
Abstract
Purpose:
Most of the endourologic procedures along the urinary tract have been widely practiced as outpatient operations, including surgery for benign prostatic hyperplasia (BPH). This systematic review and meta-analysis was conducted to assess safety and feasibility of outpatient surgery for patients suffering from symptomatic BPH candidate for endoscopic disobstruction.
Materials and Methods:
PubMed, Web of Science, Cochrane, and Embase were searched up until March 30, 2020. Methodological index for nonrandomized studies (MINORS) tool was utilized to assess the quality of included studies, and a pooled measure of failure rate (FR) or event rate (ER) estimate was calculated. Further sensitivity analysis, subgroup analysis, and meta-regression were conducted to investigate contribution of moderators to heterogeneity.
Results:
Twenty studies with a total of 1626 patients treated according to outpatient criteria for endoscopic BPH surgery were included. In total, 18 studies reporting data on immediate hospital readmission and/or inability to discharge after endoscopic procedure presented FR estimates ranging from 1.7% to 51.1%. Pooled FR estimate was 7.8% (95% confidence interval [CI]: 5.2–10.3); Heterogeneity: Q = 76.85; degree of freedom = 17, p < 0.001; I 2 = 75.12%. Subgroup analysis according to surgical technique revealed difference among the three approaches with pooled FR of 3% (95% CI: 1–4.9), 7.1% (95% CI: 3.9–10.4), and 11.8% (95% CI: 7–16.7) for transurethral resection of the prostate, Green-light, and holmium laser vaporesection, respectively (p < 0.001). At meta-regression analysis, none of the retrieved covariates was able to significantly influence the cumulative outcomes reported. ER for postoperative complications and early outpatient visit showed a pooled estimate of 18.6% (95% CI: 13.2–23.9) and 7.7% (95% CI: 4.3–11), respectively.
Conclusions:
Our analysis revealed how transurethral procedures for BPH on an outpatient setting are overall reliable and safe. Of note, there were significant outcome differences between groups with regard to type of surgical procedure, perioperative prostate volume, and discharge protocol suggesting the need for further prospective analysis to better elucidate the best strategy in such outpatient conduct.
Introduction
Lower urinary tract symptoms (LUTS) caused by benign prostatic hyperplasia (BPH) can be bothersome and negatively impact on a patient's quality of life. 1 As the prevalence of symptomatic BPH increases with age, the burden on the health care system and society may increase due to the aging population. 2 –4 In recent years, the surgical treatment of BPH has changed significantly both for the use of medical therapy and for the introduction of new technologies such as laser surgery as highlighted by the recent update to the American Urologic Association guidelines. 5 Despite several trials which have demonstrated that medications monotherapy or in combination have decreased the progression of BPH and the need for surgery, endoscopic management of BPH remains one of the most performed surgeries in Urology both in an inpatient and outpatient setting. 6
Due to advancement in technology, many of endourologic procedures developed for BPH have been widely practiced as outpatient operations. 7 This has been, in part, due to the miniaturization of the instruments and new laser energies available, which has allowed for a reduction in the costs related to the procedure and morbidity. Professional Urologic societies suggest the possibility of managing BPH surgery in an outpatient setting; however, there are no specific recommendations 5,8 mainly due to the absence of high-quality evidence about the safety of urologic procedures in ambulatory basis and the right population for outpatient procedures. Currently there is a gap in evidence supporting this approach.
In inpatient setting, scientific societies strongly recommend as a reference treatment transurethral resection of the prostate (TURP) and laser surgery, including holmium laser vaporesection (HoLEP) and 532 nm (“Green-light”) laser vaporesection of the prostate with the potassium-titanyl-phosphate and the lithium triborate. 5,8 All these procedures are effective treatments for moderate-to-severe LUTS secondary to BPH, but they show some differences in terms of safety and required experience. 9,10 These differences raise the question of whether all these procedures can be valid for an outpatient setting. The aim of this systematic review was to assess the safety and feasibility of outpatient surgery in BPH.
Methods
This systematic review and meta-analysis was conducted according to Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. 11 A research question was established based on the Patient-Index Comparator-Outcome-Study design criteria as the following: what is the cumulative failure rate for endoscopic surgical treatment of BPH in the setting of an outpatient recovery? Furthermore, our goal was to compare current evidence within available retrospective and prospective cohort studies. In particular, we determined the pooled failure rate (FR) for outpatient endoscopic surgical BPH procedure in outpatient setting and the prevalence (event rate [ER]) of postoperative complications and emergency room (Er) readmission/outpatient visit within 30–90 days after the surgery.
Evidence acquisition
A systematic literature search was performed on PubMed, Embase, Web of Science, and Cochrane up to March 30, 2020. The following search strategies were used: Ambulatory Surgical Procedures OR outpatient OR day case OR ambulatory AND benign prostatic hyperplasia. All titles and abstracts were assessed to select those focusing on outpatient surgery of patients with bladder outlet obstruction secondary to BPH. The references of the included studies were evaluated for other potential trials. In PubMed the function “related articles” were used to research other articles. The full texts of these studies were evaluated by two authors (S.S. and A.S.).
Selection of the studies and criteria of inclusion
Inclusion criteria
All control and observational studies independent of their size, language, and status of publication, which included patients who had outpatient surgery for BPH and who reported data on the safety of the procedure.
Only studies which reported outcomes in terms of hospital readmission, Er visit, or ambulatory visit.
Randomized and not-randomized comparative studies if they focused on readmission rate after outpatient surgery.
