
Abstract
Introduction and Objective:
“Clinically insignificant residual fragments” are an independent predictive factor for recurrence of nephrolithiasis. To improve the stone-free rates (SFR), we tested the viability of a novel bioadhesive system for intrarenal embedding and retrieval of residual fragments <1 mm in a kidney model.
Materials and Methods:
All procedures were performed in a standardized setting, including a kidney model (Kidney module right, Samed GmbH, Dresden) in a plastic basin filled with water. We used a Viper URF flexible ureterorenoscope (fURS) (6.6/8F, Richard Wolf, Knittlingen). A mean amount of 138 mg (standard deviation [SD] ±32.2 mg) of sand grains (range, 0.2–0.8 mm) was inserted in renal calices of the kidney model. We assessed the extraction efficacy of fURS using the bioadhesive system. In total, eight different surgeons performed each one trial, respectively. The endoscopic and macroscopic SFR, the level of the surgeons' experience, and the overall time of stone retrieval were evaluated. Additionally, a survey of the participants was conducted, to assess the contentment with this novel system.
Results:
The extraction of the sand grains was only possible using the bioadhesive system, otherwise they were too small sized to grab with a retrieval basket. The total SFR was 84% (SD ±11.7%). The operation time (p = 0.052) and the percentage of extracted sand grains (p = 0.194) were not significantly different between experienced and less experienced surgeons. All participants stated that it was a promising technique, which they could imagine using on a daily basis.
Conclusions:
The bioadhesive system improves the SFR with fragments from 0.2 to 0.8 mm (0% vs 84%). Also, the performance of this operation is not dependent on the surgeon's experience level. This method might improve the SFR in difficult anatomic conditions, that is, lower calices or anomalous kidneys.
Introduction and Objective
Urolithiasis is a relevant medical condition, which affects patients with a lifetime risk of 6% to 12% depending on geography. In the Western World it is—with a prevalence of around 7%—a major subject of urological treatment. 1 Moreover, the incidence and prevalence of kidney stones is increasing globally, mostly due to dietary practices. 2 Regarding treatment options, minimally invasive procedures, such as ureteroscopy (URS) and percutaneous nephrolithotomy, are the gold standard in modern urology. 3 With the Holmium:YAG (yttrium/aluminium/garnet) laser as the preferred flexible intracorporeal lithotrite, different treatment approaches, especially dusting vs fragmenting, are a subject of research. 4
However, residual fragments after endoscopic lithotripsy are a challenging problem, especially because dusting results in even smaller (<1 mm) residuals. If the diameter measures 4 mm or less, the residuals are designated as “clinically insignificant residual fragments” (CIFRs), which generally have a high chance of spontaneous passage with low reintervention rates. 5 Nevertheless, the term is still discussed controversially. Persisting stone residuals in the upper urinary tract may grow and attain clinical relevance again. 6 Up to 26% of patients with residual stones after treatment become symptomatic within 2 years and need intervention. 7,8 Also, patients feel their quality of life is compromised profoundly because of the recurrent operations and treatments. 9,10 Additionally, it causes a significant amount of health care costs. 11 –13 Hence, it is essential for the patients' well-being to secure complete stone clearance. 14 To improve the stone-free rates (SFR), we tested the viability of a novel bioadhesive system for intrarenal embedding and retrieval of residual fragments after endoscopic lithotripsy in a kidney model. Although this method has been used in different trials, 15 –17 it has not been tested to extract particles within the size of stone dust (diameter 0.2–0.8 mm) so far.
Materials and Methods
Experimental setting
All procedures were performed in a standardized setting, including a kidney model (Kidney module right, Samed GmbH, Dresden) in a water-filled plastic basin (Figs. 1 and 2). To access the renal pelvis, a Flexor® ureteral access sheath (14/16F, 35 cm; Cook Medical, Bloomington) was inserted through an opening in the plastic basin. A mean amount of 138 mg (standard deviation [SD] ±32.2 mg) of sand grains (range 0.2–0.8 mm) was inserted in different renal calices of the kidney model. Before using the new bioadhesive, the surgeons tried to extract the sand grains with a standard ureterorenoscopic approach. The extraction efficacy was assessed using conventional retrieval baskets (NCircle® Nitinol Tipless Stone Extractor [Cook Medical] and NGage® Nitinol Stone Extractor [Cook Medical]).

Experimental setup of basin with Kidney module right, Samed GmbH. Color images are available online.

Kidney module right, Samed GmbH, Dresden. Color images are available online.
