
Abstract
Objectives:
Management of radiation-induced ureteral stricture (RIUS) is complex, requiring chronic drainage or morbid definitive open reconstruction. Herein, we report our multi-institutional comprehensive experience with robotic ureteral reconstruction (RUR) in patients with RIUSs.
Patients and Methods:
In a retrospective review of our multi-institutional RUR database between January 2013 and January 2020, we identified patients with RIUSs. Five major reconstruction techniques were utilized: end-to-end (anastomosing the bladder to the transected ureter) and side-to-side (anastomosing the bladder to an anterior ureterotomy proximal to the stricture without ureteral transection) ureteral reimplantation, buccal or appendiceal mucosa graft ureteroplasty, appendiceal bypass graft, and ileal ureter interposition. When necessary, adjunctive procedures were performed for mobility (i.e., psoas hitch) and improved vascularity (i.e., omental wrap). Outcomes of surgery were determined by the absence of flank pain (clinical success) and absence of obstruction on imaging (radiological success).
Results:
A total of 32 patients with 35 ureteral units underwent RUR with a median stricture length of 2.5 cm (interquartile range [IQR] 2–5.5). End-to-end and side-to-side reimplantation techniques were performed in 21 (60.0%) and 8 (22.9%) RUR cases, respectively, while 4 (11.4%) underwent an appendiceal procedure. One patient (2.9%) required buccal mucosa graft ureteroplasty, while another needed an ileal ureter interposition. The median operative time was 215 minutes (IQR 177–281), estimated blood loss was 100 mL (IQR 50–150), and length of stay was 2 days (IQR 1–3). One patient required repair of a small bowel leak. Another patient died from a major cardiac event and was excluded from follow-up calculations. At a median follow-up of 13 months (IQR 9–22), 30 ureteral units (88.2%) were clinically and radiologically effective.
Conclusion:
RUR can be performed in patients with RIUSs with excellent outcomes. Surgeons must be prepared to perform adjunctive procedures for mobility and improved vascularity due to poor tissue quality. Repeat procedures for RIUSs heighten the risk of necrosis and failure.
Introduction
Ureteral stricture is a serious long-term complication of abdominopelvic radiation therapy. The rate of radiation-induced ureteral stricture (RIUS) has been reported to be 1.2% to 13.5% in patients who have received radiation therapy for pelvic malignancies such as endometrial, cervical, colorectal, or prostate cancer. 1 –5 Such patients may experience significantly altered quality of life due to chronic flank pain, increased risk of urosepsis, need for chronic drainage with a foreign body, and renal unit failure.
Management of RIUS is particularly challenging. Although chronic ureteral stenting or percutaneous nephrostomy (PCN) is an option, this requires periodic exchange under general or local anesthesia and relegates the patient to life-long management. While endoscopic management has a wide range of reported success rates due to heterogeneity of patient factors and surgical techniques, Hafez and Wolf 6 summarized the available literature and report 67% and 78% average overall success rates for balloon dilation and endopyelotomy, respectively. Vast majority of the data are derived from cohorts with few to no RIUSs. Many experts propose that endoscopic management may be appropriate for select patients with benign, short (<2 cm), nonischemic ureteral strictures, but do not recommend it for RIUS. 6 –9 Ureteral reconstruction is the most definitive method for repair, 10 yet such procedures are extremely challenging due to severe postradiation fibrosis and subsequent obliteration of anatomical planes. In a radiated field, the fragile ureteral blood supply has often become compromised and becomes even more tenuous. 11 Microvascular injury to the ureter and periureteral tissue can lead to poor healing and increased fibrosis. 12 Thus, meticulous dissection is essential to minimize disruption of the remaining blood supply. While open reconstructive surgery has traditionally been offered to patients, visualization of tiny blood vessels is limited and these approaches can carry significant morbidity and revision rates. 13,14
The popularity of robotic ureteral reconstruction (RUR) has been on the rise over the past decade. 15 Benefits of RUR include improved visualization and dexterity, quicker recovery due to smaller incisions, access to near-infrared fluorescence (NIRF) imaging modalities, 16 lower estimated blood loss (EBL), and shorter length of stay (LOS). 17 We believe that the advantages of RUR can benefit patients with RIUSs. There is paucity of data regarding treatment of RIUSs and, more specifically, application of the robotic approach. Herein, we present our multi-institutional experience of RUR for management of RIUS.
