
Abstract
Background:
MRI-guided transurethral ultrasound ablation (TULSA) offers minimally invasive thermal ablation of benign and malignant prostate tissue, using directional high-intensity ultrasound and real-time, magnetic resonance thermometry feedback control. Feasibility of TULSA for alleviating lower urinary tract symptoms (LUTSs) associated with benign prostatic hyperplasia (BPH) is retrospectively assessed in a subgroup of men from a localized prostate cancer study who also had LUTSs.
Patients and Methods:
TULSA was used to ablate 90% of the prostate gland in 30 men with localized prostate cancer, without plans to spare ejaculatory ducts. Mean ± standard deviation treatment time was 37 ± 10 minutes. Retrospective analysis was conducted on a subpopulation of nine patients who also suffered from LUTSs (International Prostate Symptom Score [IPSS] ≥ 12 at baseline) as well as a smaller subgroup of five patients with IPSS >12 and peak urinary flow (Qmax) <15 mL/second. Urinary symptom relief, continence, and erectile function were assessed using IPSS, International Index of Erectile Function (IIEF), and uroflowmetry.
Results:
At 12 months post-TULSA, IPSS improved significantly by 58% to 6.3 ± 5.0 (p = 0.003), with at least a moderate (≥6 points) reduction in eight of nine patients. IPSS quality of life improved in eight of nine patients. Erectile function (IIEF-EF) remained stable from 14.6 ± 9.3 at baseline to 15.7 ± 9.0 at 12 months. The proportion of patients with erections sufficient for penetration (IIEF Q2 ≥2) was unchanged. Full urinary continence (pad free and leak free) was achieved at 12 months in all patients. In five men who suffered from more severe symptoms, Qmax increased from 11.6 ± 2.6 mL/second to 22.5 ± 14.2 mL/second at 12 months (p = 0.126). Perfused prostate volume, measured on MRI, decreased 70% to 13.6 ± 4.6 mL (p = 0.003) at 12 months. All adverse events were mild to moderate (Common Terminology Criteria for Adverse Events [CTCAE] Grade 1–2) with no serious events reported.
Conclusions:
This retrospective analysis demonstrates promising safety and feasibility of TULSA to relieve LUTSs, with improvement in IPSS comparable with modern, minimally invasive surgical therapies. Larger controlled studies with BPH-specific ablation plans in men seeking treatment for LUTSs are warranted.
Introduction
Benign prostatic hyperplasia (BPH) is a prevalent age-associated condition estimated to affect 50% of men over the age of 50 and 75% of men over the age of 70. 1,2 Clinically significant BPH is typically associated with incomplete bladder emptying, weak urinary stream, frequent urination, and several other lower urinary tract symptoms (LUTSs). 3 Mild to moderate BPH can be conservatively managed with watchful waiting and lifestyle modifications or with medications such as α-blockers, 5α-reductase inhibitors, and PDE5 inhibitors. 4 Severe BPH can be managed through gold standard surgical interventions, including transurethral resection of the prostate (TURP) or open simple prostatectomy for larger prostates, which are associated with perioperative complications and morbidity. 5 A comprehensive meta-analysis of 23 randomized controlled trials evaluating TURP observed adverse event rates of as much as 21% for urethral stricture, 13% for retention requiring recatheterization, 38% for urinary urgency, 7.7% for intraoperative bleeding, and 9% for blood transfusion and as many as 4 days of hospital stay. 6 Hence, in the spirit of reducing adverse events and unwanted complications such as erectile/ejaculatory dysfunction, new minimally invasive treatments such as convective radiofrequency water vapor therapy (Rezum) and prostatic urethral lift (UroLift) are more frequently utilized. 7 However, while effective in relief of BPH symptoms, these minimally invasive procedures are limited in scope for patients with smaller prostates (<80 mL) and without concurrent cancer diagnosis.
With more than 1.3 million new cases in 2018, prostate cancer is the second most prevalent cancer in men, the majority of whom are diagnosed with low or favorable intermediate-risk disease. 8,9 These patient groups are increasingly being managed with active surveillance, 10 –12 which (as they age) leads to a growing number of cancer patients who suffer from concurrent BPH symptoms. Therefore, there is an unmet need for development of less invasive ablative treatments with minimal side effects, which can be used effectively to treat patients with BPH and coexisting prostate cancer, or large-volume BPH, who are managed with invasive treatments such as open simple prostatectomy.