Embedding technique
In the second run, the sand grains were covered with the polysaccharide-based, two-component bioadhesive system. 16,18 To our knowledge, the mediNiK® gel developed by Purenum GmbH (Bremen, Germany), we used for the trial, is the only one that has been assessed in studies so far. It was solely compared with clotted blood in the study of Schoeb and colleagues. 17 This bioadhesive is a gel product consisting of 100% biopolymers. The hydrogel-forming components consist of prepolymers of marine origin. The main components comply with the Food and Drug Administration (FDA) definition “generally recognized as safe (GRAS)” and can therefore also be used for food.
It was invented and is produced by Purenum GmbH. Component A, comprising cationically crosslinkable polymers, and component B, comprising crosslinkable polymers, which are crosslinking with component A in a physical reaction through divalent ions and forming a gel (Fig. 3). This reaction is reversible by eliminating the divalent ions through for example, EDTA. 18,19

(1) Stones or stone fragments added to cup. (2) Stones were covered with the blue component A (cationically crosslinkable polymers), (3) Yellow component
To apply the components we used a thin catheter (FlexGuard™ laser fiber insertion sheath [LISA Laser Products GmbH, Kaltenburg-Lindau]) with 2.7F outer diameter and 2.1F inner diameter, which was introduced through the working channel of the scope and placed closely to the sand grains in the calices.
First, the liquid component A was poured over the sand grains. The volume depended on the amount of sand grains that needed to be fully covered. For better visualization, component A was dyed blue. In the next step, component B was distributed the same way, but in a predefined 20 mL volume. The complexing agents instantly formed an adhesive gel lump, which contained the sand grains (Fig. 4).
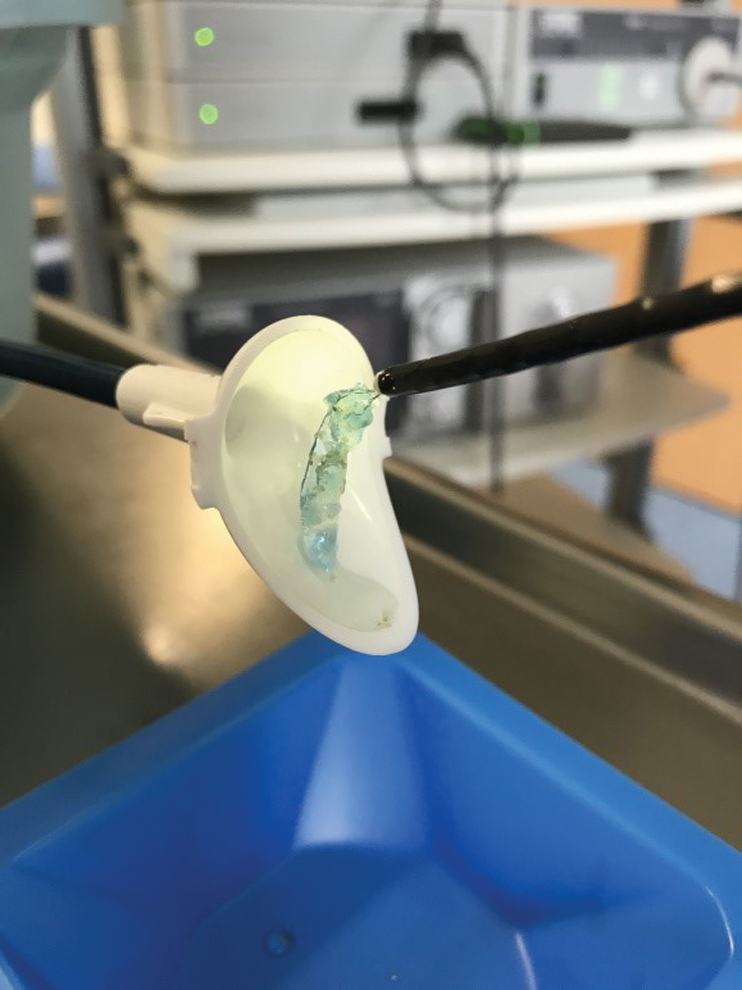
Sand grains covered in bioadhesive system. Color images are available online.
Generally, by using a catheter for application of the gel and an access sheath to collect the stones, the gel rarely is in contact with the ureteroscope. If it still comes into contact with the ureteroscope, it is equally easy to clean it with NaCl, for example, by irrigation.
Extraction of sand grains
For all extractions, a Viper URF flexible endoscope (fURS) (6.6/8F, Richard Wolf, Knittlingen) was used with constant irrigation. Eight different surgeons were included in this study. Three of them had performed more than 250 ureterorenoscopic interventions. One resident performed the operation for the first time. First of all, the surgeons tried to grab the sand grains before applying the gel. Afterward, the residuals were covered with the gel and subsequently, the bioadhesive clots were extracted until the calices appeared endoscopically stone free.