Patients and Methods
We performed an Institutional Review Board approved retrospective review of our multi-institutional RUR database for all patients with a history of radiation therapy between January 2013 and January 2020. The data reflect surgeries performed by four primary surgeons (M.A., M.S., L.Z., and D.D.E.) at three tertiary referral centers. The indication for inclusion was development of symptomatic ureteral stricture after radiation therapy for any abdominopelvic malignancy. Patients with other potential etiologies such as impacted stones were included if the stricture was developed after radiation therapy. Comprehensive work-up that often included a nuclear medicine renal scan (i.e., MAG-3) and computed tomography (CT), as well as high-quality antegrade and/or retrograde ureterogram by the primary surgeon, was performed before RUR to ideally characterize the strictures. Whenever possible, stents were removed at least 2 to 3 weeks before definitive repair to allow for ureteral rest and better delineate stricture margin. 18 PCN was performed in patients who could not tolerate stent removal. We gathered demographic, clinicopathologic, and outcome data for each patient. Ureteral stricture length was measured radiographically with a fluoroscopic ureterogram and/or during the RUR using an intracorporeal ruler. Postoperative complications (30 days) were reported. Our primary outcomes were clinical and radiographic success rates at the time of last follow-up. Study data were collected and managed using REDCap (Research Electronic Data Capture) tools hosted at each of the institutions listed above.
Surgical techniques
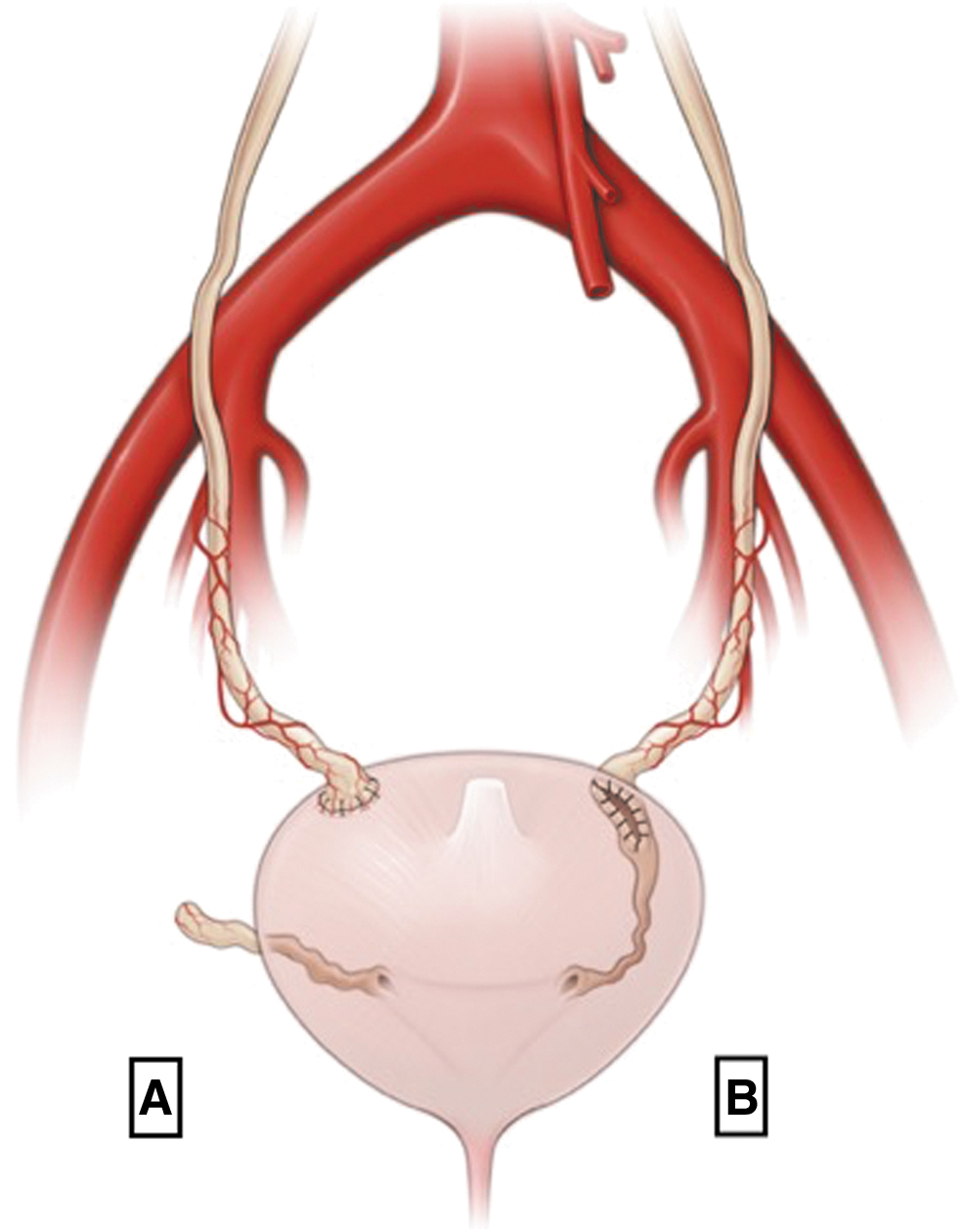
Using the da Vinci Si or Xi surgical systems (Intuitive Surgical, Sunnyvale, CA), patients underwent one of five reconstruction techniques. One case was performed using the novel da Vinci single-port system. The techniques for end-to-end 19 and side-to-side 20 ureteral reimplantation (Fig. 1) have been previously described by our group. Additionally, we have described our experience and techniques for substitution ureteroplasty using the appendix 21 and buccal mucosa graft. 