MRI-guided transurethral ultrasound ablation (TULSA) is a novel minimally invasive treatment for customizable prostate tissue ablation using high-intensity directional ultrasound controlled by real-time, magnetic resonance (MR) thermometry feedback. TULSA effectively decreases prostate volume through thermal ablation and has previously demonstrated safety and efficacy in patients with localized prostate cancer. 13,14 As such, TULSA has great potential to be used as a minimally invasive treatment modality for selected patients with LUTSs due to BPH.
We previously reported on a Phase I study demonstrating the safety and precision of MRI-guided TULSA in 30 patients with low- to intermediate-risk, organ-confined prostate cancer. 13 In this study, we present a retrospective analysis of LUTSs in a subgroup of these patients who suffered from LUTSs in addition to their cancer at baseline.
Patients and Methods
Study protocol
A prospective, multicenter, single-arm Phase I study evaluated the safety and feasibility of MRI-guided TULSA for prostate tissue ablation in patients with low- and intermediate-risk prostate cancer. 13 Between March 2013 and March 2014, adult men aged ≥65 years with organ-confined prostate cancer (clinical stage T1c–T2a, Gleason score 3 + 3 or 3 + 4, and PSA ≤10 ng/mL) were consented to enroll in the study. Research ethics boards at three tertiary urology centers in Canada (London, Ontario), Germany (Heidelberg), and the United States (Royal Oak, Michigan) approved the study (NCT01686958, DRKS00005311).
Patient selection, exclusion criteria, and the TULSA technique have been previously described by Chin and colleagues. 13 Briefly, 30 patients were included in the study. International Prostate Symptom Score (IPSS) and International Index of Erectile Function (IIEF) questionnaires were used at baseline and 1-, 3-, 6-, and 12-month intervals to assess their LUTSs and erectile function. Uroflowmetry and MRI were performed at baseline and 12 months. From this study population, a subgroup of 9 of 30 men with baseline IPSS ≥ 12 and a smaller subgroup of 5 of 30 patients with baseline IPSS ≥ 12 and Qmax (peak urinary flow) ≤15 mL/second were considered as the patients with LUTSs in addition to their prostate cancer at baseline. While this Phase I study includes follow-up of 5 years, longer-term outcomes are beyond the scope of this feasibility assessment with focus on 12-month safety and effectiveness and will be reported separately.
MRI-guided TULSA procedure
MRI-guided TULSA (TULSA-PRO; Profound Medical, Mississauga, Canada) is delivered using a transurethral ultrasound catheter, while thermal treatment is automatically monitored and controlled by closed-loop, MR thermometry feedback. The treating physician prescribes the ablation volume by drawing boundaries on intraoperative, prostate MR images (Fig. 1), followed by robotically controlled delivery of directional ultrasound energy through a sweeping rotation around the urethra. Each TULSA procedure was performed by a team, including a urologist, radiologist, anesthesiologist, MRI technologist, and nurse assistant.

TULSA. Tissue ablation is delivered using a transurethral probe that contains 10 high-intensity ultrasound elements (top left corner). The ablation volume is prescribed by the treating physician by drawing boundaries on prostate MR images in TULSA-PRO software (top row). Using real-time MR thermometry, the TULSA-PRO system calculates the exact energy required for tissue ablation at each moment of treatment (lower left corner), automatically ablates the tissue through 360° sweeping rotation around the urethra, and monitors the entire process. Treatment effectiveness can be instantaneously measured at the end of the procedure through final thermal map coverage of prostate (middle row) or contrast-enhanced MRI (bottom row). The yellow line indicates the targeted prostate boundary and the green line indicates the ablation limit, which is matched with the nonperfused tissue border in the bottom row. MR = magnetic resonance; TULSA = MRI-guided transurethral ultrasound ablation.
