
Abstract
Purpose:
Conventional cystoscopy plays an important role in detection of bladder cancer; however, it is difficult to differentiate benign and neoplastic lesions based on cystoscopic appearance alone. Advanced microscopic modalities, such as confocal laser endomicroscopy and optical coherence tomography, have been shown to provide critical histopathologic information to help identify neoplastic bladder lesions in real time, but their availability and clinical adoption are limited due to a high cost. In this study, we present the first use of a novel and low-cost ($ <5000) confocal high-resolution microendoscope (confocal HRME) for in vivo imaging of bladder lesions.
Materials and Methods:
In a cohort of 15 patients undergoing white light cystoscopy as part of their standard of care, high-resolution images of proflavine-stained bladder lesions were acquired in vivo using the confocal HRME. Based on these images, we evaluated the ability of the confocal HRME to visualize uroepithelium with subcellular resolution and high contrast. Furthermore, we analyzed the cellular architecture and staining patterns of benign and neoplastic bladder lesions in confocal HRME images and compared results to that of standard cystoscopy and histopathology.
Results:
In vivo imaging in the pilot study demonstrates that the confocal HRME resolved subcellular structures of bladder uroepithelium with high contrast. In a wide range of clinical conditions from normal bladder wall to benign and neoplastic lesions, confocal HRME images revealed important diagnostic features that correlated to histopathology.
Conclusions:
The confocal HRME provides an affordable, portable, and easy-to-use tool to allow real-time and high-contrast subcellular characterization of bladder lesions, well suited for bladder cancer detection in community and resource-constrained settings. The
Introduction
In 2020
White light cystoscopy (WLC) is the standard of care for bladder cancer detection and surveillance. Nonetheless, it suffers from several major shortcomings, including inability to detect early cancers and inaccuracy for tumor margin demarcation. 6 To augment urologists' ability to better characterize bladder lesions, novel optical imaging techniques have been developed and evaluated in initial clinical studies.
Overall, these modalities can be categorized into two groups. First, wide-field modalities such as fluorescence cystoscopy and narrow-band imaging have been used to survey large areas of bladder mucosa; these approaches have been shown to improve neoplasia detection rates in comparison to WLC alone. 7 –9 Second, to enable more detailed examination of uroepithelium with microscopic or near-microscopic resolution, optical coherence tomography (OCT) and confocal laser endomicroscopy (CLE) have been utilized in conjunction with standard cystoscopy to help differentiate benign and neoplastic lesions. 10,11 There is early evidence to support the use of multimodal imaging approaches that combine the benefits of wide-field and high-resolution imaging modalities. 12,13
While favorable diagnostic performance for bladder cancer detection has been reported using existing commercial high-resolution imaging modalities, 14 –16 the widespread clinical adoption is hindered by the high cost and limited availability of these technologies. 6 As a low-cost alternative to CLE (≤ $5000 vs ≥ $150,000 for a commercial CLE system), we recently developed a portable confocal high-resolution microendoscope (confocal HRME). 17,18 Unlike CLE based on a scanning laser source, the confocal HRME takes advantage of digitally programmed illumination from the LED of an affordable digital light projector (DLP). Scanning illumination from the DLP is synchronized with a virtual detection aperture on a complementary metal oxide semiconductor (CMOS) sensor, allowing for confocal imaging without mechanical scanning.
Initial ex vivo and in vivo clinical data from the esophagus and cervix show that the confocal HRME can reveal disease-associated morphologic alternations with subcellular resolution, potentially reducing the number of unnecessary biopsies at the point of care. 19 Importantly, compared with nonconfocal imaging, the confocal HRME significantly enhances image contrast of crowded nuclear architecture in highly scattering tissues. 18,20
In this study, we report the first in vivo clinical study to image benign and neoplastic bladder lesions using the low-cost confocal HRME. We demonstrate subcellular-resolution fluorescence imaging of proflavine-stained bladder lesions using the confocal HRME in conjunction with standard WLC. We compare confocal and nonconfocal HRME images of bladder tissue, comparing image contrast and the ability to visualize diagnostically relevant features. Furthermore, we analyze proflavine staining patterns of a range of clinical conditions, from normal bladder wall to benign and neoplastic lesions; these features are compared with WLC images and histopathology.