The gel is very soft in the beginning and hardens after 3 to 5 minutes. However, it can always be easily split in smaller pieces by grabbing it with a basket or grasping device. When in pieces, it is safe to get the gel-covered concrements out through the access sheath. If the gel fragment is not too large to fit through an access sheath, it stays stable. It is possible to lengthen it or adjust to surrounding structures like a chewing gum. There is no limitation to visualization during operation because the gel usually does not stick to the tip of the scope. However, if small pieces should get stuck to the endoscope, it would not be complicated to clean the scope with NaCl. Using the same method, residual gel in the kidney can be dissolved with increased irrigation. NaCl softens the gel so that it floats on top of the irrigation due to its lesser density compared with kidney stones. So it can easily be separated from solid components.
Moreover, residual gel fragments are simple to detect due to their blue coloring. There is no difference in visualization of the gel if water or saline is used.
Questionnaire
After completion of the trial, every surgeon had to fill out a questionnaire with 12 topics (Supplementary Table S1). The questions were about the practicability of the procedure and if it is conceivable to include the technique in the daily clinical routine. Each question could be answered with “I completely agree” to “I completely disagree” using the Likert Scale. Points were assigned to each answer to simplify the acquisition of the general opinion regarding the biocompatible adhesive, with five points being the maximum to achieve. The questionnaire was designed specifically for this study. Based on the opinion of the surgeons, it is supposed to help answering if the daily use of this new product is actually supporting the surgery.
Endpoints
The endoscopic and macroscopic SFR were measured after finishing the procedure by extracting the sand grains manually and weighing them after washing the remaining gel material off. The absolute stone extraction rate was defined as the percentage of embedded sand grains the surgeons were able to withdraw. The time from insertion of the scope until the surgeon declared the kidney model as stone free was measured. Also, the experience of the surgeons and amount of ureteral passages were documented. Finally, the total points of the questionnaire was evaluated.
Statistical evaluation
All data were expressed as mean ± SD. For the analysis of the data, the Microsoft Excel 2010 software package (Microsoft Office 2010 for Windows, Version 14.0; Microsoft Corporation, Redmond, WA) was used. Endpoints were evaluated using a t-test for two independent samples. p-Values <0.05 were considered to be significant.
Results
The extraction of the sand grains was only possible while using the bioadhesive system, otherwise they were too small sized to grab with a retrieval basket. In total, a SFR of 84% ± 11.7% was achieved. The mean operating time was 22 ± 7.92 minutes (Table 1). For statistical analysis, the participants were divided in two groups of more and less experienced surgeons (n = 3 vs n = 5). The consultants with experience of over 250 ureterorenoscopic operations needed a mean of 16.67 ± 3.68 minutes to conduct the procedure, compared with 22.6 ± 7.24 minutes for the residents (<250 URS) (p = 0.052). The SFR in the experienced group was 79.8% ± 5.09% vs 86.56% ± 12.61% in the less experienced group (p = 0.194). In both endpoints, no significant difference was measured between the groups.
Results of the Individual Trials
SD = standard deviation.
To retrieve the sand grains, between 3 and 11 passages were needed—which leads to a mean of 6.38 trials. Because of the large “stone burden” that we used for the experiment, each surgeon needed several trials to extract the whole amount of gel-covered sand grains. Failure to successfully grab the gel-covered concrements, was exclusively due to human error for example, missing experience in flexible ureteroscopy.
In the postoperative survey, all surgeons stated that it was a promising technique, which they could imagine using on a daily basis (Table 2). The participants replied with a mean of 4.58 ± 0.27 points to each answer. Regarding the two groups (consultants vs residents), the median was 55.3 ± 3.09 points vs 54.8 ± 3.25 points out of 60 points that could be reached in total. The results of the two groups were not significantly different (p = 0.425).
Point Result of Questionnaire (See Supplementary Table S1)
Discussion
In this study, the practicability and usability of the novel bioadhesive was systematically evaluated for surgeons with a different level of experience. Our key findings were that this new approach ensures a very high SFR. This might minimize the incidence of CIFR and therefore reduce recurrence rates.
The novel bioadhesive material was already tested in three articles and stated as a safe and well practicable technique to extract residual stones. 15 –17 The stone clearance was up to 100% in those settings. However, only very experienced surgeons conducted the operations.
To our knowledge, our setting is the first that included urologists with different levels of endoscopic experience and where particles comparable to stone dust were used. We still achieved a median of 84% stone clearance. In our study, the less-experienced surgeons achieved a higher SFR. This might be due to the fact that the trial was performed during the daily operating schedule in which the more experienced surgeons had less time to be involved in the experiment. However, the SFR was not significantly different between the two groups. This shows that the handling of the gel substance is independent of the users' experience. Even though the statistical insignificance of the amount of extracted sand grains between the two groups could be due to the small number of participants (n = 3 vs n = 5). This certainly represents one of the limitations of this study.