The entire process of ablation is automated and controlled through closed-loop temperature feedback from real-time, MR thermometry scans. Based on the thermal images, the TULSA system calculates and delivers the exact ultrasound energy required for precise and conformal tissue ablation. The high-resolution MR images used in the planning phase, along with the millimeter accuracy of ablation delivered by the TULSA system, provide the treating physician with the unique ability to customize the ablation plan to each individual patient's disease and needs. In doing so, the natural function of critical structures, such as nerve bundles or ejaculatory ducts, can be preserved by excluding them from the target boundary. Additionally, the transurethral catheter is cooled, providing periurethral tissue preservation. In this study, the treatment plan was designed to achieve near whole-gland ablation (90% of the inner core of the prostate) in patients with localized prostate cancer and did not attempt to preserve the ejaculatory ducts, as one could if the treatment goal was only to alleviate LUTSs.
Statistical analysis
Safety and efficacy outcomes, including frequency and severity of adverse events, changes in MRI-measured prostate volume, quality of life (QoL; IPSS and IIEF-EF [erectile function] domain), and uroflowmetry, were summarized by their mean and standard deviation (SD) and compared with baseline using Student's t-test, with p < 0.05 considered statistically significant. Among the nine patients with baseline IPSS ≥ 12, all completed the 6-month follow-up and eight completed the 12-month follow-up. Missing data were imputed using the last observation carried forward method for one patient who did not complete the 12-month follow-up.
Results
Demographics
Baseline patient characteristics are summarized in Table 1. Mean ± SD ultrasound treatment time was 37 ± 10 minutes. In the nine-patient subgroup with LUTSs (IPSS ≥ 12), mean age was 70.1 ± 2.9 years, baseline IPSS was 16.1 ± 3.8, pretreatment prostate volume as measured by T2-weighted MRI was 54.0 ± 23.2 mL, postvoiding residual (PVR) volume at baseline was 95.0 ± 117.8 mL, and peak urinary flow rate (Qmax) was 14.5 ± 4.1 mL/second. The five-patient subgroup with more severe LUTSs (IPSS ≥ 12 and Qmax <15 mL/second) had a baseline IPSS of 17.8 ± 4.3, PVR of 80.3 ± 56.0 mL, and peak flow rate of 11.6 ± 2.6 mL/second. Mean catheterization time was 3.1 ± 1.8 weeks. Patients who were concurrently taking medications with antiandrogen properties, over-the-counter or herbal preparations, any investigational anabolic steroids or corticosteroids, or any investigational 5 alpha-reductase inhibitors were not included in this study.
Comparing Baseline and 12-Month Data for the Nine-Patient Subgroup with Lower Urinary Tract Symptoms (International Prostate Symptom Score ≥12) and the Five-Patient Subgroup with More Severe Lower Urinary Tract Symptoms (International Prostate Symptom Score ≥12 and Qmax < 15 mL/Second)
IIEF = International Index of Erectile Function; IIEF-EF = International Index of Erectile Function–erectile function; IPSS = International Prostate Symptom Score; LUTS = lower urinary tract symptom; PVR = postvoiding residual; Qmax = peak urinary flow.
Lower urinary tract symptoms
Postablation IPSS in the nine-patient subgroup improved significantly by 9.1 ± 7.1 points, from 16.1 ± 3.8 at baseline to 6.3 ± 5.0 at 12 months (p = 0.003) (Fig. 2A). Improvement is demonstrated at the 3-month time point and continues to improve through to 12 months. At 12 months, at least a moderate (≥6 points) reduction in symptoms was experienced by eight of nine men, with eight of nine also experiencing IPSS reduction >30%, and symptoms of seven of nine men were reclassified from moderate to normal (mild) (IPSS ≤7). IPSS QoL improved significantly from 2.8 ± 1.1 at baseline to 0.8 ± 1.0 (p = 0.007) at 12 months, with seven of nine men reporting that mixed or worse at baseline improved to pleased or delighted (Fig. 2B). PVR improved significantly from 95.0 ± 117.5 mL at baseline to 62.5 ± 88.2 mL at 12 months despite a large SD (p = 0.042) (Fig. 2C). Qmax increased from 14.5 ± 4.1 mL/second at baseline to 21.9 ± 12.7 mL/second at 12 months, but did not reach statistical significance (p = 0.126) (Fig. 2D). In the five-patient subgroup with more severe symptoms, mean ± SD IPSS improved from 17.8 ± 4.3 at baseline to 4.4 ± 2.1 at 12 months, QoL score improved from 3.0 ± 1.2 to 0.4 ± 0.5, PVR decreased from 80.3 ± 56.0 to 52.2 ± 38.8 mL, and Qmax increased from 11.6 ± 2.6 to 22.5 ± 14.2 mL/second (Table 1). In the complete, single-arm, Phase I study population (N = 30), there were no significant changes in IPSSs (from 9.0 ± 5.6 at baseline to 6.6 ± 5.2 at 12 months) or Qmax (from 14.3 ± 5.6 to 16.9 ± 10.0 mL/second). Similarly, there were no significant changes among the patients with IPSS <12 at baseline (IPSS stable from 6.0 ± 2.8 to 6.5 ± 5.4 at 12 months and Qmax unchanged from 14.2 ± 6.2 to 15.8 ± 9.4 mL/second).
