
Abstract
Introduction:
This study evaluates the introduction of an electronic pH meter to measure the urinary pH in patients with uric acid (UA) urolithiasis and assess patient's perspective.
Materials and Methods:
Patients known with UA urolithiasis were included in this single-center, nonrandomized, prospective feasibility study, IDEAL stage 2a. Their experience with urolithiasis and satisfaction with the method of urinary pH monitoring before inclusion was evaluated. All patients received an electronic pH meter and standardized instructions. After a period of 6–12 weeks their experience and satisfaction with this pH meter and new regimen was assessed. Patient satisfaction was scored on a Likert scale 1–5.
Results:
Eighteen patients were included. Median age was 63 years and median body mass index was 30 kg/m2. The cohort consisted of 67% men and 33% women. In their medical history, 55% had unilateral stones, whereas 45% had bilateral stones. The median estimated glomerular filtration rate was 58 mL/minute/1.73 m2. Eighty-nine percent took medication to alkalize their urine, median 3.5 years. Fifteen patients used paper reagent strips and three used an electronic pH meter to assess urinary pH before this study. Satisfaction with the method of urinary pH measurement at inclusion was reasonable (median score 3; interquartile range [IQR] 1–4). Satisfaction with the new electronic pH meter was good (median score 4; IQR 3–5), as was the overall satisfaction (median score 4; IQR 3–5). The new electronic pH meter was slightly easier to use (median 3.5; IQR 1.75–5), as easy in maintenance (median 3; IQR 2–4), and significantly easier to read (median 5; IQR 4–5). The new electronic pH meter was better (median score 4; IQR 2.75–5) than their previous method.
Conclusion:
The introduction of a standardized approach of urinary pH monitoring for UA urolithiasis patients with an electronic pH meter leads to an easier interpretable outcome and higher patient satisfaction.
Introduction
The prevalence of uric acid (UA) stones within the total spectrum of urinary stones shows a great ethnic and geographic diversity worldwide in published series. 1 –3 The prevalence varies between 4% in Sweden, 16% in Japan, 25% in Germany, and up to 40% in a series in Israel. 1,2 Several studies found that the formation of UA stones is higher in patients with diabetes mellitus type 2, metabolic syndrome, and obesity (body mass index [BMI] ≥30 kg/m2). 1 –5
Furthermore, low urinary volume, low urinary pH, and hyperuricosuria predisposes to UA stone formation. Therefore, metaphylaxis in these patients focuses on the increase of urinary volume by increasing daily fluid intake (decreasing the UA concentration), prevention of hyperuricosuria through xanthine dehydrogenase inhibition (Allopurinol), and dietary advice. In addition to these measures, metaphylaxis with sodium bicarbonate (NaBic), sodium citrate, and/or potassium citrate (KCit) can increase the urinary pH and consequently increases the solubility of UA in urine and prevent new UA stone formation or even dissolve UA stones. 1 –3,6,7 Urinary pH should be targeted between 6.5 and 7.2 for chemolitholysis of UA stones and between 6.2 and 6.8 for prevention. 8
A recent review by Kamphuis and colleagues found that urine alkalization is an established treatment modality for the metaphylaxis of UA urolithiasis despite the lack of evidence from high-quality studies on the methods of alkalization and its treatment efficacy. The studies published on this topic are scarce and contain notable risks of bias that should be kept in mind when interpreting the stated results. Furthermore, guidance on how to go about oral alkalization therapy (medication, dosage, duration, and monitoring) is limited. 3
During alkalization therapy, patients are asked to self-monitor their urine pH. There are different ways to monitor urinary pH. Urine reagent strips are cheap and relatively easy to purchase and handle, however they are inaccurate. 9 –12 On the contrary, electronic pH meters provide an accurate and easily interpretable result but can be hard to come by in an ambulatory setting and require support. 9,11,13 Regular calibration of the meter is necessary. Besides availability, cost can also be a limitation for the use of urinary pH monitoring.