Materials and Methods
Confocal HRME
The confocal HRME (Fig. 1A) is a probe-based fluorescence confocal microscope that uses a DLP (LightCrafter 4500; Texas Instruments) as the light source and a CMOS sensor (Firefly MV USB 2.0; FLIR Integrated Imaging Solutions, Inc.) for fluorescence imaging. Illumination from the blue LED of the DLP is focused onto a fiber bundle (FIGH-30-850N; Myriad Fiber Imaging) through a collimation condenser and a 10 × objective; fluorescence from tissue in contact with the fiber bundle is then collected and imaged onto the CMOS sensor. The fiber bundle covers a 790 μm field of view (FOV) and can resolve lines 4.4 μm in width.
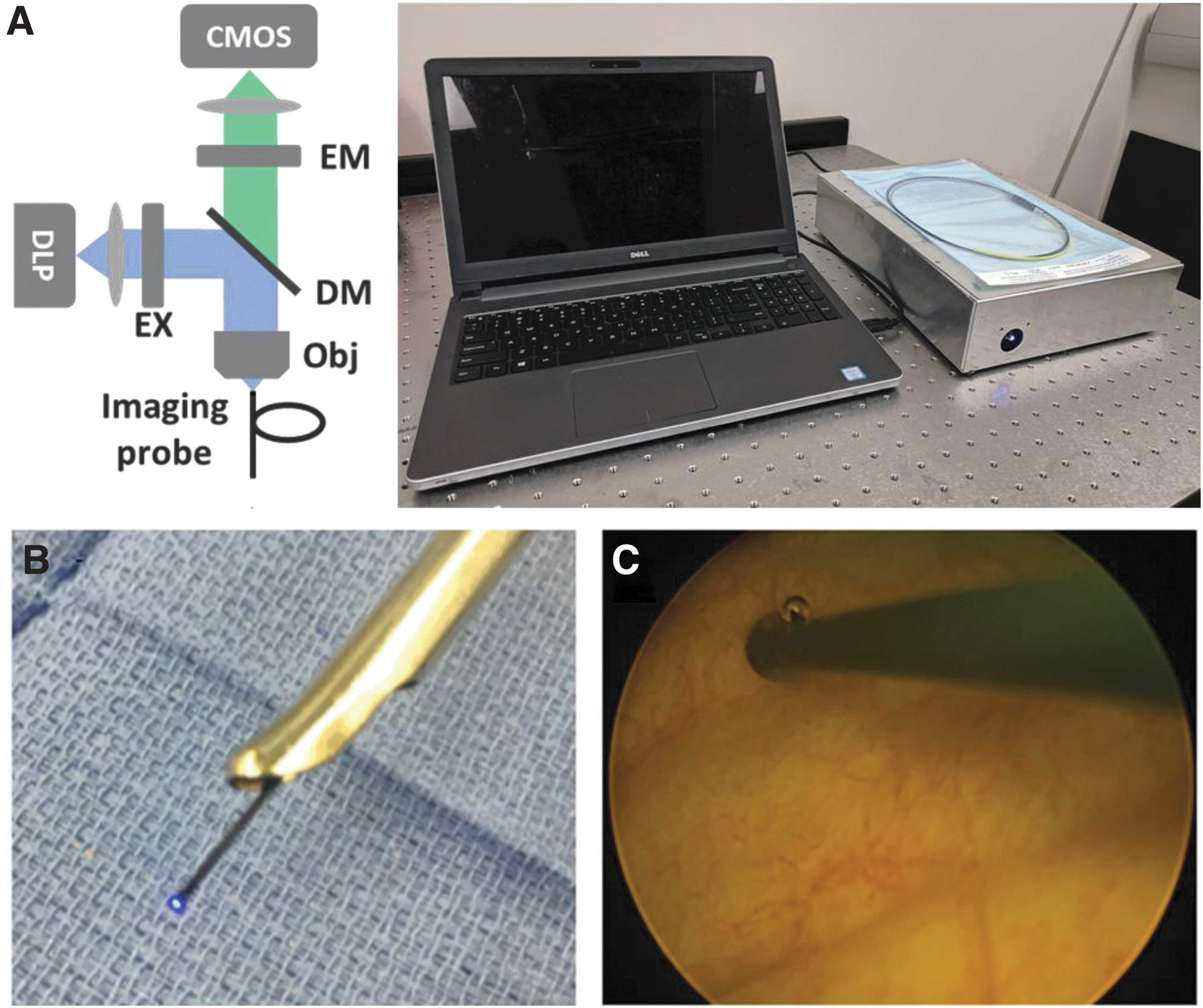
The confocal HRME and its use with standard cystoscopy.