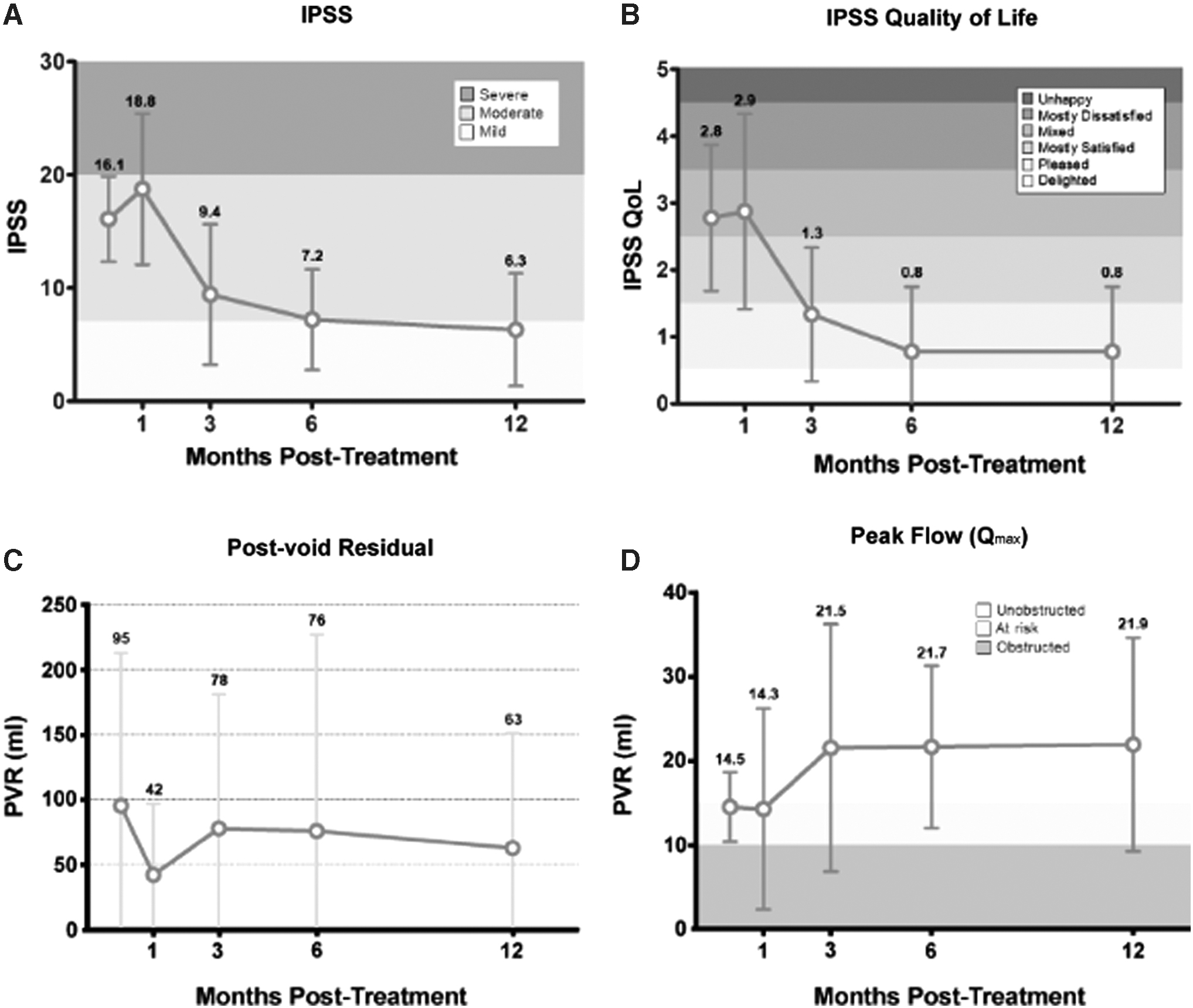
Temporal trend in urinary symptoms, quality of life, and urodynamic data, from baseline through 12 months. Mean ± SD values of the subgroup of nine patients with symptomatic BPH at baseline (IPSS ≥ 12).