22 Similar to techniques described in literature, 23 ileal interposition as ureteral replacement was performed in select cases. The choice of reconstruction technique was at the discretion and experience of the surgeon.
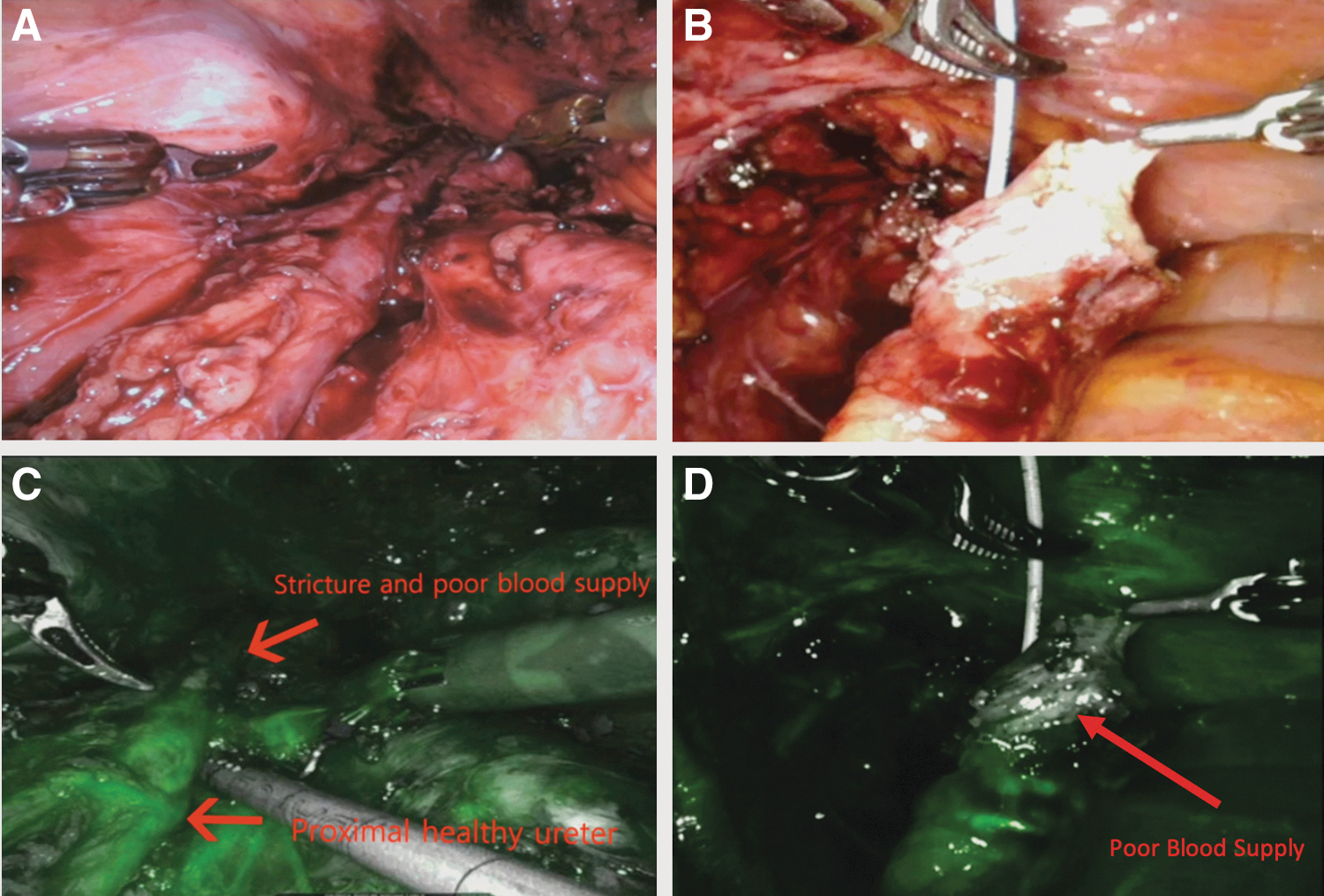
Intraureteral injection of indocyanine green (IU-ICG) with the use of NIRF 16 was used in select cases to help ureteral identification and dissection. In some cases, intravenous injection of indocyanine green (IV-ICG) was administered to ensure adequate perfusion to the anastomosis (Fig. 2) or the appendiceal pedicle. 24 Adjunctive procedures such as a psoas hitch or Boari flap (BF) were undertaken in some cases to reduce tension at the anastomotic site. In select cases, the bladder was hitched to the peritoneum, paravaginal structures, or pelvis instead of the psoas muscle. A 6F Double-J ureteral stent was used for all cases.
Postoperative evaluation
Patients returned to the clinic 4 to 8 weeks postoperatively, depending on surgeon preference and intraoperative factors, for stent removal. In the absence of significant complications, an imaging study such as renal ultrasonography (US), CT, fluoroscopy, or nuclear renal scan was obtained at 3 months postoperatively. Patients who reported pain or had equivocal imaging findings for obstruction were either monitored until resolution or taken back to the operating room for further evaluation. If the work-up revealed a clinically significant obstruction, patients were recommended to undergo revision and reconstruction. Clinical success was defined as the absence of flank pain without a ureteral stent or PCN drain. Radiographic success was defined as lack of obstruction using an imaging study (US, CT, or MAG-3 scan). Imaging studies were obtained 3 to 6 months postoperatively; additional imaging was done if clinically indicated. Descriptive statistics were used to report our data.