Procedure included: TURP (monopolar, bipolar, plasma resection) or laser surgery, including Thulium laser, Holmium laser, and “Green-light”.
The outpatient surgery had to be preplanned as protocol.
Only studies where outpatient surgery was defined as <12 hours of hospital stay.
Exclusion criteria
The clinical evaluation after hospital discharge was not clearly reported.
Definition of “outpatient” was not clearly reported.
Outcomes from other minimally invasive therapies (e.g., transurethral incision of the prostate, transurethral thermal ablation of the prostate (needle ablation, microwave therapy, and radiofrequency ablative techniques), prostate stent, and prostatic arterial embolization.
Study quality assessment and statistical analysis
To assess the risk of bias (RoB), all included reports were independently reviewed using the “Methodological index for nonrandomized studies” (MINORS), 12 by assessing the potential risk for selection bias, information bias, measurement bias, or confounding bias. All the studies enrolled were rated using a 12-point scale, according to the method proposed by Slim and colleagues. 12 Each item was scored from 0 to 2; 0 indicating that it was not reported in the article evaluated, 1 indicating that it was reported but inadequately, and 2 indicating that it was reported adequately. The mean score for each item was then evaluated to compute a cumulative score and to assess the presence of significant differences among the studies enrolled in the review.
Furthermore, publication bias was tested both by visual assessment of the Deeks' funnel plot and calculation of p-value using the Deeks' asymmetry test. 13 The Trim and Fill method was implemented to explore the possible nature of studies “missed” in the review. 14 We compared each study using ER and 95% confidence intervals (CIs) for both primary and secondary aim. Sensitivity analyses were performed to assess the contribution of each study to the pooled estimate by excluding individual trials one at a time and recalculating the pooled estimates for the remaining studies.
Evaluation for presence of heterogeneity was done using 15,16 : (1) Cochran's Q-test with p < 0.05 signifying heterogeneity; (2) Higgins I 2 test with inconsistency index (I 2 ) = 0%–40%, heterogeneity might not be important; 30%–60%, moderate heterogeneity; 50%–90%, substantial heterogeneity; and 75%–100%, considerable heterogeneity. The pooled ER estimate was calculated using a random effects model. 17 Our results are graphically displayed as forest plots, with pooled ERs indicating overall FR for each study implementing an outpatient recovery regimen for endoscopic BPH treatment and cumulative ER for complications and Er/outpatient visit.
To explore the predefined outcomes of interest, subgroup analysis was performed regarding differences in surgical technique (TURP, HoLEP, Green-light), preoperative transrectal ultrasound (TRUS) prostate volume (PV) (<40cc, >40cc), protocol of discharge (with or without urethral catheter), and preoperative America Society of Anesthesiologist (ASA) score (only I–II vs any score). Meta-regression analyses were performed using available continuous demographic and perioperative variables retrieved among the studies to assess potential source of heterogeneity. ERs were plotted against the following available variables: year of publication, mean age of participants, sample size, intraoperative time (minutes), preoperative TRUS volume (cc), catheterization time (hours), volume of resected tissue (cc), and overall MINORS scores.
The point estimates of the log ERs were obtained and plotted with the area of the circles proportional to the inverse of the squared standard errors of the studies included. Locally weighted scatterplot smoother (LOWESS) function was used to graphically depict the relationship between the different surgical approaches adopted in each single study and the prediction of postdischarge complications and Er/outpatient visit, respectively. Calculations were accomplished using the “metaset” command in Stata version 16.1 (Stata Corporation, College Station, TX) with all tests being two sided and statistical significance set at <0.05.
Results
Search results
The search strategy identified 807 studies, and 10 additional articles were identified through other sources. After removing the duplicates, 687 studies were screened of which 664 were excluded based on title and abstract. For the remaining 23 studies, the full texts were obtained. Three studies were excluded because they did not meet the inclusion criteria (outpatient definition >12 hours). The PRISMA flow diagram is presented in Figure 1. In total 20 records fulfilled the inclusion criteria and were included in the final analysis (Table 1). RoB for the studies included in the qualitative analysis has been reported in accordance with MINORS criteria and is presented in Supplementary Figure S1.
