
Abstract
Purpose:
Male urethral injury is a common urologic emergency in developing countries. Whether early or late treatment of urethral injuries is often multifactorial and controversial. The goal of this study is to determine whether early realignment can reduce postsurgical complications and evaluate the clinical feasibility of emergency endoscopic urethroplasty using single rigid ureteroscopy in the treatment of bulbar urethral severe injury.
Patients and Methods:
Between September 2013 and March 2019, 15 male adult patients (mean age 35 years; from 21 to 62 years) with severe bulbar urethral injury were enrolled into the current study. The patients mainly presented with dysuria or painful urination (15/15, 100%), urethral bleeding (13/15, 86.7%), and urinary retention (11/15, 73.3%). Six of them had swelling of perineal or scrotal soft tissue, while four had testicular contusion. No pelvic fracture was found in all cases with CT scanning of the pelvic cavity. The bulbar urethral at grade IV was confirmed to be completely ruptured in all cases by endoscopy during operation. The modified endoscopic primary realignment was performed.
Results:
This new urethral repair technique was effectively performed in all patients and none converted to open operation. Mean operation time was 42.3 ± 11.5 minutes (28–52 minutes) and the mean Foley catheter indwelling time was 34.5 ± 6.9 days (28–42 days). During a follow-up of 41.3 ± 22.8 months (12–64 months), mild urethral strictures (grade I) (19.7 ± 9.5 weeks, 10–27 weeks postsurgery) developed in 8 patients (53.3%) and then were all improved 2.1 ± 0.8 months (1.3–2.9 months) after periodic dilatations of the urethra (4–10 times). Erectile dysfunction (ED) occurred in three patients (20%) after surgery, who recovered from mild ED to normal by administration with oral sildenafil (100 mg, three times a week) for 12 weeks. The International Index of Erectile Function-5 (IIEF-5) score was significantly improved after surgery (M ± SD, 25 ± 3) compared with before (16.4 ± 3.5) (p < 0.05). No incontinence and other complications occurred in all cases.
Conclusions:
Early endoscopic realignment via suprapubic puncture cystostomy by single rigid ureteroscopy provides an effective, feasible, and safe procedure for severe bulbar urethral injury.
Introduction
Urethral injuries are uncommon yet potentially devastating, often leading to sequelae such as urethral strictures, erectile dysfunction (ED), and urinary incontinence. 1 These injuries may occur at various segments of the urethra and typically have varying management strategies. Anterior urethral injuries are most often caused by iatrogenic or straddle injuries and occasionally by penetrating injuries or insertion of foreign bodies. The bulbar urethra is the most often injured by blunt trauma, where the bulb is compressed against the pubic symphysis, resulting in urethral disruption. 2 In contrast, posterior urethral injuries are often distraction injuries accompanied by pelvic fracture injuries. 3
Although a urethral injury is not a life-threatening injury, appropriate treatment is necessary to improve patients' quality of life. 4 As such, the European Association of Urology classification system is implemented for blunt urethral injury to guide therapy. 5,6 According to the degree of injury, blunt urethral injury is divided into five grades. Common treatment modalities used to treat urethral injuries include suprapubic catheter placement (SPC) with delayed urethroplasty, early nonendoscopic realignment (EPR), and early endoscopic realignment. 7 However, management strategies for anterior urethral injuries, particularly severe bulbar urethral injury, are controversial.
The goal of management is to realign the urethra while minimizing the risks of subsequent urethral stricture, ED, and incontinence. Many experts adopt delayed urethroplasty (3–6 months) after initial placement of SPC. SPC placement results in decreased comorbidity in the immediate period, however, long-term suprapubic drainage is associated with wound infections, urinary tract infections (UTIs), bladder calculi, discomfort, leakage, and dislodgment. 8,9 As such, early repair is worth considering in select cases.
To date, few reports have focused on emergent endoscopic urethroplasty using rigid urethroscopy for grade IV bulbar urethral injuries. The best method for treatment is still a matter of debate. 10 Thus, we sought to conduct a retrospective review of patients with complete anterior urethral rupture with immediate repair using single rigid ureteroscopy and to assess the postsurgical complications.