To the best of our knowledge, data on patient's perspective are missing with respect to the aforementioned factors. The goal of this study was to evaluate patient's perspective and feasibility on the introduction of an electronic urinary pH meter and monitoring protocol in patients with recurrent UA stones. We hypothesized that with the introduction of this device and user protocol, measuring urinary pH would be easier for patients, give a clear outcome and increase patients willingness and protocol adherence without additional costs. Possible downside would be time spent with the meter to take a measurement or patients not being able to use the meter.
Materials and Methods
Study design and population
This study was a single-center, nonrandomized, prospective feasibility study, IDEAL stage 2a. 14 Fifty-two patients with recurrent UA urolithiasis were screened for inclusion at our tertiary referral center (Amsterdam UMC, Amsterdam, The Netherlands) between March 2017 and March 2018. Inclusion criteria were age ≥18 years, proven UA stones by X-ray diffraction, recurrent stone events (SE), prior monitoring of urinary pH, and proficiency in Dutch and follow-up at our center. Thirty-two eligible patients were invited to participate and 18 patients agreed to partake in this study.
Ethics
This study was performed according to the ethical standards described in the 1964 Declaration of Helsinki and its later amendments and was approved by the local ethics committee (No. 16.388 8-11-2016). Informed consent was obtained from all participants.
Outcome
The primary outcome of this study was to assess the feasibility of the introduction of an electronic pH meter and patient perspective and compliance on the use of the meter. This was evaluated by assessing patient's experience and satisfaction with structured questionnaires (nonvalidated, created for this study) before and after implementation of a new electronic pH meter.
Data and questionnaire acquisition
Patient characteristics (age, sex, BMI, side affected kidney(s), family history for stones, comorbidities including metabolic conditions predisposing to UA stone formation, estimated glomerular filtration rate [eGFR; the chronic kidney disease epidemiology collaboration equation in mL/min/1.73 m2]) and urolithiasis history were collected. Subsequently, all patients received a first questionnaire (Q1) at inclusion enquiring on their experience with urolithiasis; time since first SE, number of SE, treatment required during SE, and number of spontaneous stone passages. Furthermore, experience with UA stones was addressed; time since diagnosis UA stones, prior medical metaphylaxis (type, dosage, and compliance), time since start of medical metaphylaxis and previous pH monitoring technique (technique, type, frequency, time spend on self-monitoring a week). In addition, we evaluated patient satisfaction on the method of pH monitoring (usefulness and comprehensiveness of the explanation on stone composition and treatment options, on the use of an electronic pH meter, satisfaction with the method of urinary pH monitoring, time spend on monitoring during a week, and overall satisfaction regarding the entire treatment process).
Intervention
Afterward, all patients received an electronic hand-held pH meter (HI99141 pH meter; Hanna® Instruments, Nieuwegein, the Netherlands) (Fig. 1) provided by the hospital, a graphical user manual illustrating the different steps to measure urinary pH, and standardized instructions from a trained lab technician.

The HI99141 pH meter (Hanna® Instruments)
After a period of 6–12 weeks, the participating patients were seen for evaluation and filled-in the second questionnaire (Q2) assessing patient satisfaction; usefulness and comprehensiveness of the explanation on stone composition and treatment options, on the use of the new pH meter, user-friendliness of the new pH meter, and satisfaction with the new standardized method of urinary pH monitoring. In addition, differences with the previous method of urinary pH monitoring (user-friendliness, maintenance, interpretation, and overall satisfaction) and time spend monitoring a week and overall satisfaction regarding the entire treatment process were evaluated.
Statistical analysis
A descriptive analysis was conducted for patient characteristics (age, sex, BMI, side affected, family history for stones, comorbidities including metabolic conditions predisposing to UA stone formation, and eGFR), urolithiasis history characteristics (Q1), and satisfaction with treatment (Q1 and Q2). Patient satisfaction was scored on a Likert scale from 1 (not satisfied at all) to 5 (very satisfied).
SPSS V.26 (IBM Corp., Armonk, NY, USA) was used to perform the statistical analysis. Median and interquartile ranges (IQRs) were reported for continuous variables. Frequencies were reported for categorical variables. Figures and tables were created with Microsoft® Excel for Mac V.2016 (Microsoft Corp., Redmond, WA, USA).