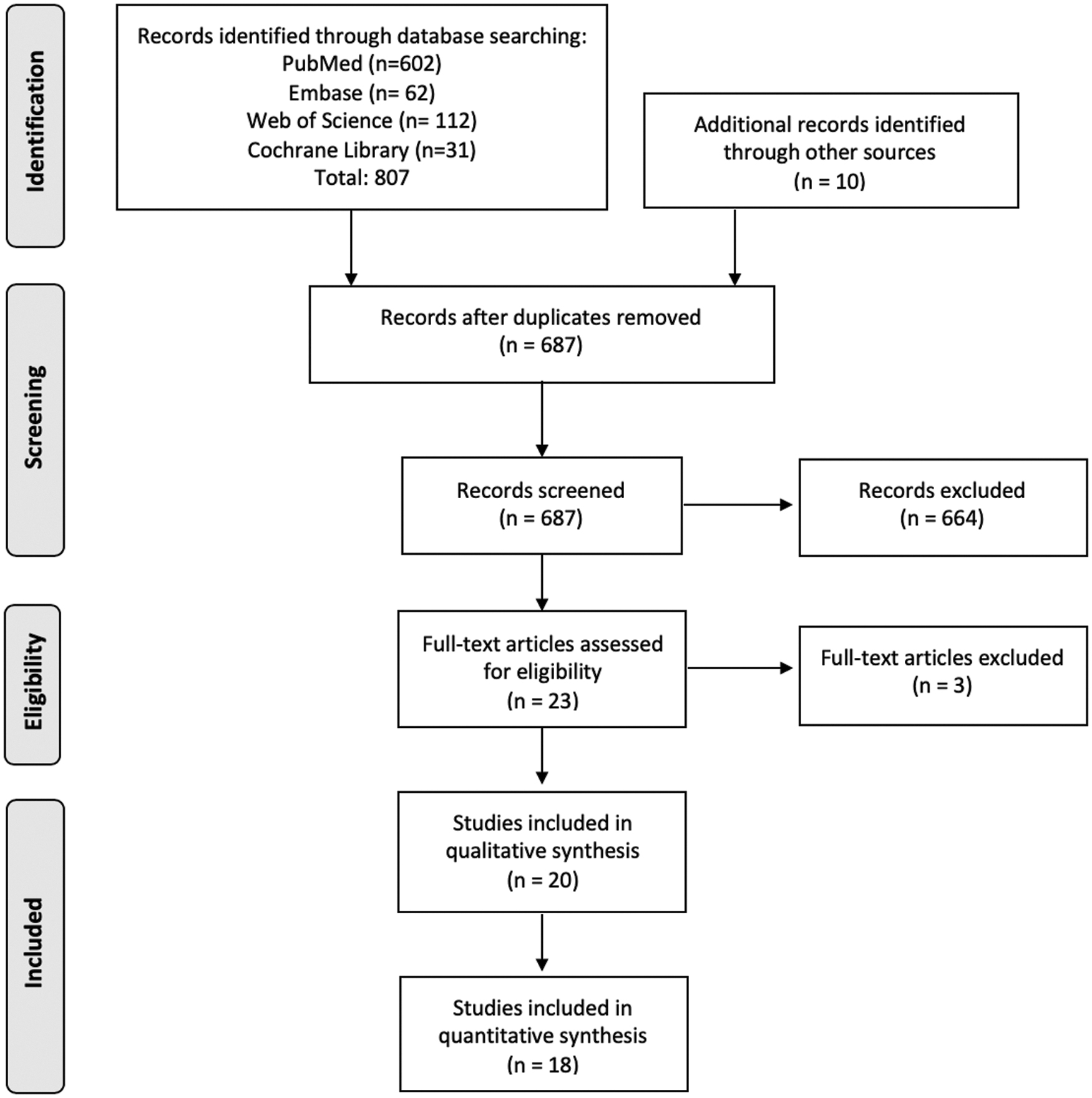
Preferred Reporting Items for Systematic Reviews and Meta-Analyses flow diagram.
Characteristic of the Studies Included in the Systematic Review and Meta-Analysis
Location, design, and characteristics of the study population
Twenty studies that met the inclusion criteria were included in this analysis with a total of 1626 patients that were treated on outpatient basis for BPH. The enrollment of patients was performed between 1990 and 2020. The study design was prospective cohort in 14 studies and retrospective in 6 studies. The location of the studies included were North America (9 studies), Europe (8 studies), Australia (1 study), and India (2 study). Data reported included PV (19 studies), ASA score (18 studies), operative time (18 studies), protocol of discharge (with or without catheter, 16 studies), prostatic tissue resected (10 studies), catheter time (13 studies), and type of anesthesia (8 studies).
Technical surgical aspects and perioperative variables assessed
In terms of type of surgery, four studies were carried out using TURP (one bipolar TURP), nine HoLEP, and six Green-Light (three studies 120 W-HPS, three studies 180 W-KPS). Perioperative outcomes were assessed in terms of outpatient FR (16 studies), Er/outpatient visit (10 studies), and 30–90 days complications-any grade (14 studies).
Cumulative FR of outpatient BPH surgical management
Only two studies 20,36 did not report failure events among the patients included in their analysis and therefore were not considered in the quantitative synthesis. In total, 18 studies 18,19,21 –35,37 reporting data on immediate hospital readmission and/or inability to discharge after the endoscopic procedure presented different FR estimates ranging from 1.7% to 51.1%. Demographic and perioperative characteristics of the 18 studies analyzed are further presented in Table 2. As there was evidence for presence of substantial heterogeneity between the studies: Q = 76.85 (degree of freedom [df] = 17), p < 0.001; I 2 = 75.12%, we reported results according to random-effect model achieving a pooled FR of 7.8% (95% CI: 5.2–10.3) (Fig. 2).

Forest plot reporting cumulative FR among the 18 studies included in the meta-analysis. FR = failure rate.
Demographic and Perioperative Characteristics of Patients with Benign Prostatic Hyperplasia Managed As Outpatient Among the Eighteen Studies Included in the Meta-Analysis
BPH = benign prostatic hyperplasia; HoLAP = holmium laser ablation of the prostate; HoLEP = Holmium Laser Vaporesection; PV = prostate volume; TURP = transurethral resection of the prostate.
According to sensitivity analysis, no single study significantly affected the heterogeneity statistic when removed from the imputation. Inspection of the funnel plot suggested that there was a small-study effect with the smaller studies tending to have higher FR estimates, suggesting the presence of publication bias (Supplementary Fig. S2a). Egger's regression test showed a significant small-study effect (p < 0.001), while the “Trim and Fill” method suggested that six “missing” studies would need to be included to remove asymmetry from the funnel plot (Supplementary Fig. S2b). With these hypothetical studies included, the FR having accounted for publication bias was estimated to be 4.8% (95% CI 1.9–7.7). However, out of these only two of the six imputed studies would have fallen in the area of statistical significance (p < 1%) (Supplementary Fig. S2c). None of the variables implemented in the modeling process resulted significantly able in influencing the pooled FR estimate suggesting absence of potential confounders and confident reliability of our findings for the aim of interest. A summary of the meta-regressions performed together with bubble plots is reported in Supplementary Figure S2d.