Patients and Methods
Patients
From September 2013 to March 2019, 15 male patients with anterior urethral ruptures were included in this study (Table 1). Urethral injury severity was graded as partial or complete based on cystourethroscopy. All patients were hemodynamically stable at the time of intervention and all procedures were conducted by the same two surgeons (Z.J.Z., X.S.W.). Patient inclusion criteria were as follows: (i) complete bulbar urethral rupture (grade IV injury) confirmed during surgery, (ii) primary intervention was emergent endoscopic urethral realignment with rigid ureteroscopy; and (iii) failure of catheterization of patients in the emergency room. Patients were excluded if they had (i) concomitant pelvic bone fracture or any other organ injury with the exception of perineal and scrotal hematomas, and testicular contusion, (ii) if follow-up was less than 12 months, or (iii) if patients had ED before injury.
Clinical Information and Treatment Outcomes in 15 Cases
ED = erectile dysfunction.
The most common cause of urethral rupture was straddle injury from falls during work-related activities, sports, and bicycle accidents (11 patients, 73.3%). Two patients (13.3%) were admitted for iatrogenic injury, including urethral avulsion during urethral dilatation and one patient was admitted due to failure of catheterization for acute retention in another department of our hospital. Two patients (13.3%) were injured in traffic accidents.
Primary symptoms included urethral bleeding (13/15, 86.7%) and acute urinary retention (11/15, 73.3%). Various organ injuries, including scrotal or perineal hematomas (6/15, 40%) and testicular contusion (4/15, 26.7%), occurred concomitantly with urethral injuries. Abdominal examination, digital rectal examination, and assessment of lower extremity mobility were all negative. Pelvic CT was performed to exclude pelvic fracture, and six patients had combined swelling of scrotal and perineal soft tissue, and injury and bleeding of the urethra cavernous body. In four patients, this was combined with testicular contusion. Suprapubic catheterization was not needed for any patient. Three patients (20%) had hypertension, two patients (13.3%) had diabetes mellitus, one patient (6.7%) had prior urethral stricture, one patient (6.7%) had benign prostatic hyperplasia, and two patients (13.3%) had two or more comorbidities. Emergency preoperative examinations for patients consisted of routine blood, hepatic and renal function tests, coagulation function tests, X-ray examinations, electrocardiograms, and pelvic CT.
Surgical procedures
Prophylactic antibiotics were given 30 minutes prior surgery. The patients were placed in the dorsal lithotomy position under combined epidural and spinal anesthesia. A 6F/7.5F rigid ureteroscope was inserted into the urethra. The proximal urethra was visualized using a peristaltic pump to continuously irrigate with saline to maintain clear vision. The disrupted portion of the urethra was located and could not be visualized beyond that. Thus, suprapubic puncture was performed with a 16-gauge coaxial needle tube under ultrasound guidance (BK Ultrasound System, Denmark). A guidewire (0.035 inch) was inserted through the puncture needle channel. A 5 mm skin incision was made adjacent to the needle, which was then removed over the guidewire. Dilatation sheaths were then used sequentially from 10F to 18F to expand the abdominal musculature along the guidewire. The dilatation sheath was withdrawn and a 16F peel-away sheath was inserted along the guidewire into the bladder. A rigid ureteroscope was then inserted into the bladder through the peel-away sheath to examine the bladder, bladder neck, and the posterior urethra. A guidewire was then passed through the site of rupture (Fig. 1A). Once the wire was seen by the operator from the cystoscope, it was grasped with biopsy forceps and pulled out through the external urethral meatus (Fig. 1B). At this point a 20F, three-way silicone catheter was inserted over the guidewire into the bladder. Finally, the peel-away sheath was removed.