Results
A total of 32 patients with 35 ureteral units who underwent RUR met our inclusion criteria, as detailed in Table 1. Our cohort consisted of 17 males (63.1%) with a median age of 65 years (interquartile range [IQR] 55–70). Median patient body mass index was 28.0 (IQR 26.0–32.3). Eighteen (54.5%), 13 (39.4%), and 2 (6.1%) patients had right, left, and bilateral strictures, respectively. One patient, who initially presented with right ureteral stricture and underwent RUR, later developed a left ureteral stricture and ultimately underwent staged repair. This patient was not counted as having bilateral strictures in our calculations as they were asynchronous.
Demographic and Pathologic Variables
IQR = interquartile range.
The median stricture length was 2.5 cm (IQR 2.0–5.5). Majority of strictures (n = 26, 74.3%) were in the distal ureter, with seven (20.0%) extending from distal to mid-ureter and two (5.7%) isolated in the mid-ureter. At the time of RUR, 18 ureteral units were managed with PCNs and 9 with stents. As seen in Table 2, majority of the patients (n = 21; 60.0%) underwent an end-to-end ureteral reimplantation. A side-to-side ureteral reimplantation was performed in eight (22.9%) cases. In select patients, an appendiceal procedure (n = 4; 11.4%), buccal ureteroplasty (n = 1; 2.9%), or an ileal ureter interposition (n = 1; 2.9%) was performed. NIRF was used in select cases by administration of IV-ICG (n = 15, 42.9%) or IU-ICG (n = 4, 11.4%). Adjunct mobility procedures such as psoas hitch (n = 16; 45.7%), BF (n = 5; 14.3%), and peritoneal hitch (n = 2; 5.7) were performed to ensure a tension-free anastomosis. Additionally, adjunct procedures for improved vascularity such as omental wrap were performed in nine (25.7%) patients. The median operative time was 215 minutes (IQR 177–281) with EBL of 100 mL (IQR 50–150). The median LOS was 2 days (IQR 1–3).