Results
Patient characteristics
Eighteen patients were included in this study, 12 men and 6 women. All included patients had the white ethnicity/race (16 European, 1 North African, and 1 from the Middle East) according to the “Racial and Ethnic Categories and Definitions for NIH Diversity Programs and for Other Reporting Purposes.” 15 An overview of the patient characteristics is given in Table 1.
Patient Characteristics
BMI = body mass index; CKD = chronic kidney disease; eGFR = estimated glomerular filtration rate; IQR = interquartile range.
Uric acid stone history
An overview on the patients' previous stone episode(s) and treatment(s) are given in Table 2.
Uric Acid Stone History
Kcit = potassium citrate; NaBic = sodium bicarbonate; SE = stone events; UA = uric acid.
Eighty-nine percent of our included patients took medication to alkalize their urine before this study (72% used NaBic and 17% used KCit). The median time since these patients started metaphylaxis was 3.5 years (IQR 1–5). The compliance in taking the medication differed widely between patients. Fifty-six percent of patients said they always used their metaphylaxis, 22% said to use their metaphylaxis often, and 11% rarely used their metaphylaxis before this study.
All included patients monitored their urinary pH before the start of this study. Eighty-three percent of patients used reagent paper strips and 17% used an electronic pH meter. Both reagent strips and electronic pH meter were self-bought at a variety of commercial sites (e.g., pharmacy, Internet, and agricultural shops). The majority (94%) spent up to 30 minutes a week monitoring their urinary pH and 6% needed 30–60 minutes for their measurements. On average 44% of patients did less than one measurement a week, 39% measured one to three times a week, and 17% measured their urinary pH more than three times a week.
Questionnaire outcomes: patient perspective on metaphylaxis and method of pH measurement
In general, patients found the explanations on stone type and treatment options clear and useful with both a median score of 5 of 5 on a Likert scale (IQR 4–5), as given in Figure 2. The patients found explanations about the pH measurement comprehensive (median score 4.5; IQR 3–5) and useful (median score 4; IQR 3–5) (Fig. 3). Six patients had difficulties with pH measurement at start of the study, both financially, as well as technically, and scored 1 on the Likert scale. The same six patients were also dissatisfied with the pH measurement method as given in Figure 4. Asked about the method of urinary pH measurement before this study, patients were rather satisfied (median score 3; IQR 1–4) and found it rather easy to use (median score of 3; IQR 1–4). Overall satisfaction with the treatment process was very good (median score 4.5; IQR 4–5).