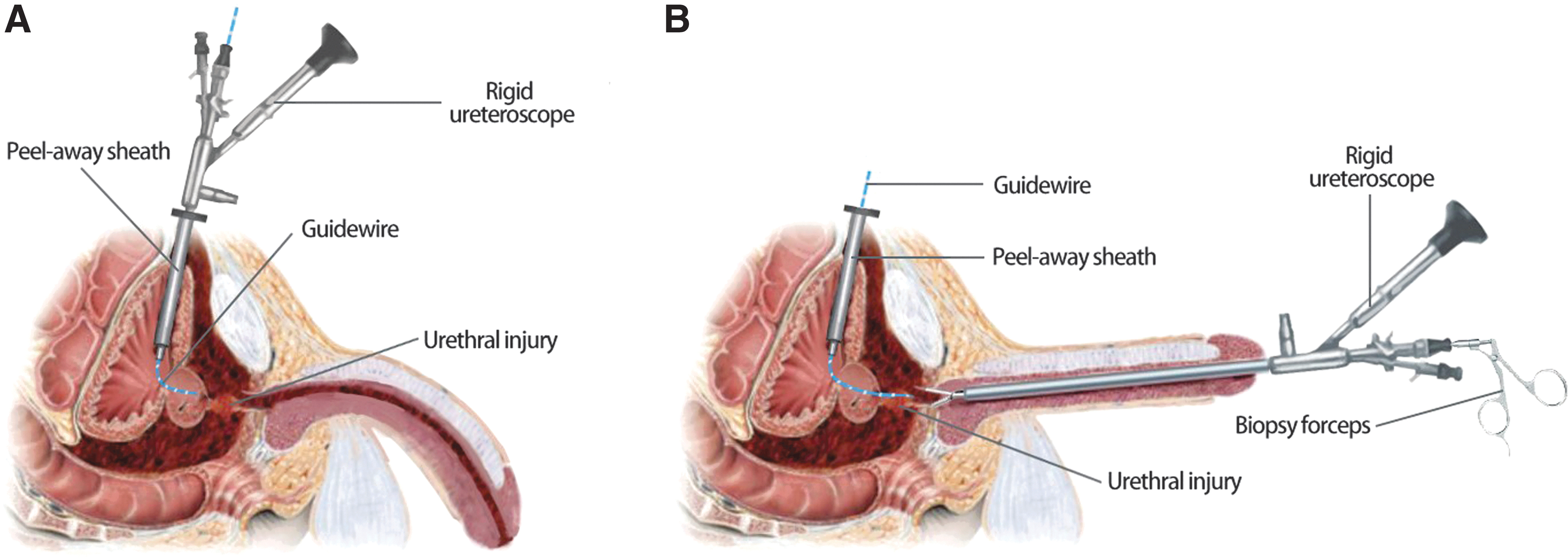
Illustration of the surgical procedures to repair bulbar urethral injury.
Intravenous antibiotics (ceftriaxone sodium) were postoperatively administered for 5 to 7 days. At 4 to 6 weeks after the urethroplasty, pericatheter retrograde urethrogram was performed. If there no urinary extravasation was visualized, the urinary catheter was removed. All patients passed a trial of void after catheter removal.
Postoperative complications such as urethral stricture, urinary incontinence, and ED were examined in all patients at 3, 6, 9, and 12 months. Urethrography (Fig. 2), cystourethroscopy, and urine flow rate (Table 1) were performed for the urethral stricture. The stricture was considered if peak urine flow rate was <15 mL/s. Three grades of urethral stricture were scored by retrograde urethrogram: grade I (mild stricture) the internal diameter of the urethral stricture >2/3 of the normal diameter; grade II (moderate stricture)—the urethral diameter between 2/3 and 1/3 of the normal diameter; and grade III (severe stricture)—the diameter of the urethra <1/3 of the normal diameter. Urinary continence was defined as patient dryness without pads. Erectile function was determined by the simplified International Index of Erectile Function-5 (IIEF-5) during follow-up visits to the clinic. 11,12 An IIEF-5 score ≥22 was considered normal, 12 to 21 was mild ED, 8 to 11 was moderate ED, and ≦7 was severe ED.

Urethrography showed no bulbar urethral stricture and urinary extravasation in case 9 after catheter removal (in a 30° oblique position).
Results
Early endoscopic urethroplasty (EER) by using single rigid ureteroscopy for anterior urethral complete rupture was effective in all 15 patients, and neither of the patients required open or delayed urethroplasty for stricture. The mean time to surgery after injury was 4.7 ± 1.3 hours with a range of 3.5 to 6.0 hours. The mean operation time was 42.3 ± 11.5 minutes (28–52 minutes), and the mean indwelling catheter time was 34.5 ± 6.9 days (28–42 days). Normal urethral continuity was maintained and urethrography was normal in seven patients just after catheter removal. Mean maximal flow rate was 28.8 ± 10.2 mL/s (22.5–39.1 mL/s) within 6 months after surgery. Mild urethral strictures at the site of trauma occurred in the remaining eight patients (53.3%), visualized by urethrogram or cystourethroscopy. No other complications such as urothelium obliteration on urethral lumen, urethrocutaneous fistula formation, or urinary incontinence were found in any of the patients during the 12-month follow-up.