Prostate volume
Prostate volume was measured on MRI at 12 months, including any regions of nonperfused prostate tissue and fibrosis. In the nine-patient subgroup, mean prostate volume decreased from 54.0 ± 23.2 mL at baseline to 23.9 ± 7.8 mL at 12 months (p = 0.003). In this subgroup, the largest prostate volume before TULSA was 96.7 mL, and the mean ± SD transition zone volume was 28.0 ± 15.3 mL, corresponding to 51% ± 10% of the gland. Excluding nonperfused regions within the prostate, prostate volume decreased over 70% to 13.6 ± 4.6 mL at 12 months. The residual prostate volume at 12 months contained an expected presence of enhancing fibrous tissue, ranging from 17% to 84% of the total remaining volume measured by transrectal ultrasound-guided biopsy.
Cancer treatment outcomes
In the nine-patient subgroup, mean ± SD PSA reduction of 96% ± 64% and nadir of 0.75 ± 0.5 ng/mL were similar to the overall 30-patient population (PSA reduction of 88% ± 10% and nadir of 0.69 ± 0.6 ng/mL). In the nine-patient subgroup, 12-month post-treatment 12-core biopsy was positive in 3 of 8 patients (2 Grade Group 2, 1 Grade Group 1), excluding 1 patient with stable 12-month PSA of 0.2 ng/mL who refused follow-up biopsy and withdrew from the study.
Erectile function and safety outcomes
In the nine-patient subgroup, the IIEF-erectile function domain score (IIEF-EF) remained stable from mean ± SD of 14.6 ± 9.3 at baseline to 15.7 ± 9.0 at 12 months (Fig. 3). The proportion of patients with erections sufficient for penetration (IIEF Q2 ≥2) also remained stable, from seven of nine at baseline to eight of nine at 12 months. Only one patient reported retrograde ejaculation. Full urinary continence (pad free and leak free) was achieved at 12 months in nine of nine patients. In the five-patient subgroup with more severe LUTSs, mean ± SD IIEF-EF was 16.0 ± 10.7 at baseline and 19.0 ± 11.1 at 12 months.