Surgical Management and Postoperative Outcomes
BF = Boari flap; EBL = estimated blood loss; ICG = indocyanine green; IU = intraureteral; IV = intravenous; LOS = length of stay; NIRF = near-infrared fluorescence.
Two (6.1%) patients had postoperative complications greater than Clavien-Dindo grade two. One patient who underwent an ileal ureter interposition had an anastomotic bowel leak requiring return to the operating room. The other patient had a myocardial infarction, resulting in sudden cardiac arrest and death within 24 hours of surgery. This patient has been excluded from follow-up and success calculations.
At a median follow-up of 13 months (IQR 9–22), 30 (88.2%) of 34 ureteral units met our clinical and radiographic definitions for success. Of the four patients who failed the index RUR, patient-one, who underwent an end-to-end ureteral reimplantation, had complaints of flank pain without radiographic evidence of obstruction. A ureteral balloon dilatation was performed 25 months after her index surgery, which resolved her pain. Patient-two had undergone an end-to-end ureteral reimplantation with unintentional early stent extraction due to the stent being tethered to the catheter at the time of catheter removal. This patient's reimplantation failed after early stent removal likely due to urinoma and underwent a revision and reimplantation with BF. Her second repair also failed due to necrosis of the BF and ultimately required a urinary diversion. Patient-three underwent a side-to-side ureteral reimplantation with an appendiceal procedure for a proximal ureteral stricture not attributed to radiation and is currently managed with PCN. Patient-four underwent an appendiceal interposition bypass procedure and developed an obstruction resulting in sepsis and is now managed with PCN.
Discussion
Treatment of RIUSs has presented a challenge to surgeons since the 1920s. 25 The difficulty stems from microvascular injury secondary to radiation therapy and the resultant ischemia and fibrosis of the ureter and surrounding tissue. Tenuous blood supply and dense fibrosis make for a hostile surgical field. While difficulty of dissection in such cases is often anecdotal, Iqbal and colleagues 26 objectively measured preoperative parameters to predict difficult pelvic dissection. Pelvic radiation was significantly associated with increased EBL, operative time, LOS, and hospital costs.
The postoperative course of radiation patients is no less challenging. Monn and colleagues 13 reported their 24-year experience with ureteral substitution using the ileum in management of radiation-induced strictures. In a cohort of 23 patients, of whom 15 had distal strictures, they reported significant morbidity associated with open ureteral reconstruction. At a median follow-up length of 47 months, 34.7% of patients had a small bowel obstruction, while 13% developed a fistula or abdominal hernia. One patient required urinary diversion and another patient required dialysis. Toia and colleagues 14 also reported their experience in open reconstruction of RIUSs. Of 18 patients, 6 underwent primary diversion, while others were managed with reimplantation and cystoplasty, BF, or ileal ureter interposition. In total, six patients developed recurrent strictures and three patients remained dependent on a stent/PCN. Given such outcomes, clinicians may shy away from definitive treatment of RIUSs.