To enable confocal imaging, line-scanning illumination and detection are enabled and synchronized on the DLP and CMOS sensor; detailed aperture design and the resulting background rejection performance were previously described. 17,18 The confocal HRME was built in a compact enclosure (14″ × 10″ × 3″) using commercially available components. A more detailed illustration of the confocal HRME and its cost breakdown is shown in Supplementary Figure S1 in the Supplementary Data.
For in vivo imaging, confocal HRME images were displayed in real time on a laptop, and image acquisition was controlled using a foot pedal. To evaluate the benefits of the confocal HRME for bladder imaging, we programmed the illumination sequence to capture and save two sequential frames in confocal and nonconfocal modes upon depression of a foot pedal trigger.
In vivo imaging
Patients scheduled to undergo standard of care cystoscopy were recruited for in vivo imaging with the confocal HRME at the Lyndon B. Johnson Hospital in Houston, Texas. Participants are enrolled if they have a suspicious bladder lesion or clinical presentation identified by a physician who recommends further evaluation with cystoscopy and bladder biopsy or who are undergoing cystoscopy as part of their routine clinical care. The study protocol was approved by the Institutional Review Boards of the University of Texas Health Science Center at Houston (HSC-MS-12-0144), Harris Health System (14-08-0882), and Rice University (IRB-FY2016-76). Participants were enrolled from February 13th, 2018 to March 21st, 2019; all participants provided written informed consent before enrollment.
During in vivo imaging sessions, WLC was first performed as per standard of care. With the patient under anesthesia, the bladder was inflated with sterile saline and surveyed using standard cystoscopy. Before HRME imaging, the irrigant fluid was drained. Approximately 60 mL of proflavine (0.01% w/v in sterile phosphate-buffered saline) was then instilled into the bladder, and the bladder was surveyed to assess adequacy of distention. Additional proflavine solution was instilled as needed with the goal of using the smallest volume of proflavine possible while permitting sufficient visualization of and access to the target areas. HRME images were then obtained by passing the HRME probe through the endoscopic biopsy channel of the cystoscope (Fig. 1B and Supplementary Video S1) allowing simultaneous HRME and WLC imaging (Fig. 1C).
Post-HRME imaging, the proflavine solution was drained from the bladder and then reinflated with sterile saline. In addition to suspicious lesions, images from normal bladder regions were also acquired to serve as negative control. If clinically indicated, biopsies were obtained as per standard of care and sent for pathologic diagnosis with hematoxylin and eosin staining.
Image analysis
Taking advantage of the versatile digital confocal apertures, we acquired confocal and nonconfocal HRME images sequentially to evaluate the background rejection performance of confocal scanning in nearly identical FOVs during in vivo imaging. The effect of background rejection was assessed by comparing the histogram of pixels within the fiber FOV. To further quantify contrast enhancement, line profiles across important clinical features were compared.
Detailed proflavine staining pattern of bladder epithelium was characterized in 56 imaging sites from 15 patients. To provide clinical context and validation, confocal HRME image features were compared with expert clinical impression based on cystoscopy (N.D.) and the gold standard of histopathology (Z.H.).
Results
In a cohort of 15 patients, we obtained confocal HRME images from 56 imaging sites, including the normal bladder wall, benign, and neoplastic lesions; patient characteristics are shown in Table 1. Biopsies were acquired in 17 sites from 12 patients, and the resulting histopathology was used as the gold standard to evaluate diagnostic features in confocal HRME images.
Patient Characteristics
Figure 2 shows nonconfocal and confocal HRME images of normal bladder wall and a low-grade papillary carcinoma. At both sites, images obtained with the confocal HRME show improved contrast and ability to recognize diagnostically relevant morphology than do images obtained with the nonconfocal HRME. Images of the normal bladder wall (Fig. 2A) show large, interconnected umbrella cells that are round or polygonal shape. Images of low-grade papillary carcinoma (Fig. 2B) show fibrovascular stalks (white arrows) and clusters of large pleomorphic nuclei. At both sites, contrast is lower in the nonconfocal HRME images.

