
Abstract
Introduction:
The current study evaluated the efficacy and safety of external physical vibration lithecbole (EPVL) after extracorporeal shock wave lithotripsy (SWL) or retrograde intrarenal surgery (RIRS) for urolithiasis.
Methods:
Publicized literature was systematically searched from EMBASE, Cochrane Library, PubMed, ScienceDirect, ClinicalTrials.gov, and Web of Science up to February 2020. Fixed-effects or random-effects model was chosen in risk ratio (RR) calculation according to heterogeneity. Quality of evidence was estimated under the guidance of Cochrane handbook. Stone expulsion rate, stone-free rates (SFRs), and complication rates were set as end points.
Results:
Six randomized controlled trials, including 853 patients, were eligible for analysis. EPVL significantly increased SFR within 3 weeks (RR = 1.17, 95% CI: 1.06–1.29, P = 0.001) and above 3 weeks (RR = 1.19, 95% CI: 1.03–1.37, P = 0.02) after SWL. EPVL also improved SFR within 3 weeks (RR = 1.84, 95% CI: 1.35–2.49, P < 0.0001) and above 3 weeks (RR = 1.53, 95% CI: 1.33–1.77, P < 0.00001) after RIRS. Besides, EPVL can significantly increase SFRs for stones in renal pelvis, lower calix, and multiple locations (all P-value <0.05). Although the overall complication rate was not significantly higher in EPVL + RIRS group, it was found to be 1.38 times higher in EPVL+SWL group (RR = 1.38, 95% CI: 1.06–1.79, P = 0.02), especially the incidence of flank pain (RR = 3.11, 95% CI: 1.02–9.46, P = 0.05).
Conclusions:
EPVL is effective and safe with high SFRs (especially in renal pelvis, lower calix, and multiple locations) after SWL or RIRS and lower overall complication rate after RIRS in patients with urolithiasis. However, the overall complication rate (especially the incidence of flank pain) was higher after EPVL + SWL.
Introduction
Urinary stone disease is the most common condition in urology, with an increasing prevalence of 2%–20% all over the world. 1 The recurrence rate is as high as 50% within the first 5 years after the first stone episode and increases to 75% within 20 years. 2,3 Because of its efficacy, safety, and minimal invasiveness, extracorporeal shock wave lithotripsy (SWL) is regarded as the first-line therapy for urinary stones <2 cm. 4 Recently, retrograde intrarenal surgery (RIRS) has been widely applied for its lower complication rates, blood loss, and admission times than percutaneous nephrolithotomy (PCNL) and better stone clearance than SWL. 5,6 However, the residual stone fragments after SWL or RIRS can be hard to discharge, which is possible to be the source of infection, obstruction, and hematuria. 7 –9 Besides, around half of the asymptomatic residual stone fragments may regrow and enlarge, leading to stone recurrence. 10 Therefore, it has been an urgent need to promote the expulsion of residual stone fragments and increase the stone-free rates (SFRs) after SWL or RIRS.
Expulsion of stone fragments can be affected by many factors, including stone size, location of residual stones, urinary tract stenosis, the internal structure of stones, and external forces. 11 –14 Many interventions, such as expulsive medical therapy, ultrasonic propulsion, or movement and physical therapy, have been applied to promote stone fragment discharge. Still, the results of safety and efficacy were inconsistent. 15 –17 Among these interventions, physical therapy, including mechanical percussion, diuresis, and inversion (PDI) therapy, was deemed to be tolerated and effective in the expulsion of stone fragments since Kirsch and coworkers first applied mechanical vibration for urolithiasis treatment in 1965. 15,18 Therefore, physical therapy has been recommended for improving SFRs and accelerating stone passage after SWL. 19 As a novel noninvasive device applied for years, external physical vibration lithecbole (EPVL) applied the mechanical percussion and inversion but not the diuresis principle of PDI therapy. This device can promote residual stone fragment discharge with mechanical vibration and inversion. EPVL is a therapeutic bed consisting of one main and one sub oscillator. Patients need to drink 1000–3000 mL water before therapy and lie on the bed in a lateral or prone position without anesthesia. Then the oscillators produce harmonic vibration waves from multiple directions (the power is 20 W, the vibration frequency is 2800–3500 blows/min, and the amplitude is 5 mm) controlled by inertial guidance system to help separate the stones from the kidney or ureter. Besides, the angle of the bed can be adjusted from −26° to 26° to change the relative position of the stones. As a result, the fragments can be discharged smoothly. 20,21 The whole stone expulsion process is monitored by ultrasound.