Subgroup analysis according to type of surgical technique
In total, five studies 32 –35,37 implementing Green-light, nine articles with HoLEP, 23 –31 and four with TURP 18,19,21,22 were, respectively, reviewed. Test for differences among subgroups revealed the presence of a statistical difference among the three different approaches (Q = 13.32, df = 2, p < 0.001). Furthermore, the subgrouping reveled evidence for heterogeneity imbalances with the studies implementing HoLEP suffering from higher values (I 2 : 80.52%, Q = 56.52, p < 0.001) compared to studies adopting Green-light and TURP, respectively (I 2 : 34.56%, Q = 7.68, p = 0.10 and I 2: 11.18%, Q = 4.65, p = 0.20). Pooled FR was 3% (95% CI: 1–4.9), 7.1% (95% CI: 3.9–10.4), and 11.8% (95% CI: 7–16.7) for TURP, Green-light, and HoLEP, respectively (Fig. 3a). As expected, at funnel plot inspection presence of asymmetry distribution was found only in the HoLEP subgroup as depicted in Supplementary Figure S3a.

Forest plot reporting cumulative FR to
Subgroup analysis according to preoperative TRUS volume (cc)
In total, six studies 21 –23,25,26,32 reporting a preoperative PV <40 cc and eight 24,29 –31,33 –35,37 with >40 cc were, respectively, enrolled. Test for differences among subgroups revealed presence of a statistical difference among small and larger prostates (Q = 4.88, df = 1, p = 0.03). Heterogeneity was mainly in the studies with higher PV (Q = 39.93, I 2 = 75.1%, p < 0.001). Smaller prostates resulted in lower ER with a pooled FR of 4.1% (95% CI: 0.7–7.5) compared to 10.7% (95% CI: 6–15.4) within studies with greater PV (Fig. 3b). Funnel plot according to subgroup stratification is presented in Supplementary Figure S3b.
Subgroup analysis according to urethral catheter discharge protocol
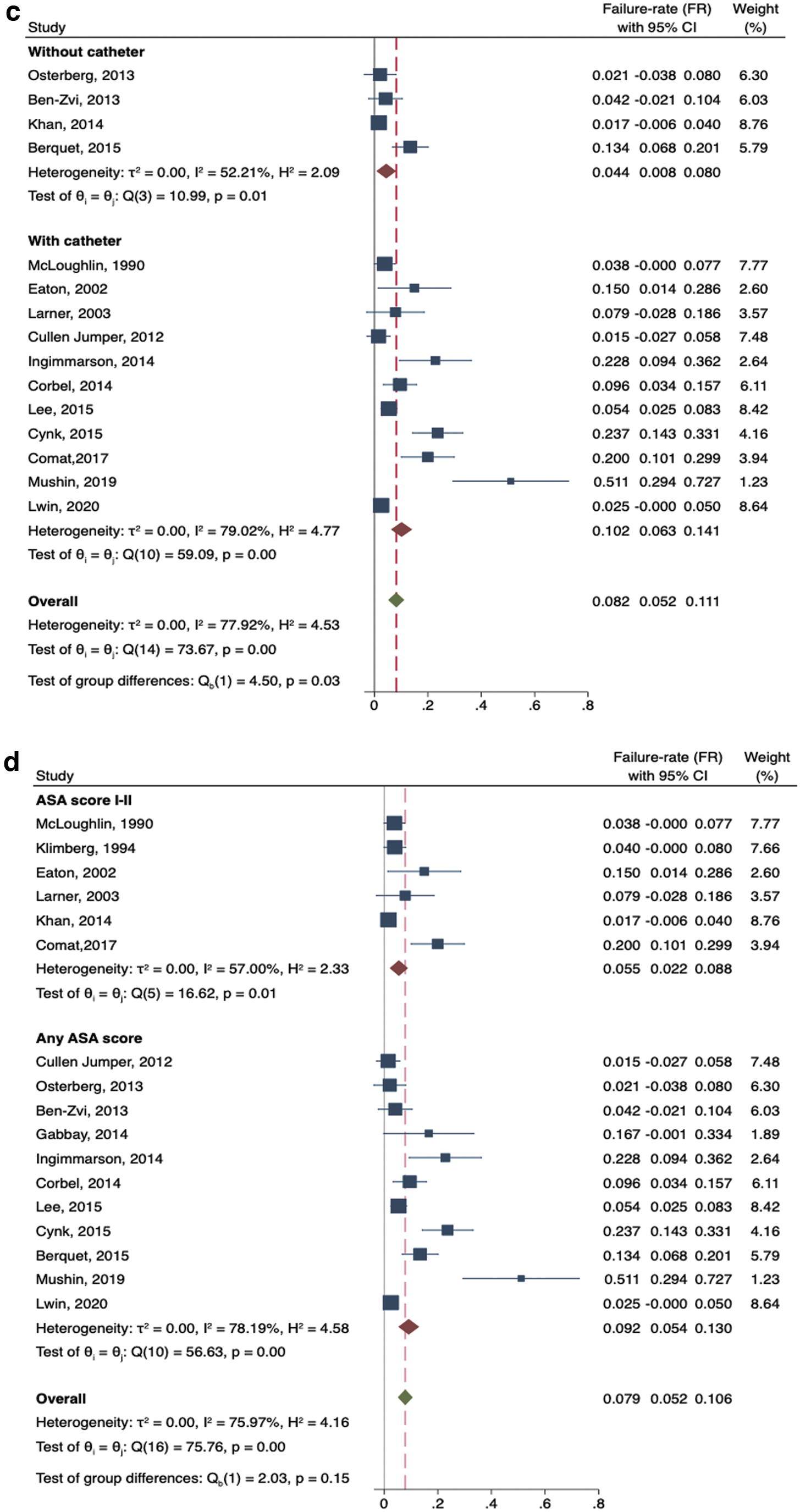
Information regarding urethral catheter at discharge was available on 15 studies. Out of these, 11 18,21,23,25 –31,37 and 4 studies 22,32,33,35 reported discharge with and without catheter, respectively. We found that there was evidence for difference among the two subgroups analyzed (Q = 4.5, df = 1, p = 0.03). Both groups revealed the existence of moderate to substantial (Q = 10.99, I 2 = 52.21%, p = 0.01 and Q = 59.01, I 2 = 79.02%, p < 0.001) as also expressed by funnel plot inspection (Supplementary Fig. S3d). Interestingly, pooled FR was higher in patients discharged with urethral catheter 10.2% (95% CI: 6.3–14.1) compared with those who were catheter free (4.4%, 95% CI: 0.8–8) (Fig. 3d).