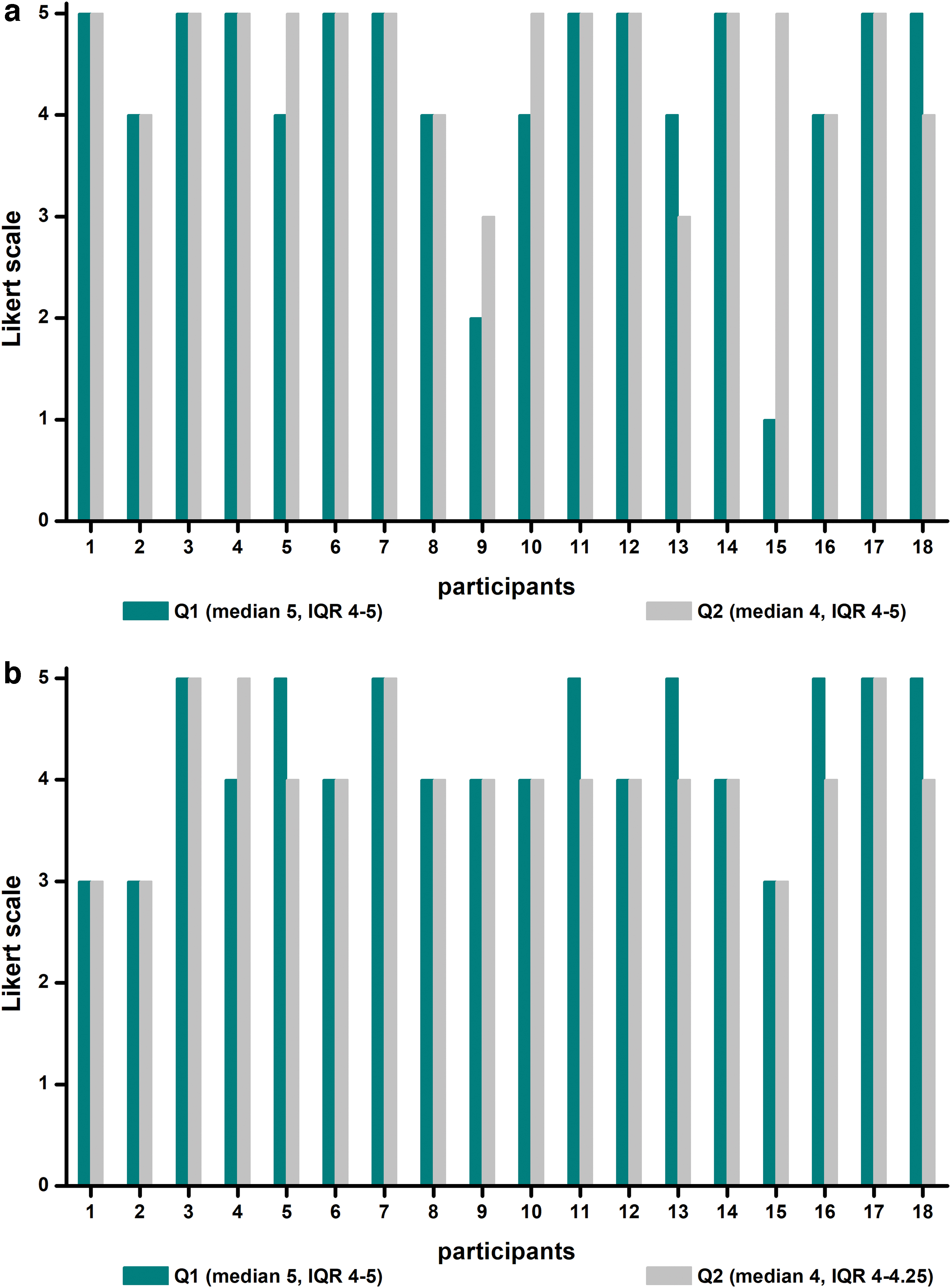
Patient satisfaction with the explanations on stone composition and treatment options (a. Usefulness; b. Comprehensiveness). Color images are available online.
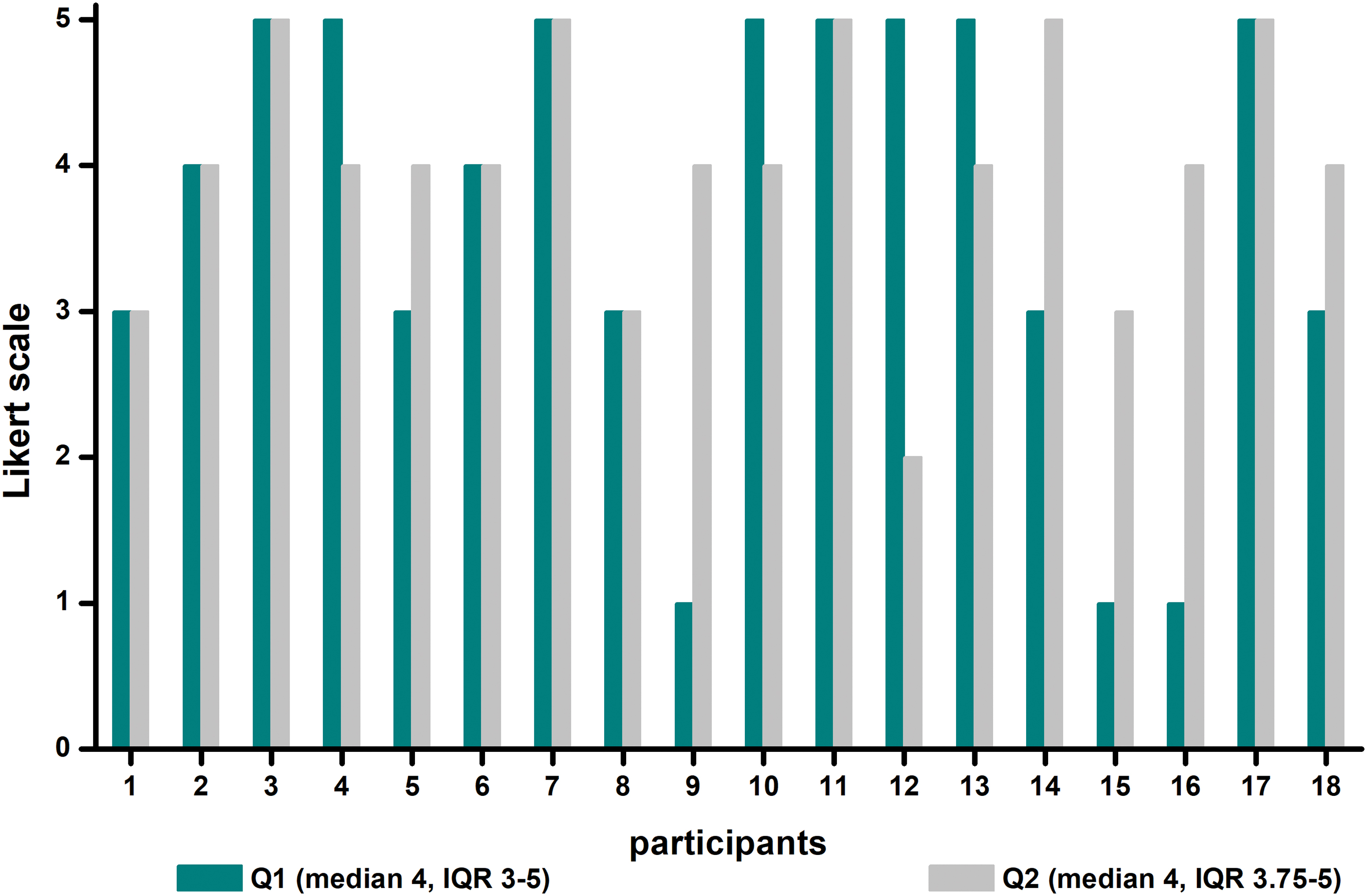
Usefulness of explanations on pH measurement (Q1 = before study inclusion; Q2 = after study inclusion). Q1 = Questionnaire at inclusion; Q2 = Questionnaire at 6–12 weeks after inclusion. Color images are available online.
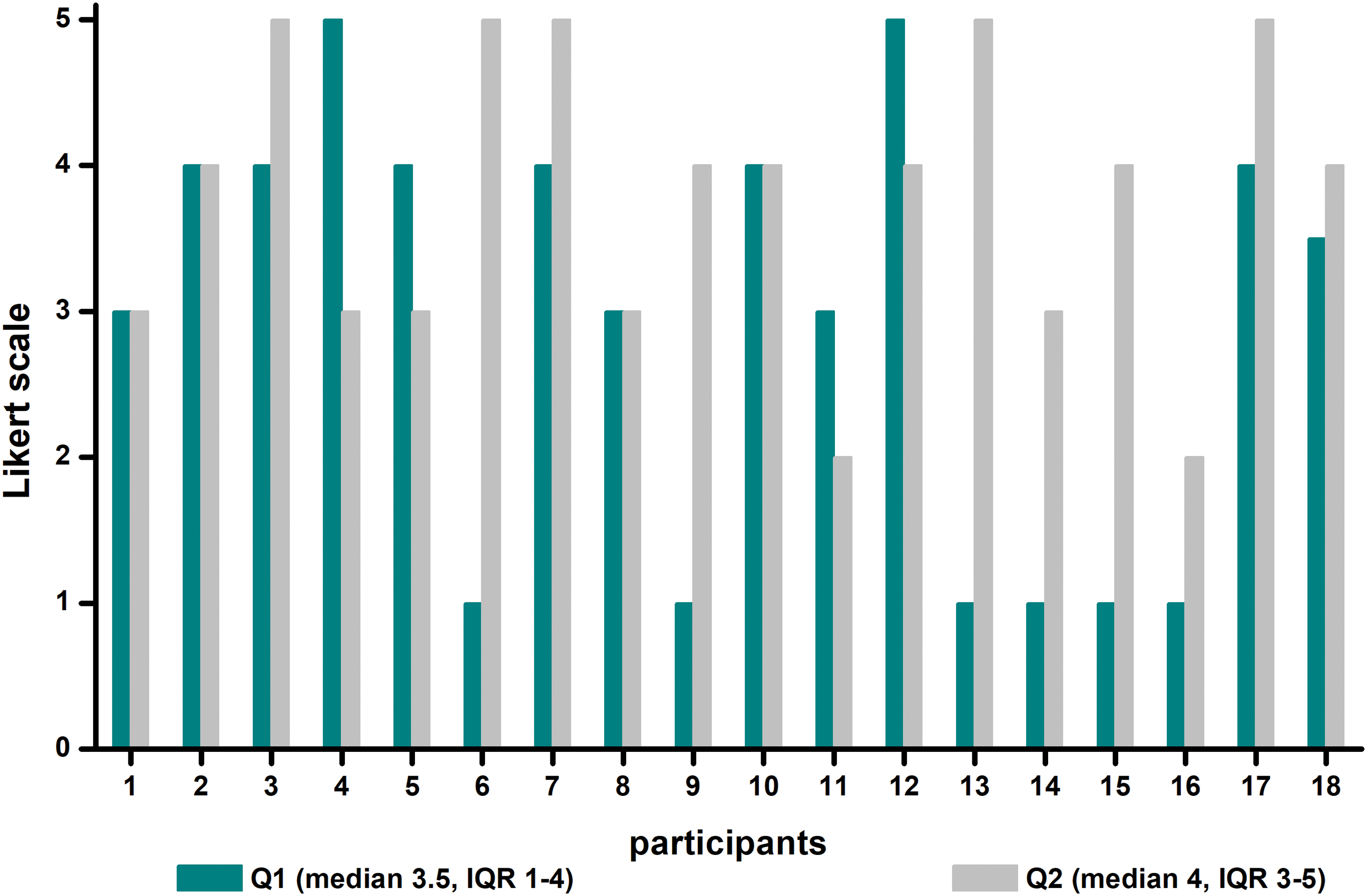
Patient overall satisfaction with pH measurement method (Q1 = before study inclusion; Q2 = after study inclusion). Color images are available online.
After 6–8 weeks using the new electronic pH meter provided, all patients returned the second questionnaire (Q2). The satisfaction with the explanations on stone type and treatment options (Fig. 2) was “clear” (4; IQR 4–4.25) and “useful” (4; IQR 4–5). The median satisfaction with the standardized explanation and graphic user manual as evaluated on Q2 is given in Figure 3 and was high.
We found a median score of 4 (IQR 3.75–5) for usefulness and the same (score 4; IQR 3.75–5) for comprehensiveness. Our study cohort found the new electronic pH meter fairly easy to use with a median score of 3 (IQR 2–4). The overall satisfaction (Figure 4) was good (median score 4; IQR 3–5). The same was true regarding the overall satisfaction with the standardized approach for urinary pH monitoring and overall treatment process in our cohort (median score 4; IQR 3–5). Thirty-three percent of the patients spend 0–30 minutes a week monitoring their urinary pH, whereas 50% spend 30–60 minutes a week on monitoring and 17% spend 60–120 minutes a week measuring urinary pH.
Finally, the included patients were asked to compare this new electronic pH meter with the method of monitoring they used before this study. The new electronic pH meter was slightly easier to use and as easy in maintenance as their previous measurement method (median 3.5; IQR 1.75–5 and median 3; IQR 2–4, respectively). But individually there are exceptions and some patients preferred the paper reagent strips.
Especially the user friendliness in taking paper strips along instead of the meter when travelling from home and the process of calibration on the perspective of maintenance were points of criticism. However, the interpretation of the results was significantly easier according to our patients with a median score of 5 (IQR 4–5). When compared with their previous method of measurement, patients found our study protocol with the new electronic pH meter better (median score 4; IQR 2.75–5) (Fig. 5).