Although some previous studies have already analyzed the safety and efficacy of EPVL after SWL or RIRS in urinary stone patients, there is still insufficient evidence to demonstrate its efficacy on stone fragment discharge due to the small sample size. 20 –25 Besides, complications of EPVL after SWL or RIRS, such as hematuria, urine white blood cell (WBC) rise, flank pain, and fever, were reported as well. Thus, extra evidence is still required to support the safety of EPVL. In this research, we performed a comprehensive meta-analysis to assess the efficacy and safety of EPVL after SWL or RIRS therapy in patients with urinary stones.
Method
Search strategy
Literature in EMBASE, Cochrane Library, PubMed, ScienceDirect, ClinicalTrials.gov, and Web of Science up to February 2020 was systematically searched to find related studies and clinical trials. The keywords used in our search strategy were “external physical vibration lithecbole,” “extracorporeal shock wave lithotripsy,” and “retrograde intrarenal surgery.” The references in the searched articles were reviewed as well. No restrictions on sample size or publication years were set.
Study eligibility
The selecting criteria were that only randomized controlled trials (RCTs) with randomly assigned urinary stone patients who received (1) EPVL+SWL or EPVL+RIRS combination therapy or (2) SWL or RIRS monotherapy. Retrospective studies and observational studies without control groups were excluded, as well as editorials, correspondence, meta-analysis, articles that are irrelevant to the research theme, comments, sympathetic review, and case reports.
Quality assessment
We estimated the quality of selected RCTs under the guidance of the Cochrane handbook for systematic reviews of interventions. 26 This study evaluated detection bias (blinding of outcome assessment), selection bias (random sequence generation and allocation concealment), attrition bias (incomplete outcome data), reporting bias (selective reporting), performance bias (blinding of participants and personnel), and other bias.
End points and data collection
Two independent investigators collected data from the selected RCTs, which contain baseline information (author, year of publication, arms, and region), demographic and clinical characteristics (e.g., gender, age, hydronephrosis degree, follow-up time points, mean stone size), and therapeutic end points. SFRs and stone expulsion rates (SERs) were the primary end points. Stone free was regarded as no visible stone fragments on plain film with or without ultrasonography in ureter, bladder, and kidney. Correspondingly, SFR was defined as the proportion of the stone-free population to the total population. SER was prescribed as the ratio of the number of patients with any stone fragment discharge to total patient number. 22 Compared with SFR, the SER does not empathize with the thorough clearance of stone fragments. The secondary end points were the overall complication rates, including the incidences of hematuria, urine WBC rise, flank pain, fever, and dizziness.
Statistical analysis
Review Manager 5.3 (The Cochrane Collaboration) was applied to conduct meta-analysis with extracted data. We applied χ 2 statistic for the heterogeneity evaluation and I 2 statistic for inconsistency assessment in the selected RCTs. We chose the fixed-effects model in risk ratio (RR) calculation for dichotomous data when little or no heterogeneity exists (P > 0.1). When heterogeneity was moderate or large (P < 0.1), we applied the random-effects model instead. P-Value ≤0.05 was considered statistically significant in this meta-analysis. Moreover, we described the 95% confidence interval as 95% CI of the meta-analysis in the result section.
Results
Characteristics of the reviewed studies
As the flow diagram shown in Supplementary Figure S1, there were in total 91 articles and clinical trials identified during the searching process. Among them, 31 articles were from ScienceDirect, 19 from EMBASE, 9 from PubMed, 4 from ClinicalTrials.gov, 16 from Cochrane Library, and 12 from Web of Science. According to the titles, abstracts, and eligibility criteria, we excluded 85 publications. Totally, there were six RCTs included. 20 –25 All the studies except one 24 have mentioned the particular random method. The quality assessment for the selected RCTs is shown in Supplementary Figure S2.
The detailed characteristics of selected articles were summarized (Table 1). Among all the six RCTs, three focused on EPVL after SWL, 20,22,23 and the other three focused on EPVL after RIRS. 21,24,25 In total, 853 patients (580 males, 273 females) were included and assigned randomly, in which 237 patients received EPVL and SWL combination therapy, 258 only received SWL, 188 patients received EPVL and RIRS combination therapy, and 170 only received RIRS. As for the studied urinary stone types, two RCTs focused on upper urinary stones, 21,23 two on renal or upper ureteral stones, 24,25 one on stones in upper ureter, 20 and one on renal stones in lower pole. 22 The stone size of included patients ranged from 1.5 to 20.91 mm, and the ages ranged from 42.7 to 50.4 years old.
Baseline Information of Included Articles
EPVL = external physical vibration lithecbole; SWL = extracorporeal shock wave lithotripsy; N/A = data not avaliable; RIRS = retrograde intrarenal surgery; SD = standard deviation.