Compared to nonconfocal imaging, the confocal HRME significantly enhances image contrast to allow for characterization of subcellular architecture, including umbrella cell layer in normal bladder wall (site A) and nuclear morphology in low-grade papillary carcinoma (site B; white arrows indicate fibrovascular stalks). Contrast enhancement is compared in the corresponding image histograms and intensity line profiles across clinically important features. Line scans are outlined by white brackets in HRME images; individual umbrella cells and nuclei are indicated by black asterisks and arrowheads in the line profiles, respectively. Circular FOV: 790 μm. FOV = field of view.
With confocal scanning, the network of umbrella cells in site A was readily discerned with clear borders; in site B, individual nuclei were also resolved with high contrast to allow accurate assessment of important histologic parameters such as nuclear size and shape. Corresponding image histograms show the marked reduction of high intensity background associated with confocal gating. Intensity line profiles of important image features (outlined by white brackets in HRME images) show that structures such as umbrella cells and nuclei (black asterisks and arrowheads in the line profiles, respectively) are imaged with higher contrast in confocal images.
Figure 3 shows representative confocal HRME images from different regions of the normal bladder wall together with the corresponding WLC images from three subjects. Macroscopically, no abnormalities were observed in WLC images; as a result, biopsies were not acquired from these sites. Confocal HRME images of normal bladder wall revealed the characteristic cellular morphology of the densely connected umbrella cell layer. The size and shape of umbrella cells differed slightly across different sites and patients, potentially due to variations in bladder filling.

Representative WLC and confocal HRME images of the normal bladder wall in different regions from three patients. WLC images show no abnormalities, and the confocal HRME images reveal characteristic polygonal or round cells that form the umbrella cell layer on normal bladder uroepithelium. Confocal HRME image FOV: 790 μm. WLC = white light cystoscopy.
This interconnected architecture is similar to that previously reported in ex vivo confocal and in vivo CLE imaging of the superficial umbrella cell layer. 11,21 In contrast to nonspecific staining used in fluorescein-based CLE imaging of the bladder wall, proflavine staining of umbrella cells shown here is associated with the highly concentrated cytokeratin beneath the apical membrane, which has a known, strong affinity for proflavine. 22 In the normal bladder uroepithelium, cytokeratin forms a unique, dense, and subapical meshwork in umbrella cells, playing a major role to provide mechanical support and regulate exocytosis during bladder expansion and contraction. 23 –25
While predominantly observed in the normal bladder wall, umbrella cells are also present in certain benign conditions. In Figure 4A, mild erythema was observed during WLC; the confocal HRME image showed a network of large and connected cells indicative of the umbrella cell layer, and the histopathology image confirmed its presence (white box) with mild chronic inflammation.

WLC and confocal HRME images of benign bladder lesions, shown with the corresponding histopathology images (40 × ). Confocal HRME images of sites
In other benign and inflammatory lesions, as shown in Figure 4B and C, the intact umbrella cell layer was disorganized or disrupted. In Figure 4B, an elevated and inflammatory area was identified using WLC. The confocal HRME image revealed dysregulation of the umbrella cell layer, which was consistent with the confirmatory histopathology image. In Figure 4C, increased vasculature was present under WLC; in the confocal HRME image, aggregations of irregularly distributed, small, and monomorphic nuclei were observed, with the histopathology revealing concordant features of acute inflammation.
Representative images of neoplastic bladder lesions are shown in Figure 5. In Figure 5A, a small tumor mass was observed in the WLC image. High-resolution examination using the confocal HRME revealed crowded and irregularly arranged nuclei, with nuclear clusters confined by fibrovascular stalks (white arrows); this microscopic finding was consistent with the histopathology diagnosis of low-grade papillary urothelial carcinoma. In a different patient, a larger mass was identified during WLC in Figure 5B, and the confocal HRME image showed fibrovascular and nuclear features similar to that of Figure 5A. Once biopsied, the lesion was also diagnosed as low-grade papillary urothelial carcinoma.
