
Abstract
Objectives:
To report our experience and lessons learned as high-volume center of robotic surgery managing patients with prostate cancer since the beginning of the COVID-19 pandemic in our center.
Materials and Methods:
We described some critical changes in our routine to minimize the COVID infection among patients and health care workers. From March 1 to May 25, 2020, we described our actions and surgical outcomes of patients treated in our center during the pandemic.
Results:
Preventing hospital visits, we implemented some modifications in our office routine in terms of patient appointment, follow-up, and management of nonsurgical candidates. In this period, 147 patients underwent robot-assisted radical prostatectomy (RARP) without intraoperative complications. The median operative time and blood loss were 91 minutes (interquartile range [IQR] = 25) and 50 mL (IQR = 50), respectively. The median hospitalization time was 15.8 hours (IQR = 2.5). None of the patients of our study had COVID in the postoperative follow-up, and only two patients were rescheduled due to a positive rapid COVID test 1 day before surgery. The final pathology described 10 patients (6.8%) Grade Group (GrGp) 1, 34 (23.1%) GrGp 2, 31 (21%) GrGp 3, 16 (10.8%) GrGp 4, 37 (25.3%) GrGp 5, and 19 (13%) with deferred Gleason. Two patients, COVID negative, were readmitted due to infected lymphocele managed with antibiotic and Interventional Radiology drainage.
Conclusion:
Our experience managing patients with prostate cancer during the COVID-19 pandemic showed that changing the office routine, stratifying the patients according to the National Comprehensive Cancer Network (NCCN) risk, and adopting COVID-based criteria to select patients for surgery are necessary actions to maintain the best quality of treatment and minimize the viral infection among our oncological patients. In our routine, the RARP during the COVID pandemic is safe and feasible for patients and health care workers if the necessary precautions described in this article are taken.
Introduction
The first reports of COVID-19 were described in Wuhan, China, in November 2019. Since then, different countries had a pandemic viral spread leading to a global health care collapse. In this scenario, most countries have adopted social distancing with massive population “lockdown” actions, allowing health care systems to focus on the new virus control. Therefore, hospitals worldwide are facing economic issues due to new investments needed in intensive care unit (ICU) and protective equipment, resulting in delays of surgical procedures, medical consultations, and most activities that are not related to the pandemic control. Consequently, oncology patients and physicians are facing new challenges during cancer management in this pandemic scenario.
With this significant health care impact, as a prostate cancer referral center, our dilemma lies in balancing the risks of viral infection with prostate cancer progression and mortality. Also, the challenge is to recognize in the COVID-19 curve the status of infection in our center and adopt the appropriate actions. In this scenario, for how long is it safe delaying the treatment of these patients if we do not know how long this pandemic will last?
Some oncology patients are at a higher risk of a Coronavirus infection, but still require more immediate cancer treatment due to the chances of disease progression. In addition, delaying treatment in patients with high-grade prostate cancer and favorable surgical conditions, while adding androgen deprivation therapy (ADT) for an undetermined period, may increase the risks of side effects, cardiologic events, and compromise the quality of life. 1 Therefore, after a challenging period of planning and adapting health care to this pandemic period, this article aims to report the lessons learned and experience from a high-volume center on managing patients with prostate cancer since the beginning of the COVID-19 pandemic in our center.
Materials and Methods
In this article, we summarized actions that we considered necessary to manage patients with prostate cancer in a robotic surgery referral center during the COVID-19 pandemic. Therefore, we described necessary modifications in our office routine, the patient selection criteria to surgery, and the lessons learned with other centers worldwide. Our main objective was to maintain adequate oncological treatment avoiding unnecessary hospital visits and minimize the viral infection among patients and members of our team.
We also described the intra- and postoperative outcomes of patients who underwent robot-assisted radical prostatectomy (RARP) in our center from March 1 to May 25, 2020. Our institutional review board approval number is 237998-40.
Statistical analyses
We reported our statistical analyses based on established guidelines. 2 Continuous variables were as mean ± standard deviation or median and interquartile range. Categorical variables were reported as frequencies and proportions. The Statistical analyses were performed using Stata 16 (StataCorp. 2019. Stata Statistical Software: Release 16; StataCorp LLC, College Station, TX).