Meta-analysis of efficacy
Stone-free rate
All six RCTs reported the SFRs (Supplementary Table S1), among which four RCTs contained 597 patients with SFRs within 3 weeks after SWL or RIRS (Fig. 1a). Moderate intergroup heterogeneity (P = 0.009 and I2 = 74%) was found, so random-effects model was applied. However, we observed no intragroup heterogeneity for P-value >0.1 and I2 = 0% in both groups. The results suggested that EPVL add-on therapy significantly increased the SFRs within 3 weeks after SWL or RIRS, in which the SFR of EPVL+RIRS was 1.84 times higher compared with RIRS group with clinical significance (RR = 1.17, 95% CI: 1.06–1.29, P = 0.001 for EPVL+SWL and SWL groups, RR = 1.84, 95% CI: 1.35–2.49, P < 0.0001 for EPVL+RIRS and RIRS group, and RR = 1.39, 95% CI: 1.09–1.77, P = 0.008 for total effect). Further subgroup analysis demonstrated that EPVL add-on therapy could significantly increase the SFRs at 2 weeks after SWL or RIRS, while no statistical difference was found at 1 week after therapy (Supplementary Fig. S3).
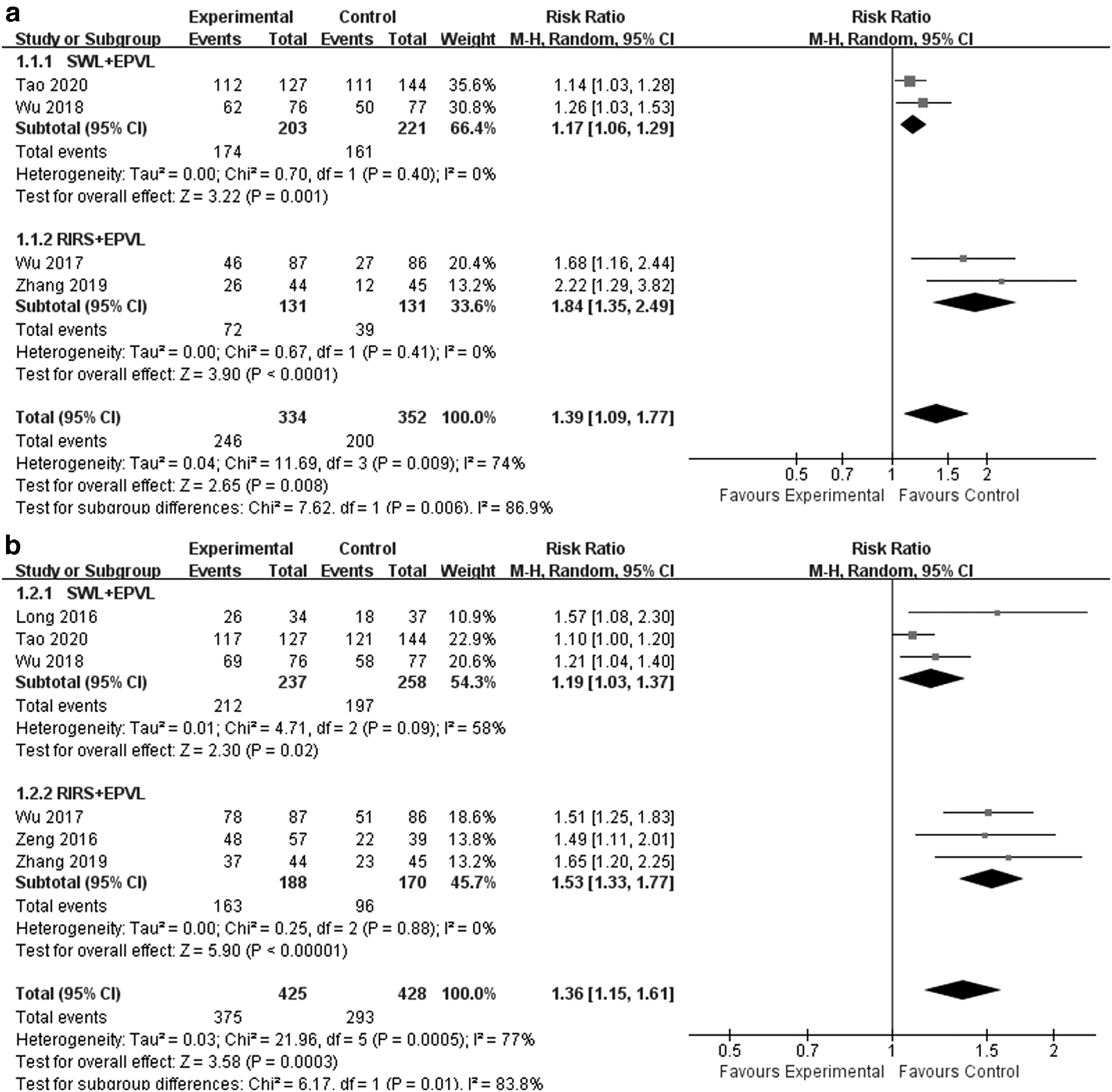
Results of the meta-analysis on the SFR
All the six RCTs recorded SFRs more than 3 weeks after SWL or RIRS (Fig. 1b). We observed moderate intergroup heterogeneity (P = 0.0005 and I2 = 77%) and intragroup heterogeneity in EPVL+SWL and SWL group (P = 0.09 and I2 = 58%) but not in EPVL+RIRS and RIRS group (P = 0.88 and I2 = 0%). The pooled results indicated that EPVL add-on therapy significantly increased the SFRs more than 3 weeks after SWL or RIRS, in which the SFR of EPVL+RIRS was 1.53 times higher compared with RIRS group with clinical significance (RR = 1.19, 95% CI: 1.03–1.37, P = 0.02 for EPVL+SWL and SWL group, RR = 1.53, 95% CI: 1.33–1.77, P < 0.00001 for EPVL+RIRS and RIRS group, and RR = 1.36, 95% CI: 1.15–1.61, P = 0.0003 for total effect). Further subgroup analysis found that EPVL add-on therapy increased SFR with statistical difference at 3, 4, and 5 weeks after SWL or RIRS (Supplementary Fig. S3), demonstrating a good long-term therapeutic effect of EPVL.
Since stone size was an important risk factor for SFRs after SWL or RIRS, we conducted meta-analysis for SFRs with different stone sizes at the last follow-up. The mean stone size in all three SWL RCTs was less than 15 mm (only one RCT <10 mm), and all three RIRS RCTs were more than 15 mm. The results showed that EPVL add-on therapy significantly increased the SFRs when the mean stone size was less than 10 mm (RR = 1.10, 95% CI: 1.00–1.20, P = 0.04) or more than 15 mm (RR = 1.53, 95% CI: 1.33–1.77, P < 0.00001), except when the size ranged from 10 mm to 