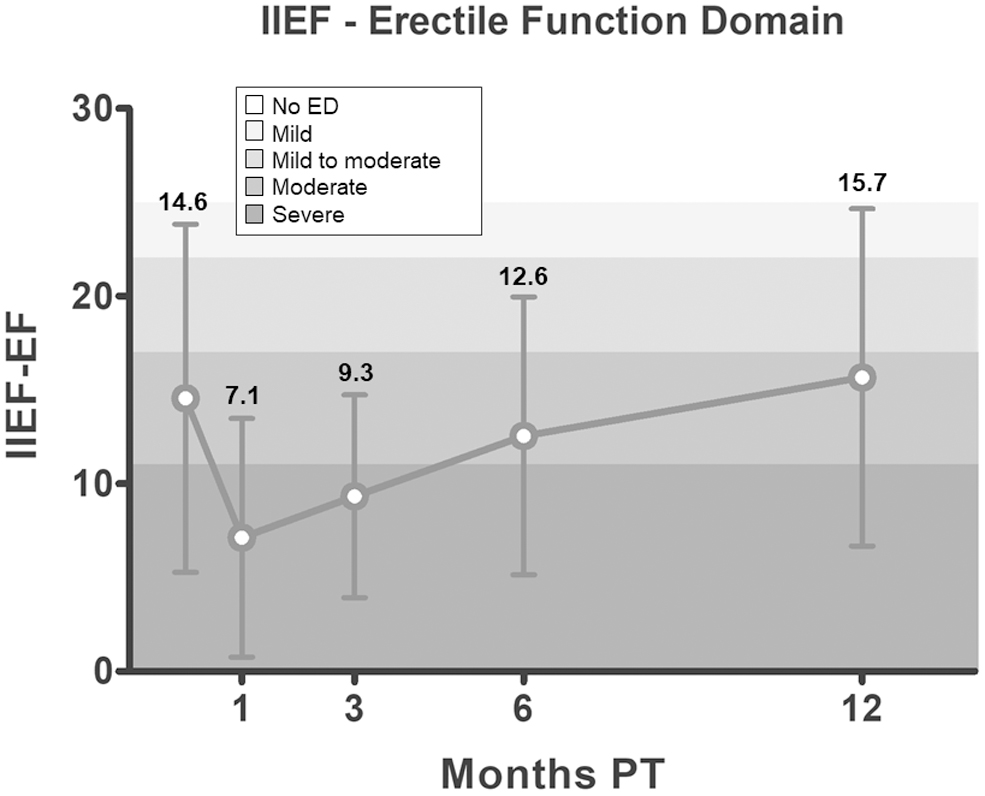
Temporal trend in IIEF-erectile function domain, from baseline through 12 months. Mean ± SD values of the subgroup of nine patients with symptomatic BPH at the baseline (IPSS ≥ 12). IIEF = International Index of Erectile Function.

Summary of treatment planning and 12-month follow-up T2-weighted axial images for the patient depicted in Figure 1. Pretreatment prostate volume was 82 mL, transition zone corresponded to 66% of total volume. At 12 months follow-up, a 93% reduction in prostate volume and 94% reduction in PSA were observed (PSA nadir at 12 months: 0.20 ng/mL). At 6 months, his IPSS improved from 7 to 2 points and Qmax from 13.8 to 39.8 mL/second.
All adverse events were mild to moderate (Common Terminology Criteria for Adverse Events [CTCAE] Grade 1–2) and no severe or serious adverse events were reported. The most common adverse events included urinary tract infection (UTI; three of nine patients), urinary urgency (three of nine patients), urinary retention (three of nine patients), and hematuria (three of nine patients), the majority of which were resolved by 1 month. Only one adverse event (ejaculatory disorder) was ongoing at 12 months. Supplementary Table S1 summarizes all adverse events.
Discussion
In a subgroup of patients presenting with symptomatic BPH at baseline, conformal prostate ablation using MRI-guided TULSA effectively alleviated LUTSs with a reasonable side effect profile. The primary measure of LUTSs, the IPSS, significantly improved from baseline to 12 months, on average decreasing by 9.8 points from 16.1 to 6.3. At 1 month after TULSA, there is a nonsignificant increase in IPSS by 24%, but improvement becomes significant by 3 months with a decrease of 35%. Peak improvement in IPSS was observed at 12 months with a decrease of 58%, similar to that demonstrated with TURP and other published tissue removal surgical procedures. There was a notable improvement in Qmax from 14.5 at baseline to 21.9 mL/second at 12 months after TULSA, although it did not reach statistical significance due to the small sample. The safety of the TULSA procedure was demonstrated in this subgroup of patients with no serious adverse events, and the majority of events resolved at 1-month follow-up. All Grade 2 adverse events were expected events, including UTI, urinary retention, urinary urgency, and hematuria, which were all resolved by 1 month, except for one case with urinary urgency that lasted 3 months and one case with ejaculatory disorder ongoing at 12 months (Supplementary Table S1). Furthermore, all patients remained leak free and pad free at 12 months. Patients maintained erectile function (from seven of nine at baseline stable to eight of nine at 12 months) and one of nine patients suffered from retrograde ejaculation.