Results
Estimating the COVID-19 surge
Figure 1 estimates the beginning of the COVID infection curve in our center. Point A was our current status before the actions, and point B was the potential “surge” peak. Therefore, being at the beginning of the disease curve, 1 month from the estimated surge, contributed on planning the necessary actions to face the pandemic and treat the oncological patients of our center. This is in contrast to other hospitals, which during the viral surge period, had to add all the efforts and resources on treating infected patients. Therefore, in our experience, we believe that the patient management is different during the different curve periods.

COVID infection curve in our center. Point A is our current status, and point B is the potential “surge” peak.
Office routine and team division
The first step taken was the modification of our office routine and the adoption of a contact precaution. Therefore, all staff members were divided in three different shifts to reduce the number of individuals working in the same period. The staff were also required to use masks and gloves during the entire working period, as were the patients during their consultations. All physical contact and object sharing, such as charts and computers in the common areas, were minimized. Furthermore, before entering the office, all patients and employees had their temperature checked and sanitized their hands with alcohol gel. It was also recommended that every office member who entered the hospital building avoid returning to the clinic on the same day.
The next action was to identify all patients waiting for surgical treatment on our prostate cancer list, and to stratify them into different groups according to the National Comprehensive Cancer Network (NCCN) classification. 3 We identified 585 patients, of which 190 had high or very-high-risk prostate cancer. In sequence, we divided all patients into six teams, of which two were responsible for high- and very-high-risk prostate cancer. Each team had one urologist (responsible for that group), one nurse, and one secretary in direct contact with the office coordinator (S.A) and Urology chief (V.P). Also, the Urology chief was responsible for discussing and guiding all treatment plans according to each case (Fig. 2).
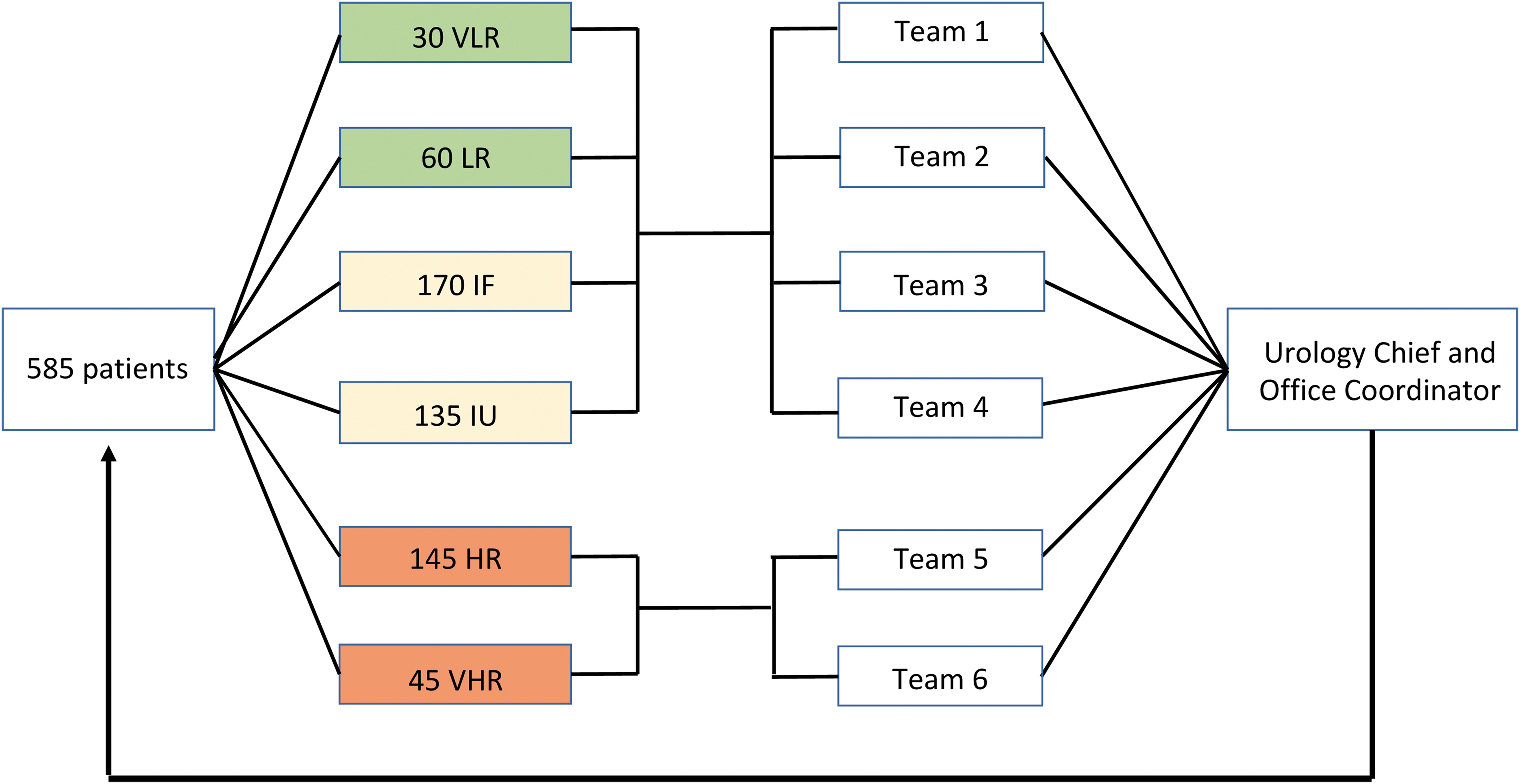
Patients divided according to NCCN risk and team division. HR = high risk; IF = intermediate favorable; IU = intermediate unfavorable; LR = low risk; VHR = very high risk; VLR = very low risk; NCCN = National Comprehensive Cancer Network.
Finally, we adapted our consultation routine to telemedicine encounters and phone calls. The scheduling department contacted all patients to explain our actions against Coronavirus. Then, the group responsible for each patient scheduled appointments as needed. The presence of patients in the clinic was restricted to catheter removals and emergencies.