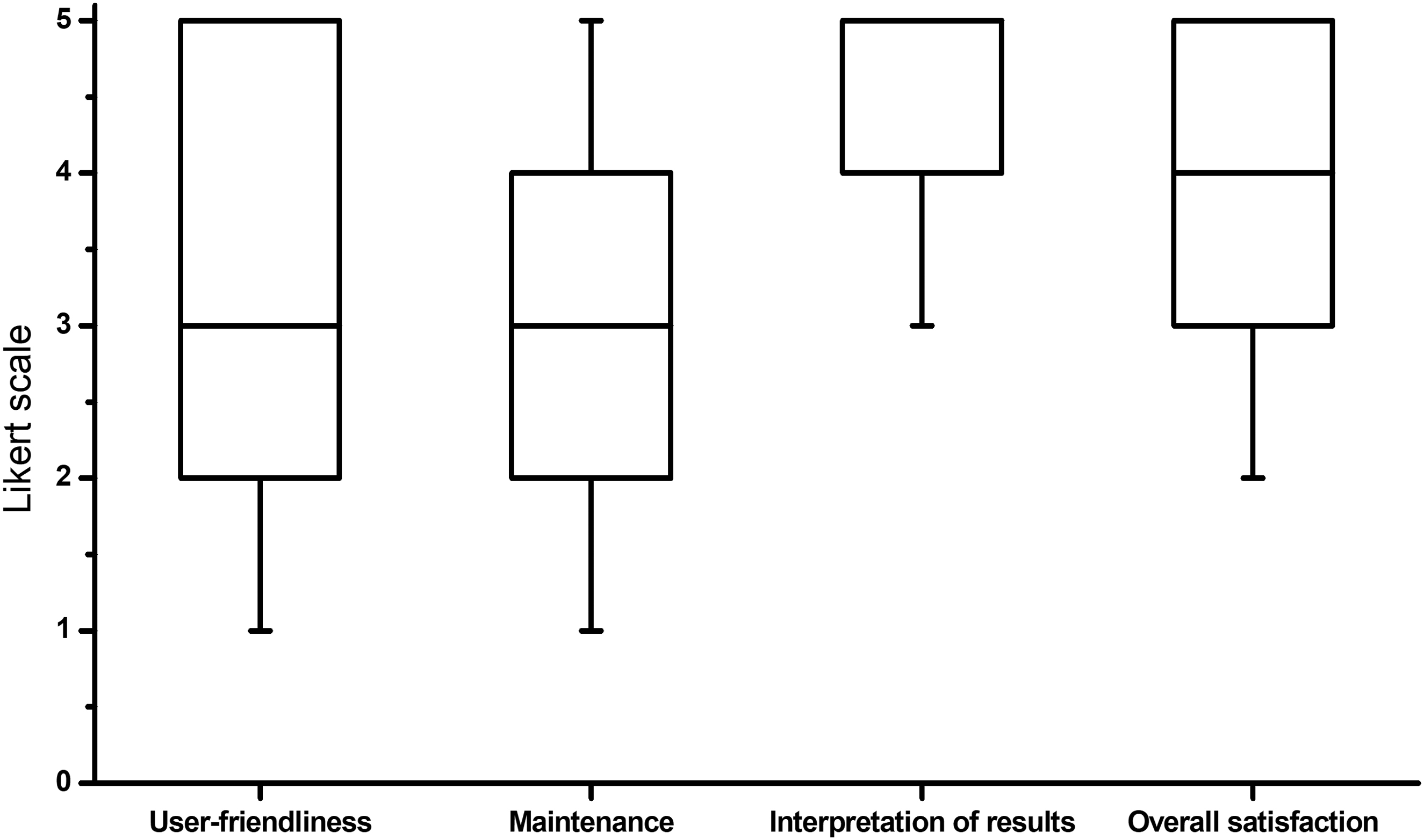
Comparison with previous method of urinary pH monitoring (median and IQR are shown in a boxplot). IQR = interquartile range.
Discussion
Analysis of urinary pH is an important factor in the metaphylaxis and treatment of patients with UA urolithiasis. However, data on the strategies for alkalization of urine in UA urolithiasis patients and on the use of electronic pH meters in patients are scarce. To the best of our knowledge, this study is the first to describe patient's satisfaction in the monitoring of urinary pH with a pH meter.