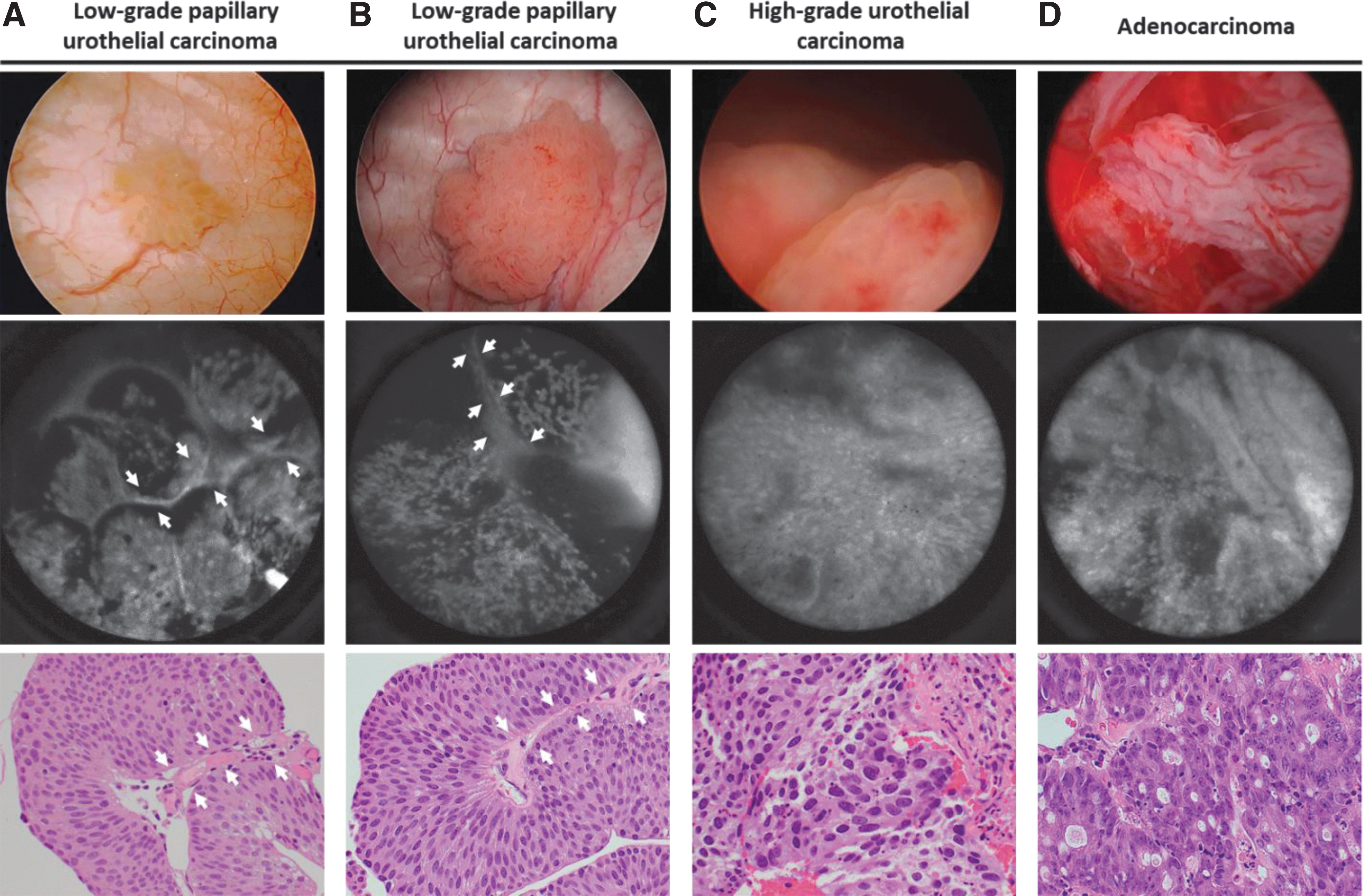
WLC and confocal HRME images of neoplastic bladder lesions, shown with the corresponding histopathology images (40 × ). Confocal HRME and histopathology images in
The lesion in Figure 5C was found in an elevated and erythematous region during WLC. Compared to Figure 5A and B, nuclei in the confocal HRME image of Figure 5C were significantly enlarged, more pleomorphic, and densely packed across the entire FOV. The resulting histopathology image confirmed the confocal HRME finding, and the lesion was diagnosed as high-grade urothelial carcinoma. In the last site in Figure 5D, a tumor identified during WLE was evaluated using the confocal HRME probe, which revealed nuclear crowding and disruption in accordance with histopathology. The corresponding diagnosis was adenocarcinoma; even though it is not a common type of neoplasm in the bladder, the confocal HRME detected microscopic features in agreement with histopathology.