Selection criteria to surgery
After the division into NCCN groups, the patients were categorized according to a COVID risk stratification based on age, BMI, smoking history, and comorbidities. 4,5 Each variable had a different arbitrary score selected by an internal committee at the beginning of the pandemic after exchanging experiences with other urologic referral centers from different countries and based on the risk stratifications published on that period. 4 –6 Table 1 summarizes all considered parameters with the scores and percentage of votes in the consensus. Patients with scores less than two, from two to four, and higher than 4 were categorized into low, intermediate, and high risk for COVID-19 infection, respectively. Finally, patients in the COVID high-risk group had their surgery deferred due to increased mortality and complication rates.
COVID Risk Table: Points per Disease and Percentage of Votes on Each Disease
BMI = body mass index.
Our criteria to select patients for surgery was based on the combination of NCCN risk and COVID risk groups. Therefore, we selected surgery patients with high or very high NCCN risk who had a COVID score lower than 5 (Fig. 3) while the low and intermediate risks were managed with active surveillance and had the surgery deferred until an available surgical window in the schedule when some high-risk patient was not able to undergo surgery in that day.

Selection criteria to surgery. Patients division and COVID-19 risk.
The high-risk patients had their cases individually reviewed by the Urology chief, who prescribed a temporary anti-ADT with daily Bicalutamide (150 mg). 7 This therapeutic plan will preserve patient isolation, avoiding visits in hospitals and clinics to receive ADT shots. Furthermore, a monthly ADT will minimize the temporary treatment side effects until a surgical window is available for the definitive treatment.
Management of surgical patients
Preoperative routine and patient demographics
The application of SARS-Cov2 testing with real-time reverse transcription/polymerase chain reaction technique 48 hours before surgery is a debatable practice due to the high percentage of false negatives and “turn positive” rates associated with the test. 8 Due to rapid COVID expansion in the United States, most centers do not have the tests available for all patients and employees. However, in our center our COVID screening is based on questionnaires about the patient's routine and exposure in the last 14 days and COVID rapid test 48 hours before surgery. Patients were advised to adopt social distancing and quarantine 2 weeks before surgery. Upon arrival on the day of surgery, the patient is given a surgical mask that will remain in place until the surgical intubation. Only two patients had positive COVID rapid test before surgery. They were canceled and are waiting rescheduling after COVID clearance by Infectious Disease.