Subgroup analysis according to ASA score distribution
Preoperative recorded ASA scores were identified from 17 studies. 18,19,21 –33,35,37 Out of these, 6 studies 18,19,21 –23,29 included only patients with a preoperative score of I or II, while the remaining 11 studies 24 –33,35,37 enrolled patients presenting with any ASA score. Test for homogeneity among the two subgroups demonstrated no significant difference between the adoption of a different ASA score inclusion criterion (Q = 2.03, df = 1, p = 0.15). Both groups presented substantial heterogeneity as shown in Figure 3c and in Supplementary Figure S3c. FR did not significantly differ among the subgroups with a cumulative estimate of 5.5% (95% CI: 2.2–8.8) and 9.2% (95% CI: 5.4–13).
ER for postoperative complications and early outpatient visit
Overall, 6 studies 18,19,22,27 –29 did not report any postoperative complications of any Clavien-Dindo grade, while the remaining 14 experiences accounted for at least one event within a total range of time from 30 to 90 postoperative days. The overall complication estimate ranged from a reported rate of 7.5% in the study of Eaton and Francis, 21 as much as 56.7% in the survey of Gabbay and associates. 24 Since there was evidence for substantial heterogeneity among the studies (Q = 58.26, df = 13, p < 0.001; I 2 = 74.8%), we relied on a random effect model achieving a pooled ER of 18.6% (95% CI: 13.2–23.9) (Fig. 4a).
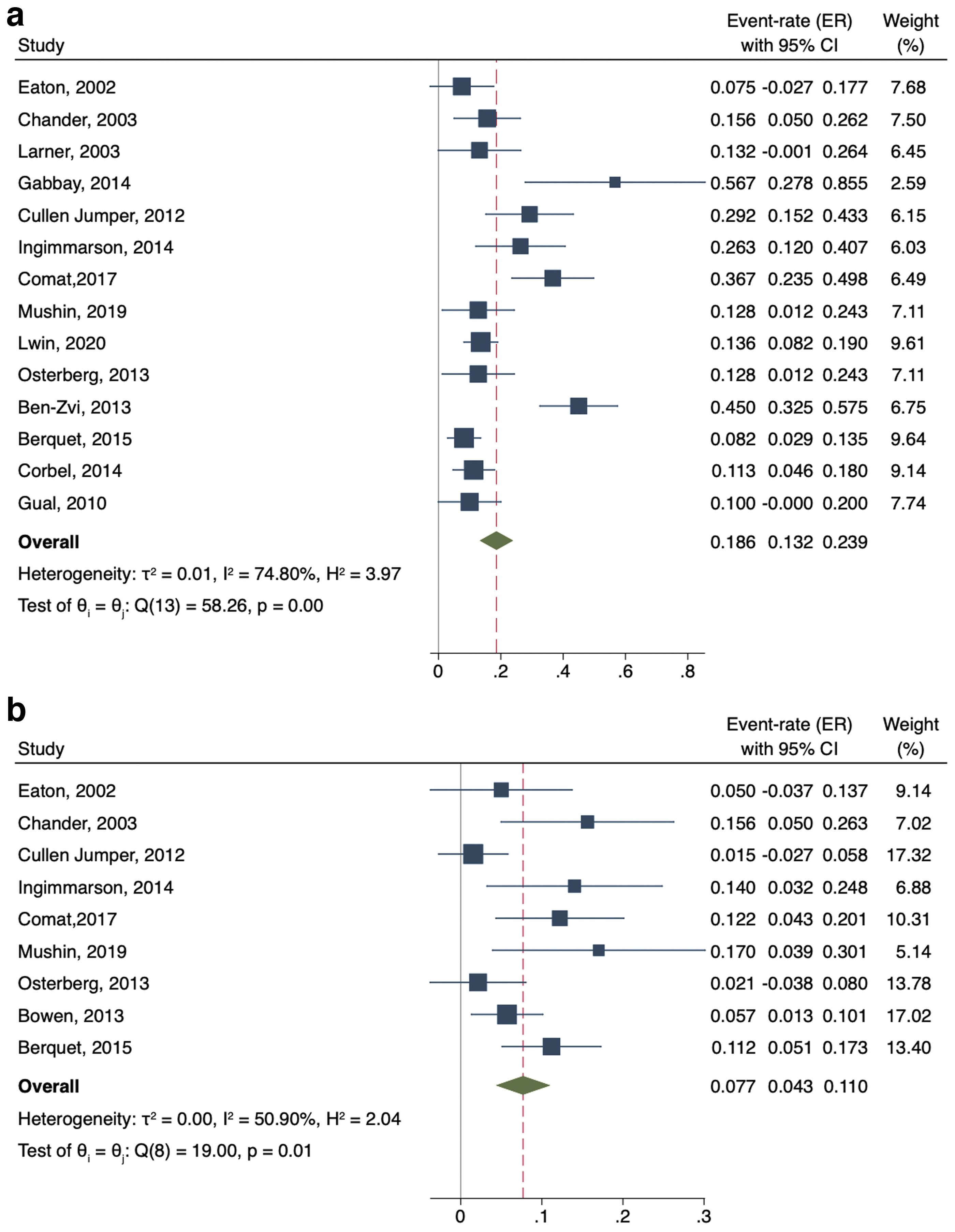
Forest plot reporting pooled ER among the studies assessing
According to sensitivity analysis, no single study significantly affected the heterogeneity statistic when removed from the imputation. Inspection of the funnel plot suggested that there was a small-study effect with one smaller study tending to have higher ER estimate. Egger's regression test showed a significant small-study effect (p = 0.0001), while the “Trim and Fill” method suggested that one single “missing” study would need to be included to remove asymmetry from the funnel plot (Supplementary Fig. S4a). With this hypothetical study included, the FR having accounted for publication bias was estimated to be 17.6% (95% CI 12.2–23.1). Subgroup analysis did not reveal the presence of a difference for complication prevalence among the three surgical techniques implemented (Q = 4.57, df = 2, p = 0.10) nor catheter discharge protocol (Q = 0.25, df = 1, p = 0.62), as well as for both preoperative mean PV and ASA score criteria adopted (Q = 0.65, df = 1, p = 0.42 and Q = 0.04, df = 1, p = 0.84) (Supplementary Fig. S4b).
At meta-regression none of the continuous variables significantly influenced the aim of interest (Supplementary Fig. S5). Regarding Er/outpatient visit following the procedure, 11 studies did not report any event, while the remaining 9 articles 20,21,25,26,29,30,32,34,35 showed an ER ranging from 1.5% in the study of Jumper and colleagues 25 as much as 11.2% in the survey of Berquet and colleagues. 