Patients were followed for 41.3 ± 22.8 months (12–64 months). Two patients were lost to follow-up 12 months after surgery. Three patients were lost to follow-up 24 months after surgery. Ten patients are still being followed without further complications. During follow-up, eight patients (53.3%) complained of voiding difficulty and maximal flow rate was less than 15 mL/s. The mean time to development of stricture was 19.7 ± 9.5 weeks (10–27 weeks), with most developing within 10 weeks after surgery. The mean stricture length was 1.8 ± 0.5 cm (1.2–2.3 cm) as determined by urethrogram or cystourethroscopy. Eight patients with urethral strictures were grade I and managed by regular urethral dilatation (4–10 times), all improved 2.1 ± 0.8 months (1.3–2.9 months) after dilatation of the urethra. No open urethroplasty was performed, and the results are shown in Table 1. Three patients (20%) reported ED. The mean time between the operation and development of ED was 17.4 ± 5.5 weeks (12–23 weeks). All patients with ED received sildenafil citrate 100 mg orally 1 hour before sexual activity. This treatment was given continuously for 12 weeks. IIEF-5 and side effects were assessed after 12 weeks of treatment. Sildenafil had a success rate of 100%. The IIEF-5 scores after treatment were higher compared with before (25 ± 3 vs 16.4 ± 3.5) (p < 0.05) (Table 3).
Patients' Conditions Before and After Surgery
SD = standard deviation.
Complications of Severe Bulbous Urethral Injury in 15 Cases
IIEF-5 = The International Index of Erectile Function-5.
Discussion
Injury patterns of anterior urethra vary and encompass mainly urethral crush injuries with straddle and iatrogenic injuries. 13 –15 The mainstay objectives for managing anterior urethral injuries are to obtain prompt urinary drainage and reestablish urethral continuity while preventing complications, such as stricture, ED, and incontinence, 16,17 which is different from posterior urethral injury. Timing for surgical intervention is controversial, 18 –20 and depends largely on the patient's condition and surgeon's comfort. If patients' condition allows, immediate surgery may result in fewer complications compared with the delayed or late surgery. 2,21
Patients with bulbar urethral severe injury usually develop hematoma at the site of injury, which could not correctly judge the injury grade. Therefore, retrograde urethrography did not clearly differentiate partial from complete urethral disruption. 22 Thus, we consider that when endoscopic realignment is appropriate for suspected anterior urethral injury, retrograde urethrography is not necessary. The diagnosis of the severity of injury is made more precisely using urethroscopy.
Three methods of urethral reconstructive surgery have been or are currently used in the clinic (Table 4): (i) EPR; (ii) place a suprapubic tube with delayed urethroplasty (STDU); and (iii) early endoscopic realignment (EER). Conventionally, STDU is implemented as a rapid way to drain urine with urethral reconstruction to follow at a later date. Classic reports advocate a primary cystostomy at the time of injury with delayed, perineal approach urethral reconstruction 3 to 6 months after injury. 10 However, its potential disadvantages include the following: (i) the need for suprapubic drainage for a prolonged period as well as inevitable urethral stricture that requires one or more urethroplasties 23 ; (ii) displacement of the tube; (iii) high incidence rate of ED (up to 40%) 20,24 ; and (iv) distal urethral misalignment and nonanatomic location that may complicate reconstruction have also been reported following the “two-step” procedure. 19
Comparison of Three Surgical Methods of Urethral Reconstructive Surgery
The role of immediate urethroplasty in urethral complete rupture aims to reduce long-term morbidity, but remains controversial to date. 25 This controversy is based on different treatment options that have been proposed in the early management (<48 hours after trauma). 10 EPR restores the continuity of urethra immediately after traumatic disruption. 26
As endoscopic equipment and techniques have improved, EER for urethral injuries has become more common. Several techniques have been reported for successful EER. 27,28 Some authors realign the urethra with two flexible endoscopes. Two flexible cystoscopies can be done simultaneously through a cystotomy and through the urethra. 