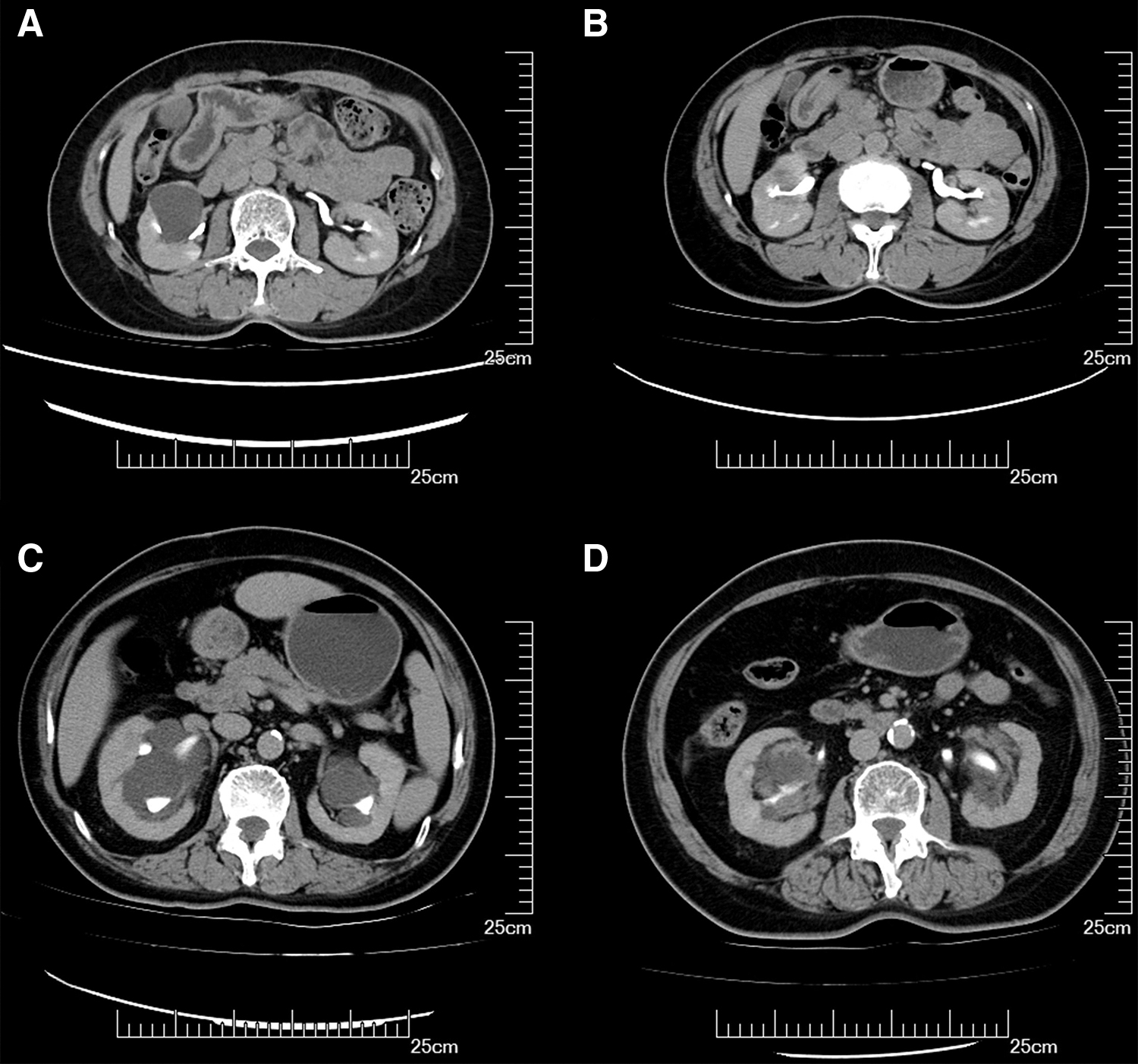
Pre- and postoperative CT scan for patients with centrally parapelvic cyst shown as simple type
Clinical and Perioperative Characteristics of Patient Stratified by Radiologic Outcome Postoperatively
p < 0.05.
SFR = stone-free rate.
Follow-up
Optimal operative outcome was observed in 73.68% patients with >50% size reduction of renal cyst on day 1 of postoperative period. During subsequent follow-up periods, the proportion of effective performance reached 81.58% at the last follow-up. None of these patients experienced recurrence during a mean 14.4 months follow-up period (range 6–26 months).