We evaluated the patient's perspective on the introduction of a standardized approach for electronic urinary pH monitoring with professional clarifications. Participants were open to the new method with the pH meter and had a good overall satisfaction with the standardized approach and overall treatment process in our study-population. More important, the interpretation of the pH was better for all patients.
An electronic pH meter is the gold standard for measuring urinary pH, although these devices are usually not found in an ambulatory setting. 9,13 Most patients use reagent strips because they are cheaper and easier to use and to come by. Electronic pH meters, on the contrary, cost more at first and require some training and regular calibration, making them less convenient for patients measuring their urinary pH at home. 10,13
This study showed that patients experienced the interpretation of the results of their measurements with the provided electronic pH meter remarkably better than their prior method of monitoring. We believe that patients will be more compliant to the therapy if they trust the measurements more and have less doubt in interpretation. Wockenfus and colleagues already showed that urine pH readings from reagent strips are not equivalent with readings from pH meters. This was owing to biased interpretation of the reagent strips. 16 Also for trained nurses, correct reading of pH strips remains challenging. 17
Correct metaphylaxis depends on the accuracy of the method used to measure urinary pH. An inaccurate interpretation can lead to incorrect doses of metaphylaxis, which can then again lead to an ineffective therapy. 9 This is supported by the findings from Kwong and colleagues and Graser and colleagues who compared reagent strips with electronic pH meters and found that one in four measurements with a reagent strip produced a clinically relevant error. 10,13 In contrast to these findings, Graser and colleagues found good intraday and interday precision and small absolute differences (<0.1 pH units) with an electronic pH meter. 13 Ilyas and colleagues described similar findings with a hand-held pH meter from Hanna Instruments with absolute differences of maximum 0.2 pH units. 12
Desai and Assimos stated that an electronic pH meter in an ambulatory setting might lead to a more accurate measurement, better interpretation, and would even be less expensive than reagent strips on the long term. 9 Ilyas and colleagues confirmed the statement that a hand-held electronic pH meter would be cost-effective on the long term. 12
Grases and colleagues did a similar study as ours by introducing an easy to use electronic pH meter with a silicon sensor, which they found to be more robust, of low maintenance, and cheaper than an electronic pH meter. 13 However, they did not look into patient satisfaction. We can imagine that a user-friendly method of measuring urinary pH would lead to a higher compliance and patient satisfaction. This is reflected in our findings, where the overall satisfaction with the new electronic pH meter and the standardized introduction was good and it was valued to be better than the previous method of measuring.
There is a chance of selection bias in our study. Fourteen of 32 patients with UA urolithiasis that were approached did not participate in the study. Main reason for them not to participate was that they were content with current treatment regimen. Possibly these patients are less active stone formers or have been stable on alkalinization therapy. This reflects that the introduction of an electronic pH meter is not necessary in all patients. Despite this, we are convinced that we can improve metaphylaxis in our UA urolithiasis patients with good patient education, as well as by giving them the tools to have high-quality urinary pH measurements to improve the process of alkalization.
In this study, we have shown that the majority of patients can be taught to work with an electronic pH meter and are satisfied with a standardized approach and guidance in this learning process. We believe that this will help patients and clinicians to improve the treatment and metaphylaxis of UA stones.
Study limitations
The main limitation is the limited number of included patients. Furthermore, there was no control group.
Conclusion
Patients with UA urolithiasis can be taught to use an electronic pH meter, which leads to better interpretable measurement results and patient satisfaction.
Footnotes
Authors Contributions
G.M.K.: protocol/project development, data collection or management, data analysis, article writing/editing. J.W. v.H.: protocol/project development, data collection or management, data analysis, article writing/editing. E.C. v.D.L.: protocol/project development, article writing/editing. M.M.E.L.H.: data collection or management, data analysis, article writing/editing. H.P.B.: article writing/editing.
Acknowledgments
The authors thank all the coworkers of the Department of Clinical Chemistry at the Amsterdam UMC, especially Arthur Hoek.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This study has been funded by the Academisch Medisch Centrum Innovation Fund, who funded the purchase of 25 electronic pH meters.