35 The pooled ER using a random-effect model was 7.7% (95% CI: 4.3–11) with moderate heterogeneity among the studies (Q = 19, df = 8, p = 0.01; I 2 = 50.9%) (Fig. 4b). According to sensitivity analysis, no single study significantly affected the heterogeneity statistic when removed from the imputation. Inspection of funnel plot showed the existence of small-study effect with a significant Egger's regression (p = 0.0009). The “Trim and Fill” method suggested that three “missing” studies would need to be included to remove asymmetry from the funnel plot predicting a cumulative ER of 5.9 (95% CI: 2.5–9.2) (Supplementary Fig. S4c).
At subgroup analysis, none of the aforementioned grouping showed significant differences for the event of interest (Supplementary Fig. S4d). Of note, intraoperative time (minutes) and increase in PV (cc) showed a significant positive association with ER of Er/outpatient visit (Coeff: 0.002, standard error [SE]: 0.0009, p = 0.024 and 0.002, SE: 0.0009, 2.17, p = 0.03, respectively) (Supplementary Fig. S6).
Finally, with regard to the surgical technique, despite no significant difference in predicted risk found across all the 20 studies in one approach compared to another for both complication and ER/outpatient visit, we however noticed a rising although slight trend for any complications while a nearly flat predicted distribution of ER/outpatient visit going from the studies using TURP to HoLEP as presented by LOWESS function depicted in Figure 5a and b, respectively.
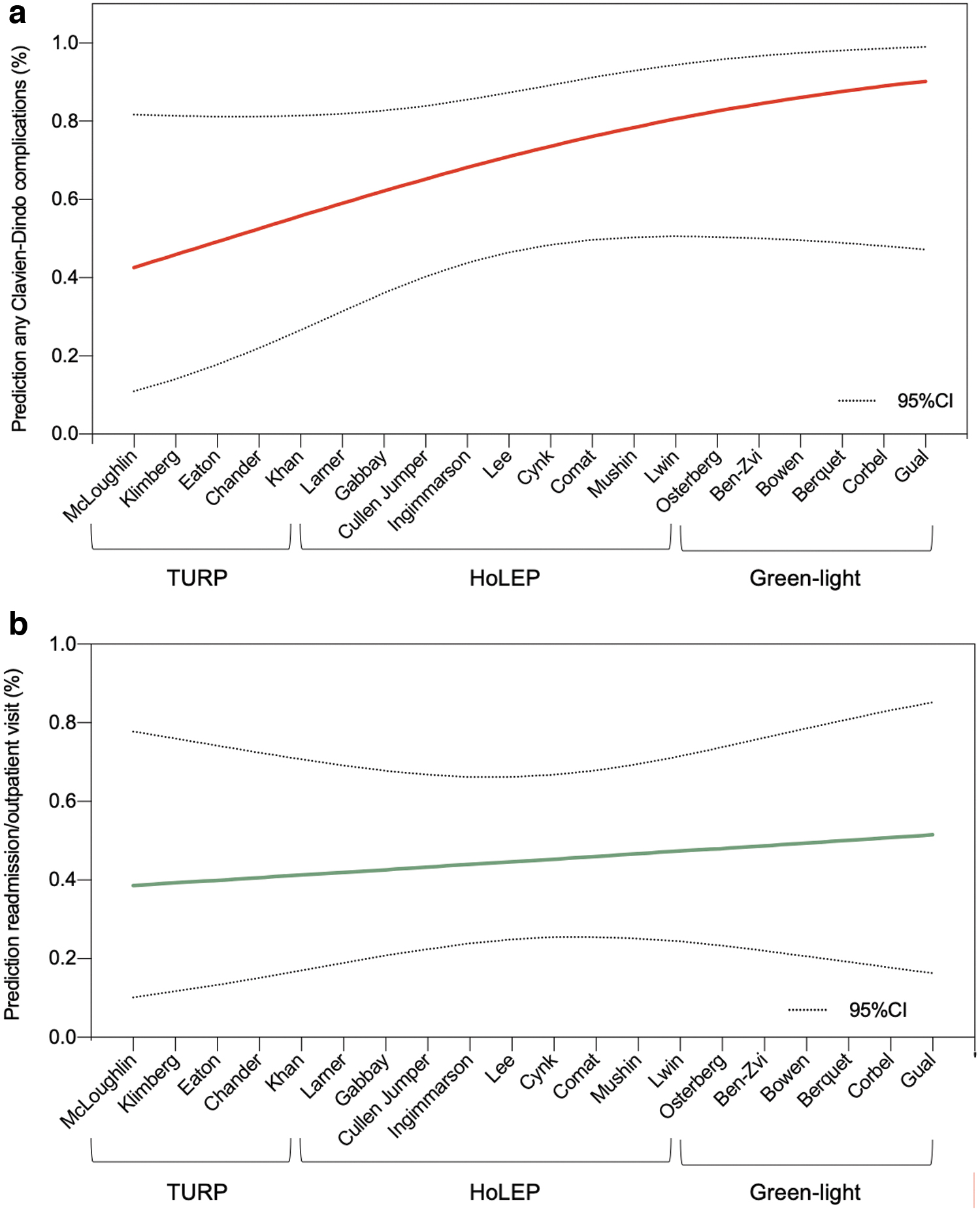
Locally weighted scatter-plot smoother function depicting the relationship between the different surgical approaches adopted with the prediction of postdischarge complications
Discussion
Overall FR of outpatient surgery for BPH
Currently, there are two primary management strategies to treating LUTS secondary to BPH: pharmacologic approach or surgical/endoscopic intervention. Despite the proven efficacy of medical therapy in improving symptoms and delaying intervention, endoscopic management of BPH remains one of the most practiced urologic surgical procedures on both inpatient and outpatient basis. 6 In recent years due to advancement in technology, most of endourologic procedures along the urinary tract have been widely practiced as outpatient operations, including surgery for BPH. The benefits of outpatient surgery are recognized and mainly include cost savings for health care system and reduced morbidity for the patient. 38,39 From a methodological point of view, a procedure to be validated for an outpatient setting should be safe and able to reproduce the same results as in an inpatient setting.
Among urologic surgical procedures, the endoscopic management of ureteral and kidney stones on outpatient basis is well established and widely practiced worldwide. The widespread use of ambulatory surgery for stone disease could be explained by the lower mean age of the patients and standardization of the technique compared to the surgical complexity of BPH surgery. In the field of BPH surgery, technological advances have resulted in many surgical procedures available with various technologies so that the choice of the device is often linked to surgeon experience and preference. These differences may, in part, explain the low quality of evidences exploring the safety of surgical procedures for BPH in the outpatient setting and therefore the absence of specific recommendations from urologic societies.