Discussion
The purpose of surgical treatment of parapelvic cyst is to drain the contents of the cyst and prevent further compression to renal pelvis and parenchyma. There are various surgical approaches such as percutaneous puncture, sclerosing agent injection under the guidance of B ultrasonography or CT, incision and de-roofing by opening or laparoscopy and robotic surgery, 9 –12 but each approach has its own advantages and disadvantages. Although laparoscopic incision and de-roofing is the gold standard for renal cyst, there is increasing probability of damaging the renal blood vessels and collecting system because of the deep location of parapelvic cysts. The proximity between the parapelvic cyst and the renal pelvis or calix anatomically makes ureteroscopy in the treatment of parapelvic cyst possible. In our study, we first identified various anatomical relationship between renal pelvis and parapelvic cyst. Typically, the membrane of renal pelvis is separated from cyst wall by fibrosis tissue. In addition, endoscopic view showed that the pelvic membrane and cyst wall was fused into one layer in other patients. The distinct anatomical relationships will pose specific challenges with regard to the discovery of cyst, especially for patients with separated structure whose cyst may not typically present bluish impression under endoscopic view. It has been confirmed that ultrasonography will contribute to the detection of these cysts in our study.
Technology related to flexible ureteroscopes has achieved rapid advances in the past few years that rendered it the mainstay of therapy in many urologic disease such as stone diseases and ureteral lesions. 13 –15 The feasibility of retrograde marsupialization in an obstructing renal sinus cyst by flexible ureteroscopy was first described by Kavoussi and colleagues. 16 Since then, the feasibility and safety of retrograde intrarenal laser incision (RIR-LI) in parapelvic cysts have been validated by varied research. 17 –19 Ureteroscopy is a less invasive option in managing parapelvic cyst compared with the gold standard of laparoscopic surgery. Moreover, there are additional benefits in obese patients as well as patients with previous abdominal or retroperitoneal surgery. Particularly, superiority was demonstrated for patients with parapelvic renal cyst accompanied by ipsilateral renal stones: killing two birds with one stone. 7,20 In our study, 24 patients underwent simultaneous RIR-LI and lithotripsy. The SFR of a single procedure was 95.83% (23/24). It is noted that lithotripsy should be performed first to achieve stone free followed by RIR-LI. This can prevent stone fragments from falling into the cyst cavity, which makes stone removal technically challenging.
Although RIR-LI appears to have considerable evidence in parapelvic cyst management, patients usually show distinctively therapeutic outcome in the same range of cases or across studies. 6,20,21 Failed cases were also reported in different studies. 8,19,22 However, few authors had explored the underlying factors impacting operative outcomes. Shen and colleagues presumed that the radiologic failure was attributed to the larger renal cysts and smaller incision of cyst wall in operation. 19 In our research, parapelvic cyst was first divided into different types based on the location of cyst convex to the perirenal tissue and the outcome of specific type was retrospectively analyzed. There was significant difference in the reduction of cyst size in subgroups with various location and shape. Based on the results, we considered that cyst tension and enough support from renal parenchyma may accumulatively play vital roles in determination of the decrease of cyst size using retrograde flexible ureteroscopy. Owing to lack of support from surroundings, peripherally parapelvic cysts are difficult to fully retract postoperatively, especially for patients with irregular protrusion, which is featured with poor tension. Spherical protrusion is an indicator of greater tension compared with irregular model, which may explain spherically peripheral cyst decreased significantly in size. For patients with central parapelvic cysts characterized with renal pelvis enveloped, there was effectively bidirectional support from renal parenchyma. However, this subgroup of cysts had been conventionally incised from a unilateral approach. Hence the release of pressure may be diminished by contralateral pelvic wall that leads to incomplete resolution of cyst.
To evaluate the therapeutic efficacy of ureteroscopic incision, we had performed a dynamic follow-up. CT scan is performed in all patients on day 1 postoperative to establish the initial therapeutic efficiency and update patients regarding the outcome before their discharge. In addition, it can be used to determine whether the D-J tube is in position and whether hemorrhage occurs in the renal pelvis or cyst cavity. The former impacts on whether prolonged internal drainage is required to keep the channel patent. 7 To the best of our knowledge, no study has assessed the radiologic appearance on the first day postoperatively.
The limitations of this study are addressed as follows. First, we had taken a retrospectively observational analysis with limited sample size. Further prospective randomized controlled study should be planned to evaluate long-term outcomes of RIR-LI in different subgroups of parapelvic cysts. In addition, the duration of follow-up period may not be sufficient to definitely determine the operative outcome of different parapelvic cyst types. Finally, we could not perform pathologic analysis during the procedure to obtain gold standard diagnoses.
Conclusion
The location and shape of parapelvic cyst may play a critical role in the decompression and reduction of parapelvic renal cyst by RIR-LI. Patients with different subtypes of parapelvic renal cysts demonstrate distinctive effectiveness. This minimally invasive approach could be a safe and effective alternative for selected patients who has simply central cyst or peripheral cyst with spherical shape.
Footnotes
Author Disclosure Statement
The authors declare that there is no conflict of interest.
Funding Information
No funding was received for this article.