To contextualize the outcomes in this feasibility report, a comprehensive comparison with pivotal studies of modern BPH treatments is summarized in Table 2. Functional results of TULSA at 12 months are comparable with even the most effective treatments while having an acceptable rate of serious adverse events.
MRI-Guided Transurethral Ultrasound Ablation Functional Outcomes Compared with Other Minimally Invasive Treatments at 12 Months
Results were gathered from pivotal studies for the devices in question (urethral lift, water vapor, and aquablation) or from RCTs comparing the treatment with TURP (PVP and artery embolization).
Calculated IPSS change using baseline and 12 months' reported value.
TURP results were calculated by weighted average from a meta-analysis of 23 RCTs comparing M-TURP with various other treatments; only studies that had both baseline and 12-month data were included in the calculation for each outcome.
QoL = quality of life; RCT = randomized controlled trial; SAE = serious adverse event; TULSA = MRI-guided transurethral ultrasound ablation; TURP = transurethral resection of the prostate; UTI = urinary tract infection.
Although the selection criterion of IPSS ≥ 12 for this nine-patient subgroup analysis is similar to inclusion criteria of other large BPH studies, the mean baseline symptom severity was not as high. It is expected that a larger improvement in symptoms could be achieved in patients with more severe baseline symptoms, as observed in the more restricted five-patient subgroup with IPSS ≥ 12 and Qmax <15 mL/second. Another important consideration is the treatment plan delivered to these patients, which targeted the inner 90% core of the prostate circumferentially (360°) around the urethra, designed for the Phase I study in patients with localized prostate cancer. It is likely that a less aggressive treatment plan, for example, only targeting the prostate transition zone, could be effective for patients with LUTSs. Of notable interest in this technology is the precision of MRI-guided TULSA, which offers the flexibility to customize the ablation plan, to spare the ejaculatory ducts, or to cover a targeted index lesion of cancer. Although not all urinary symptoms in this study can be directly attributed to BPH due to prostate cancer coexistence, a single-institute database cohort of 1330 men (665 with prostate cancer) has shown that modern prostate cancer does not appear to be associated with worse LUTSs when compared with benign prostates of the same size. 23
Among these first patients with LUTSs who received TULSA, two had a prostate volume ≥80 mL. Transurethral delivery of energy from within the prostate may make TULSA suitable for patients with large and extra-large prostate volumes who would otherwise require simple prostatectomy for their BPH. To date, patients with prostate volumes as large as 252 mL have been treated for BPH symptoms with TULSA (unpublished data). Furthermore, the thermal ablative mechanism of action in TULSA makes it the preferred choice of treatment in patients who suffer from concurrent, organ-confined prostate cancer and LUTSs. Although this initial feasibility analysis showed statistically significant improvement in LUTSs, additional studies with prospective patient selection criteria, refined treatment plans, and larger samples are warranted.
Study Limitations and Conclusions
Although statistically significant and clinically relevant improvement of symptoms has been observed, this report was restricted to a small number of nine patients. In addition, because of concomitant cancer diagnosis in these patients, it is difficult to determine how many of the reported LUTSs were solely related to BPH disease. Accordingly, the whole-gland treatment plan for these patients was prescribed based on their primary diagnosis of prostate cancer rather than their BPH symptoms. This analysis, however, demonstrates the favorable safety and feasibility of TULSA to relieve LUTSs, with IPSS improvement comparable with other modern, minimally invasive surgical therapies. Despite limitations of the study, considerable relief of LUTSs and reduction of prostate volume with acceptable morbidity and functional outcomes warrant larger studies of TULSA with BPH-specific ablation plans and appropriate controls in men seeking relief from LUTSs associated with BPH. TULSA could potentially be of particular treatment value for BPH patients with large prostate volumes, a desire to preserve ejaculatory function, and those who have suspected or biopsy-proven, concurrent, organ-confined prostate cancer.
Footnotes
Author Disclosure Statement
Drs. Joseph Chin, James Relle, and Hatiboglu were investigators in TULSA-PRO clinical trials. Drs. Chin and Relle are paid consultants and speakers for Profound Medical. W.L. was a paid employee at Profound Medical.
Funding Information
No funding information was provided.
Supplementary Material
Supplementary Table S1
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.