In our trial, the surgeons were able to choose between the two conventional retrieval baskets [NCircle Nitinol Tipless Stone Extractor (Cook Medical) and NGage Nitinol Stone Extractor (Cook Medical)] to collect the sand grains. In the end, only one surgeon of the experienced group used the NCircle Nitinol Tipless Stone Extractor (Cook Medical), the other participants chose the NGage Nitinol Stone Extractor (Cook Medical). Therefore, a statistical evaluation is not useful. There was no standardization in this regard, which presents a study design weakness. Even though the study should represent a daily routine in which the surgeons also might choose between the two grabbing devices based on what they are convinced would work better for the respective kidney stone formations.
Another significant limitation to our experimental setting was that there was no other method to extract residual fragments, for example, blood coagulation, to compare the new bioadhesive material to. However, the study of Schoeb and colleagues already stated the superior features of the new gel in comparison to blood clots due to the better visibility and the faster clotting time. 17 To our knowledge, so far, there are no studies on how laser would affect the gel. However, the gel can be easily separated with baskets. However, we believe that a laser would just separate the gel as well. Matlaga and colleagues pointed out in their review that dusting of kidney stones seems superior to fragmentation considering its shorter operation time, less material consumption (e.g., access sheaths, baskets), and reduced risk of ureteral trauma. 20,21
This method, however, carries a higher risk for CIFRs by producing mainly stone dust, especially when left behind in the lower calix. These small residuals are highly likely to pass spontaneously. However, in around one of five cases, they cause complications, which make hospital admission necessary. 4,22,23 These very small particles left behind after dusting are comparable to the sand grains we used in our experimental trial. The mixed size of concrements is definitely a weakness of this study. However, it is only supposed to be a feasibility study. Further investigations have to be made.
The main point was the better standardization of experiments with sand grains. The texture of sand grains differs from conventional kidney stones. However, for this experiment the difference is from our point of view neglectable. Also, in the sizable amount (in total 1106.6 mg) that was utilized in our study, sand grains are more reliable to acquire in the respective standardized sizes. So even for CIFRs under 0.8 mm equaling stone dust the novel bioadhesive presents a good resolution to achieve maximally high stone clearance. This technique might improve the SFR in difficult anatomic conditions, that is, lower calices or anomalous kidneys.
As expected, the more experienced group of surgeons was able to perform the operation faster than the group of residents. Due to the small group of surgeons, the time difference of around 6 minutes is not statistically significant, even though it is a relevant disparity in a daily clinical routine.
Also, a major limitation to our study is that it was exclusively conducted on a kidney model and not in patients so far. Surely, the missing of complications that would affect the procedure in a clinical routine, for example, bleeding, blurry vision, or ureteral strictures, is an important limiting factor—especially considering the operating time.
Hein and colleagues evaluated the biocompatibility in a porcine study. In this trial, the novel bioadhesive was tested in an in vivo pig model to extract residual fragments after percutaneous nephrolitholapaxia/URS. Two independent and blinded pathologists examined the porcine kidney after the use of mediNiK. They detected no substantial toxic effects to the tissue. 15 Purenum GmbH claims that the bioadhesive gel is stable in urine under laboratory conditions. Due to the biocompatibility of the product, no harm is expected if the gel stays in the collecting system of the kidney. So far, there were no inpatient studies to assess the gel's impact on the urothelium in a human kidney. However, in the study of Schoeb and colleagues, they tested the same type of gel in a porcine kidney. In their reports, they stated that there were no significant adhesions to the tissue. 17 Most likely, it will just dissolve in the urine and pass with it after a certain period of time. Unfortunately, there are no data available to proove these statements. Therefore more studies, especially inpatient trials, need to be conducted. Despite the limitations, this study is representative because it includes consultants as well as residents.
In our study, the overall satisfaction and the practicability of the new method was also evaluated with a questionnaire. In their answers, the surgeons uniformly stated that they consider the bioadhesive material as a promising new technique, which can be easily integrated in the operating routine.
Conclusions
This novel bioadhesive to remove residual fragments from the kidney has enabled the surgeons to retrieve even fragments, which could otherwise not be removed with a basket. Therefore, it significantly improves the SFR with fragments <1 mm (0% vs 84%). It also seems to be a very viable method for surgeons on every level of experience. More tests—clinically studies—are required to further evaluate the bioadhesive-based extraction of stone fragments after lithotripsy.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
Research grant was from Purenum GmbH, Medical Adhesive Innovations, Bremen, Germany.
Supplementary Material
Supplementary Table S1
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.