Discussion
In this study, we present the first use of a low-cost confocal HRME for in vivo imaging of bladder lesions. In a cohort of 15 patients undergoing WLC as part of their standard of care, we evaluated the ability of the confocal HRME to image subcellular structures of urothelium with high contrast. Furthermore, we analyzed the staining patterns of benign and neoplastic lesions in the bladder and demonstrated that confocal HRME images reveal diagnostic features that correlate to histopathology.
Previously, HRME has been shown to provide important histologic information for early cancer detection in a wide range of anatomic sites, including the oral cavity, gastrointestinal tract, and cervix. 26 –29 Because of the unique anatomy and physiology of bladder, urothelium imaging in the current work differs from previous studies in several important ways.
First, while topically applied proflavine was used in previous studies, staining of urothelium necessitates intravesical administration. The resulting ubiquitous background from proflavine, combined with inherent scattering from the tissue, significantly impairs the image contrast; as shown in Figure 2, the low contrast of nonconfocal HRME images makes image interpretation challenging. Thanks to the digital confocal scanning mechanism, we show that the confocal HRME can effectively reject this unwanted background, allowing for accurate characterization of important diagnostic features with high contrast.
Second, unlike epithelium in other sites, normal urothelium is lined with a monolayer of densely connected umbrella cells that regulate permeability and provide mechanical strength. Importantly, the umbrella cells are supported by a cytokeratin network, which is known to have strong proflavine staining. 22 As a result, distinct morphologic patterns are observed depending on the presence or absence of umbrella cells. Intriguingly, this unique staining pattern in the bladder is analogous to that in proflavine-stained oral lesions. Several previous studies show that superficial keratinization in the oral cavity, such as the hard palate and gingiva, imposes a barrier for HRME imaging of subsurface nuclei. 30,31 In the current study, we observe that umbrella cells are predominantly present in normal uroepithelium, while disruption or effacement of umbrella cells can be associated with inflammation or neoplastic progression. Taken together, the umbrella cell layer, as well as nuclear morphology of underlying layers, can play important roles for bladder lesion characterization.
Compared to commercially available high-resolution systems such as CLE and OCT that have been reported to show promising results for bladder lesion diagnosis, 15,16 the confocal HRME can provide histologic quality imaging with high contrast at a small fraction of the cost. Moreover, in the current study, we demonstrate the feasibility to use proflavine staining for differentiation of normal and benign conditions from neoplastic lesions in the bladder. In comparison, the CLE system relies on intravenously administered fluorescein to provide contrast, and OCT visualizes subcellular architectural features based on backscattering. Like other high-resolution modalities, the confocal HRME probe has a limited FOV and can also benefit from a two-step imaging protocol when used in conjunction with a wide-field imaging technique.
Future studies are warranted to establish and evaluate the diagnostic criteria of the confocal HRME in a larger sample size, which can be used to train novice users. In addition, machine learning algorithms can also be developed to facilitate image interpretation and assist clinical decision-making.
Conclusion
In conclusion, we report the first in vivo study to image bladder lesions using a low-cost and portable confocal HRME. Using clinical data, we demonstrate that background rejection in the confocal HRME is necessary for accurate characterization of proflavine-stained bladder lesions. Furthermore, our preliminary results show that the confocal HRME can visualize important diagnostic features in various clinical conditions that correlate to histopathology. Its capability to provide real-time and high-contrast imaging of bladder lesions at a low cost warrants future larger scale clinical evaluations to further evaluate its diagnostic performance, especially in resource-constrained and community settings.
Footnotes
Acknowledgments
The authors thank Timothy Quang, Katelin Cherry, and Divya Jain for their assistance with the research and preparing the article. The authors also thank Comalita Lee for coordinating the clinical research.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This work is supported through the Cancer Prevention and Research Institute of Texas (CPRIT) grant number RP160460.
Supplementary Material
Supplementary Data
Supplementary Figure S1
Supplementary Video S1
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.