The preoperative screening with chest CT is not routine in our center, due to the lack of consensus in the literature, personal protective equipment (PPE) consumption, and increased risk of infections of health care workers and other patients. 9
Table 2 describes the preoperative demographics of patients who underwent RARP during the period of our study and the number of patients operated in March, April, and May 2020. We described the biopsy according to the International Society of Urologic Pathology (ISUP) Grade Groups (GrGps). 10
Patients Preoperative Demographics
AUA = American Urological Association; GrGp = Grade Group; IQR = interquartile range; ISUP = International Society of Urologic Pathology; PSA = prostate-specific antigen; SHIM = sexual health inventory for men.
Intraoperative routine
To maximize the protection of health care professionals during the intraoperative time, all health care staff members performed COVID rapid tests every week, and precautions were taken as if all cases were COVID-19 positive. Therefore, everyone in contact with the patient must wear an N95 mask (Filtering facepiece 2 or 3), operative gowns, gloves, shoe protection, and face shield. During intubation, the entire team stayed out of the room for at least 15 minutes before starting the surgical and robotic draping. 11 The procedure was then performed with our conventional technique by an experienced surgeon to optimize the operative time. 12,13 High-risk patients underwent bilateral pelvic lymphadenectomy. However, we modified the trocar removal step. At the end of the procedure, the trocars were removed after the pneumoperitoneum suction, in a sealed system, to avoid gas spilling through the operative room. Finally, the anesthesia team performed the extubation without any staff member in the room.
Perioperative outcomes and pathology report
During the period of our study, 147 patients underwent RARP. Table 3 describes the intraoperative outcomes and the pathology report. No intraoperative complications were reported. None of the patients was diagnosed with postoperative COVID infection during the follow-up period of this study. We described the final pathology report according to the ISUP GrGps. 10
Intraoperative Parameters and Pathology Report
EBL = estimate blood loss; EPE = extraprostatic extension; PSM, positive surgical margins.
Two patients were readmitted (3 days of hospitalization each) due to infected lymphocele and were treated with antibiotics and Interventional Radiology drainage. Both had negative COVID test at readmission.
Postoperative routine
After surgery, the patient was referred to the postoperative care unit until anesthesia recovery. The patient was then sent to the hospital room with a surgical mask, where he stayed without any companion until discharge the next morning (median time of 16 hours after surgery). 12 Also, during this postoperative period, the patient received orientations about Coronavirus precautions and performed physical therapy in his room. On the morning following surgery, before discharge, our postoperative nurse provided all necessary orientation and educational material regarding the postoperative period to the patient. On the fifth postoperative day, the patient returned to our clinic to remove the catheter. Afterward, the patients were recommended adopting self-isolation for 14 days, and all appointments and consults were performed by phone or telemedicine encounters.
Follow-up and new patients
The first follow-up consultation with PSA result occurred 6 weeks after surgery. During this telemedicine appointment, the patient was advised about postoperative functional and oncological outcomes, as well as COVID-19 prevention. After this meeting, the follow-up was scheduled every 3 months or as needed, according to each case.
New patients referred to our center during the COVID pandemic had the same stratification protocol as aforementioned. The cases and exams were received by our office on email or fax and then discussed with the Urology chief before scheduling a telemedicine appointment. Finally, after the cancer stratification, the appropriate team managed the patients according to the NCCN risk.
Management of high-risk nonsurgical patients
Patients who had high-risk NCCN and high-risk COVID score had their surgery suspended for an undetermined period due to the risk of infection and increased mortality. These patients were also individually reviewed by the Urology chief, who prescribed a trimestral dose of leuprolide acetate (22.5 mg). Finally, patients stratified into very low, low, and intermediate NCCN risks were scheduled to telemedicine follow-up every 3 months.