In this systematic review we analyzed the feasibility and safety of outpatient surgery for BPH. We included only those studies with a clear definition of outpatient (<12 hours of hospital stay) mainly because this definition reflects the health organization of most countries in the world. For these reasons, studies with a definition of outpatient <23 hours, which includes a night of hospitalization, were excluded from the analysis. The meta-analysis showed that outpatient management of BPH is safe with a pooled FR of 7.8% (95% CI: 5.2–10.3). Importantly, none of the variables implemented in the modeling process was able to significantly influence the pooled FR estimate suggesting an absence of potential confounders and confident reliability of our findings for the aim of interest.
Our results are similar to those of inpatient management of BPH using TURP, HoLEP, and Green-light suggesting that from a safety point of view, outpatient surgery achieves the same results as in an inpatient setting. 40,41 Moreover, our results are similar to those reported by Rambachan and colleagues who found in a large series of urologic outpatient surgical procedures a 30-day hospital readmission rate of 4.27% for laser prostatectomy and 4.24% for TURP. 42 The results of this study, in which a definition of outpatient was not reported, indicate that a more stringent definition of outpatient (<12 hours) could result in only a small increase in the rate of readmission (4.2 vs 7.8).
Factors affecting outpatient FR
Subgroup analysis showed a statistical difference among the three different approaches (Q = 13.32, df = 2, p < 0.001) with a pooled FR of 3% (95% CI: 1–4.9), 7.1% (95% CI: 3.9–10.4), and 11.8% (95% CI: 7–16.7) for TURP, Green-light, and HoLEP, respectively (Fig. 3a). The results of HoLEP are not surprising since this procedure is often performed for larger PVs (selection bias), and in our subgroup analysis PV >40 cc was associated to worse results in terms of FR (4.1% for PV <40 cc vs 10.7% for PV >40 cc). Moreover, compared with Green-light and TURP, HoLEP involves a greater quantity of removed tissue and the enucleation procedure is more complex than TURP and Green-light laser with higher risk of intraoperative complications, including prostatic capsule perforation or complications related to morcellation procedure. 43,44 Furthermore, among the studies involving the Holmium laser, two studies 25,26 used an ablation technique (Holmium laser ablation of the prostate [HoLAP]) rather than the enucleation, and we could postulate that such approach may be associated with better safety/tolerability profile than HoLEP. Nevertheless, we did not retrieve any significant difference among this smaller portion of the experiences compared to the others thus not justifying itself the existing heterogeneity with regard to success rate not complication rate within this subgroup.