Since the advent of robot-assisted surgery, several small series have reported the success of RUR 15 ; however, only one series has reported on patients with RIUSs. 27 This study describes our multi-institutional experience with RUR in 32 patients with 35 RIUSs. Our findings suggest that patients with a history of radiation often require adjunctive procedures to allow for a tension-free anastomosis. More specifically, the use of psoas hitch and/or BF might ensure better surgical outcomes. 28 Although not routinely used for distal strictures, we noted that majority of patients with RIUSs required such procedures, even in those with shorter stricture length. This finding suggests that the degree of periureteral fibrosis may contribute to difficulty in ureteral mobilization. This is consistent with findings of Stolzenburg and colleagues who performed a psoas hitch and BF in all five patients in his series. 27 Yet, one should be cautious; although the bladder blood supply tends to be much more robust than the ureteral blood supply, it is possible that high-dose radiation may compromise bladder blood supply and possibly lead to BF failure, as demonstrated in the revision BF procedure that failed ultimately in our second failed patient. Needless to say, radiated patients demand careful preoperative evaluation, meticulous surgical techniques, and a conservative surgical plan. Additionally, our data show that an omental flap may be safely used to improve vascularity, protect the repair site, and promote a durable repair. 22,29
The microvascular injury caused by radiation highlights the paramount importance of adequate vascular supply to the site of reconstruction; we believe that RUR can achieve excellent outcomes by minimizing dissection and preserving blood supply. Combining the magnified three-dimensional optics of the robotic platform with NIRF has greatly enhanced the robotic surgeon's ability to not only preserve the ureteral microvascular blood supply but also to investigate the tissue, before and after the repair, to understand real-time perfusion during RUR. In ureteral stricture reconstruction, it is imperative for the surgeon to have an arsenal of surgical techniques to reestablish a tension-free, patent, ureteral drainage system.
Our group has been increasingly utilizing side-to-side ureteral reimplantation due to its theoretical advantages of decreased disruption of ureteral blood supply, widely patent anastomosis, and minimal dissection in a densely fibrotic field. Since the ureter is not transected, the posterior plate of the ureter can maintain its blood supply. An anterior ureterotomy can be extended longitudinally to allow for a wide anastomosis. These factors are hypothesized to lower stricture rates. 20 Minimizing dissection in a radiated field lowers the likelihood of iatrogenic injuries to surrounding structures. Another effective strategy in our consortium has been the use of substitution ureteroplasty using buccal mucosa 22 or appendix grafts. 21 Additionally, similar to a side-to-side reimplantation, we have had success with an appendiceal bypass procedure 18 (Fig. 3). This approach minimized ureteral dissection to divert urine proximal to the stricture directly into the bladder, avoiding dissection of the distal ureter altogether.

Ureteral stricture bypass surgery with appendiceal graft. UO, ureteral orifice. Adapted from Asghar and colleagues. 15
The limitations of our study include its retrospective nature. Our follow-up length of 13 months may not be long enough to adequately capture recurrence of stricture, especially in the context of radiated tissue. Even though this is the largest series in the current literature, the study is limited by the relatively small number of patients. Yet, the development of RIUS is rare and it is difficult to generate large case cohorts. Further prospective studies with more patients and longer follow-up time will allow a better understanding of an optimal management strategy for such patients and would establish the long-term durability of RUR of RIUS.
Our study shows that RUR of RIUS is associated with excellent outcomes. With greater than 1-year follow-up, 30 of 34 ureteral units (88.2%) were free of hardware (i.e., stent and PCN) without clinical or radiographic evidence of obstruction. The surgeries were well tolerated with a short LOS. Of the two patients who had postoperative complications, one had underestimated cardiac risk stratification and unfortunately died from a major cardiac event, even though the patient had an uncomplicated and short-duration operation. The second patient had an ileal ureter interposition with a bowel anastomotic leak requiring a return to the operating room for repair. The four failed RURs are currently status post a single ureteral balloon dilation (n = 1), ileal conduit creation (n = 1), or management with PCN (n = 2). Yet, for the majority, RUR in patients with RIUSs has allowed patients to avoid a lifelong need for ureteral stents or PCN and the associated pain, risk of infection, and need for frequent procedures. Such frequent procedures may result in diminished quality of life and increased financial burden on the patient and the health care system.
Conclusion
Our multi-institutional study shows that RUR could be safely performed in patients with RIUSs with excellent outcomes. Experienced robotic surgeons must abide by the principles of reconstructive surgery and be prepared to perform adjunctive procedures for mobility and improved vascularity due to poor tissue quality.
Footnotes
Author Disclosure Statement
Dr. Eun reports personal fees and other fees from Intuitive Surgical, other fees from Melzi corp, and personal fees from Johnson & Johnson, outside the submitted work. Dr. Stifelman reports personal fees from Intuitive Surgical during the conduct of the study, personal fees from Conmed, personal fees from VTI, and personal fees from Ethicon, outside the submitted work. Dr. Zhao reports personal fees from Intuitive Surgical, outside the submitted work. Remaining authors have no disclosures or conflicts of interest.
Funding Information
No funding was received.