Discussion
We described our experience in managing patients with prostate cancer during the COVID pandemic. We also adopted some actions learned from the experience of different centers in the United States (NY) and other countries (Italy, Spain, France, India, Germany, England, Belgium, and Russia) during online webinars and urologic meetings. The understanding of the challenges faced by these centers during the pandemic was essential in guiding our actions. Each center and country experienced different stages of the disease and adopted different measures to contain the viral dissemination; therefore, we performed teleconferences with these centers and discussed the best approach for our patients during this global scenario.
Furthermore, we implemented some actions that were particular to the pandemic reality of our center. Despite the COVID reports in Florida, we were in a different disease scenario compared with other states because our hospital still had a low number of COVID cases. In many other states, hospitals spent all resources and health care workers on treating infected patients; while in our center, we had resources, protection equipment, and staff available to perform surgeries. However, knowing that we were weeks behind some centers in terms of disease progression, we were unable to determine the time frame that we would be able to continue to perform surgeries. Therefore, we stratified our patients according to the NCCN risk to detect the best high-risk candidates to undergo radical prostatectomy, while we are still able to operate in our center.
In this scenario, we calculated our actions according to our COVID surge expectations. As we were at the beginning of the curve, we could plan the activities and manage our surgeries, something that would be more challenging during a viral surge. Therefore, we believe that the viral curve evaluation is essential to adopt the necessary actions according to different pandemic stages (beginning, surge, and decline).
In our opinion and experience, if adequate PPE is available for the health care providers, low hospital COVID census, and no viral surge, patients with high-risk prostate cancer should not be postponed, because we do not know how long this pandemic will last. Delaying the surgical treatment in these patients can lead to more detrimental outcomes, due to the risk of local progression and depreciation of the patient's functional status to face the treatment in the future. Also, the cancer progression may compromise the immune system leading to a higher susceptibility of COVID-19 disease. Furthermore, considering the hospitalization period for a radical prostatectomy <24 hours, appropriate isolation and patient protection during the hospital admission will minimize the virus transmission and ensure that the cancer treatment is performed during the ideal stage.
Evaluating the COVID reality of our center managing the adequate PPI available and ICU capacity are the main basis of the American College of Surgeons (ACS) guidelines management of patients with cancer during the COVID acute phase 1 (our center scenario). 14 All health care workers of our team are using N95 regardless of the patient's COVID status because the rapid tests are not 100% sensitive, and we still have chances of being exposed by COVID false negatives during surgery. The Society of American Gastrointestinal and Endoscopic Surgeons (SAGES) guidelines also have recommendations similar to our actions regarding the preoperative COVID testing, adequate use of PPE regardless of known or suspected COVID status, and pneumoperitoneum evacuation during the trocar removal. 15 It is crucial to remark that when we started the actions in our center managing our patients, most of the current guidelines were not available, and the literature had only a few recommendations with a satisfactory level of evidence.
In the future, the best practices to minimize infections and perform surgeries may include antibody testing of staff and patients to establish COVID-free centers. 6,16 However, in the current scenario, these facilities are not available and we are still learning with this pandemic period. We believe that the actions described in this article are crucial to manage patients with prostate cancer and minimize COVID-19 infection until now. However, since the last week, our state had a substantial increase in the COVID cases, and we still do not have the outcomes of this second wave in our center. We will consider these data in future publications.
Conclusion
Our experience managing patients with prostate cancer in the beginning of the COVID-19 pandemic showed that changing the office routine, stratifying the patients according to the NCCN risk, and adopting COVID-based criteria to select patients for surgery are necessary actions to maintain the best quality of treatment and minimize the viral infection among our oncological patients. In our routine, the RARP during the COVID pandemic is safe and feasible for patients and health care workers if the necessary precautions described in this article are taken. Sharing experience with other centers also improved our understanding of the pandemic scenario worldwide and the required actions to adopt in our center.
Footnotes
Author Disclosure Statement
M.C.M., S.B., F.O., T.R., S.R., M.C.S., B.R., and V.P. declare that no competing financial interests exist with the production of this article. V.P. is consultant for Exact Sciences/Genomic Health, Decipher/Genomic DX, Active Surgical, and AVRA.
Funding Information
No funding was received.