23,29 –31 We used single rigid ureteroscopy in the treatment of bulbar urethral severe injury in our study. Furthermore, rigid cystoscopy also can be used in endoscopic urethroplasty. However, a bigger peel-away sheath (≧20F) was needed in suprapubic cystostomy, which means a larger incision is needed. Furthermore, rigid cystoscopy is short and lacks enough flexibility when operated through a suprapubic cystostomy. In our study, we conducted endoscopic urethroplasty by using single rigid ureteroscopy for severe bulbar urethral injury. The aim of such immediate endoscopic realignment is to align the proximal urethra and the distal stump to minimize stricture or defect immediately postinjury. Comparing with delayed urethroplasty, 4 our approach has several advantages as this surgical procedure is (i) effective, safe, and quick; (ii) minimally invasive, avoiding extensive operations in severely injured patients; (iii) able to have spontaneous voiding 34.5 ± 6.9 days (ranging from 28 to 42 days) after surgery, compared with other procedures 25 ; (iv) not required to carry the preoperative long-term urethral catheterization for the delayed surgery, which avoids patients' inconvenience and decreases the possibility of UTI or stone formation; (v) avoids tissue damage such as ED 24 –27 that might be ceased by delayed surgery; (vi) suitable for treatment in smaller hospitals with lack of advanced equipment (such as flexible ureteroscope); and (vii) shorter hospital stay (8.5 days) compared with delayed surgery (35.2 days). 32,33
The success rates of endoscopic realignment range from 72% to 100%. 4,28 Three patients in this study had urinary retention, which can easily be treated with suprapubic aspiration or catheterization. This technique allowed for shorter operative duration (28–52 minutes) and no subsequent UTIs.
Development of postrealignment urethral stricture is a major complication of urethroplasty. EER restores in the immediate postinjury period, however, the injured urethra is replaced by scar tissue leading to stricture formation. Long-term success of urethral realignment is defined as no incidence of subsequent urethral stricture. High rates of urethral stricture (range 14%–100%) have been reported in patients who underwent primary open realignment. 12,34 Studies have demonstrated stricture rates ranging from 17.4% 29 to 100% 35 for endoscopic realignment (Table 5). In our study, 7 of 15 patients (46.7%) required no further treatment after initial endoscopic realignment and the stricture rate was 53.3%. This can be compared with other studies seen in Table 5, all of which implemented flexible scopes. This table demonstrates similar stricture rates between the use of flexible cystoscope and semirigid ureteroscope. The incidence of stricture in our series was relatively high, which is likely due to severe urethral injury (grade IV) in most cases.
The Outcomes of Endoscopic Urethroplasty in the Literatures
NR = not reported; UI = urinary incontinence.
For patients with urethral strictures postoperatively, grade I strictures were treated by urethral dilation or self-catheterization usually, grade II strictures were treated by direct visual internal urethrotomy (DVIU) or urethral dilation, and grade III strictures were managed by DVIU or stenosectomy and primary anastomotic urethroplasty. 36,37
Many surgeons do not support open realignment as it has been hypothesized that this might impair the neurovascular bundles and increase rates of incontinence. 2,10,13 In our study, no incontinence was found, which may be because we avoided surgery near the neurovascular bundles. In addition, increasing evidence has revealed that incontinence after STDU and EER did not differ and that injury severity may account for the incidence of incontinence. 19,38
ED was mainly self-reported. In nonrandomized comparative studies and noncomparative studies, ED ranged from 5% to 78.3% (Table 5). In our study, ED was observed in three patients (20%). EER may pose no disadvantage to erectile function and continence due to the lack of additional trauma to periprostatic tissues and cavernous nerves. 39 Furthermore, some researchers also observed that ED did not differ significantly between STDU and EER. 40 –42 Other notable complications include further urethral injury as well as an increased incidence of infection, however, none of these were observed in our study. As such, endoscopic urethroplasty using rigid ureteroscopy has a similar efficacy as flexible cystoscopy in urethral primary realignment of urethral injuries.
Conclusions
Early endoscopic realignment with temporary suprapubic puncture cystostomy by a single rigid ureteroscopy is a fast, effective, and minimal manipulation for several bulbar urethral injuries, having the same treatment effect as used by flexible endoscopes. This technique realigns the urethra without further deteriorating injury and produces functional and more anatomically aligned urethral stricture. We believe that this technique should be considered initially in all patients with urethral complete rupture if their condition allows.
Footnotes
Author Disclosure Statement
None of the contributing authors has any financial or personal relationships with people or organizations that could inappropriately influence work on this article.
Funding Information
No funding information was received.