Another important question is whether the protocol of discharge can affect the rate of hospital readmission. Interestingly in our analysis, pooled FR was higher in patients discharged with urethral catheter 10.2% (95% CI: 6.3–14.1), compared with those who were catheter free (4.4%, 95% CI: 0.8–8) (Fig. 3c). The protocol of discharge without catheter has been evaluated by several studies mainly using Green-light laser, and the safety of this protocol has been explained by the fact that vaporization reduced scar tissue formation during the healing process and sustained creation of a larger, pliable, and relatively smooth prostatic cavity compared with TURP or other technologies. 45 In our subgroup analysis according to protocol of discharge, three of four studies involved Green-light so that the result could be explained by this fact. In the field of outpatient surgery the recent advances in anesthetic techniques have progressively led many surgical procedures to be performed on an outpatient basis extending the types of patients eligible for this surgery: for example, the guidelines of the ASAs and other anesthesiologic societies confirm that stable and controlled ASA III or IV is not an absolute contraindication for outpatient surgery for different surgical procedures. 46 In terms of FR the subgroup analysis according to ASA score showed no significant differences (Q = 2.03, df = 1, p = 0.15) suggesting that surgical procedures for BPH on outpatient basis are safe both in healthy patients and in patients with comorbidities, including patients taking anticoagulants. 26
Complications, unplanned visit, and/or Er visit
As secondary outcomes we analyzed ER for postoperative complications and early outpatient visit or Er visit. The overall complication estimate ranged from a reported rate of 7.5% in the study of Eaton and Francis 21 as much as 56.7% in the survey of Gabbay and associates 24 with a pooled ER of 18.6% (95% CI: 13.2–23.9). Comparing with previous experiences in inpatient setting, the overall rate of complications in our analysis seems to be comparable with other systematic review: Ahyai and coworkers in a meta-analysis of functional outcomes and complications following transurethral procedures reported a rate of perioperative complications from 8.8% for HoLEP to 24.7% for Green-light and a similar trend was observed for late complications (3.5% for bipolar TURP–25.4% for Green-light). 44
In our study the subgroup analysis did not reveal the presence of a difference for complication prevalence among the three surgical techniques implemented (Q = 4.57, df = 2, p = 0.10). However in terms of outpatient visit/ER visit rate without readmission, our analysis showed that the pooled ER using a random-effect model was 7.7% (95% CI: 4.3–11), and with regard to the surgical technique, despite no significant difference in predicted risk of complications or outpatient/ER visits we noticed a slight but interesting rising trend from the studies using TURP to Green-light (Fig. 5a, b). Our analysis showed the existence of consistent variability for HoLEP in terms of reported complications (range 0%–56.7%) however similar to the complication rate observed within inpatient setting. 47,48 Although we acknowledge the presence of two out of seven studies adopting the HoLAP technique rather than HoLEP, such discrepancy was not materially or statistically sufficient to justify the existing heterogeneity, which we observed for complication rates involving Holmium laser to treat BPH.
A further possible explanation for these conflicting results might be that the learning curve of HoLEP has historically been indicated as a major barrier to the widespread of the technique and it could be possible that some of the studies enrolled present differences (unfortunately undetectable between the articles) in terms of surgeon's level of expertise and tertiary vs nontertiary centers. This particular aspect is certainly imitating our possible conclusions with regard to Holmium-based techniques while surely defining the field for future research, which will need to clarify and address this point of concern. To our knowledge, our study represents the first meta-analysis that specifically analyzed safety and feasibility of surgical procedures for BPH in terms of hospital readmission in the specific setting of outpatient surgery.
Our findings suggest that transurethral procedures for BPH are safe with comparable results with inpatient setting. One of the most important advantages of outpatient surgery is represented by the reduction of the costs related to the procedure as demonstrated by several studies. 34,38 However, all these studies do not include in their analysis the costs related to unplanned readmission or to Er/outpatient visit. We believe that this aspect should be taken into consideration for future analysis to have an analysis of the costs well balanced between outpatient and inpatient surgery. There are some limitations in our meta-analysis. First, the number of included studies for TURP was small (four studies), and there is some heterogeneity among the included studies. Nevertheless, it included a relatively large number of patients (n = 1626) and, therefore, represents the available evidence. Second, we were not able to further analyze surgical experience as per variability of the subgroup analysis so that some of included studies could represent a reference center for specific surgical technique or more generally for the surgical management of patient candidate for BPH interventions.
Conclusion
In recent years there is increased attention to ambulatory surgery, which has an advantage in terms of costs for health care system and morbidity for the patient. Our analysis showed that transurethral procedures for BPH in outpatient basis are safe. Subgroup analysis demonstrated significant differences between groups (surgical procedure, PV, protocol of discharge). The degree of heterogeneity between studies limits the strength of our conclusions, but highlights the need for further studies in this field.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this work.
Supplementary Material
Supplementary Figure S1
Supplementary Figure S2
Supplementary Figure S3
Supplementary Figure S4
Supplementary Figure S5
Supplementary Figure S6
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.