15 mm. After all, EPVL add-on therapy could increase the SFRs in total effect (RR = 1.32, 95% CI: 1.13–1.55, P = 0.0006) (Supplementary Fig. S4). Further subgroup analysis demonstrated the effectiveness of EPVL in improving SFRs of different stone sizes at different time points (except the SFRs with a mean stone size ranging from 10 mm to 15 mm at 1 week after therapy) (Supplementary Fig. S5).
Three of the selected RCTs mentioned SFRs in different locations. The results demonstrated higher SFRs in the renal pelvis, multiple locations, and lower calix in EPVL+SWL or EPVL+RIRS combination therapy groups than SWL or RIRS monotherapy groups with significant difference (Supplementary Figs. S6–S8). The same is true of EPVL+RIRS and RIRS subgroup analysis (all P-value <0.05). No significant difference of SFRs in upper and middle calix was found between EPVL+SWL or EPVL+RIRS combination therapy groups and SWL or RIRS monotherapy groups (Supplementary Figs. S9 and S10).
Stone expulsion rate
Two RCTs, including 342 patients, reported the SER 1 day after EPVL (Supplementary Fig. S11). Considering that there was a moderate heterogeneity (P = 0.1 and I2 = 63%) between individual trials, the random-effects model was applied. The pooled result demonstrated that EPVL application after SWL therapy did not significantly increase the SER 1 day after EPVL compared with SWL monotherapy (RR = 1.40, 95% CI: 0.99–1.98, P = 0.06).
Meta-analysis of safety
The overall complication rate in which incidences of hematuria, urine WBC rise, flank pain, fever, and dizziness were included was not statistically significant in total effect tests. Still, the results of the subgroup analysis showed the opposite trend (Fig. 2). For the EPVL+RIRS group, although no statistical difference has been found, the overall complication rate tended to be lower compared with the RIRS group (RR = 0.91, 95% CI: 0.82–1.00, P = 0.06). Compared with SWL monotherapy, EPVL add-on therapy could significantly increase the overall complication rate by 1.38 times after SWL therapy (RR = 1.38, 95% CI: 1.06–1.79, P = 0.02). Besides, in EPVL+SWL and SWL subgroup analysis, the incidence of flank pain, which was the primary complication of EPVL, was 3.11 times higher in the EPVL+SWL group with obvious clinical significance (RR = 3.11, 95% CI: 1.02–9.46, P = 0.05), suggesting that EPVL therapy after SWL is possible to cause more flank pain (Fig. 3). No statistical difference was found in further subgroup analysis for the incidence of flank pain at 1 or 2 weeks after therapy, and no patients reported flank pain after 4 weeks (Supplementary Fig. S12).
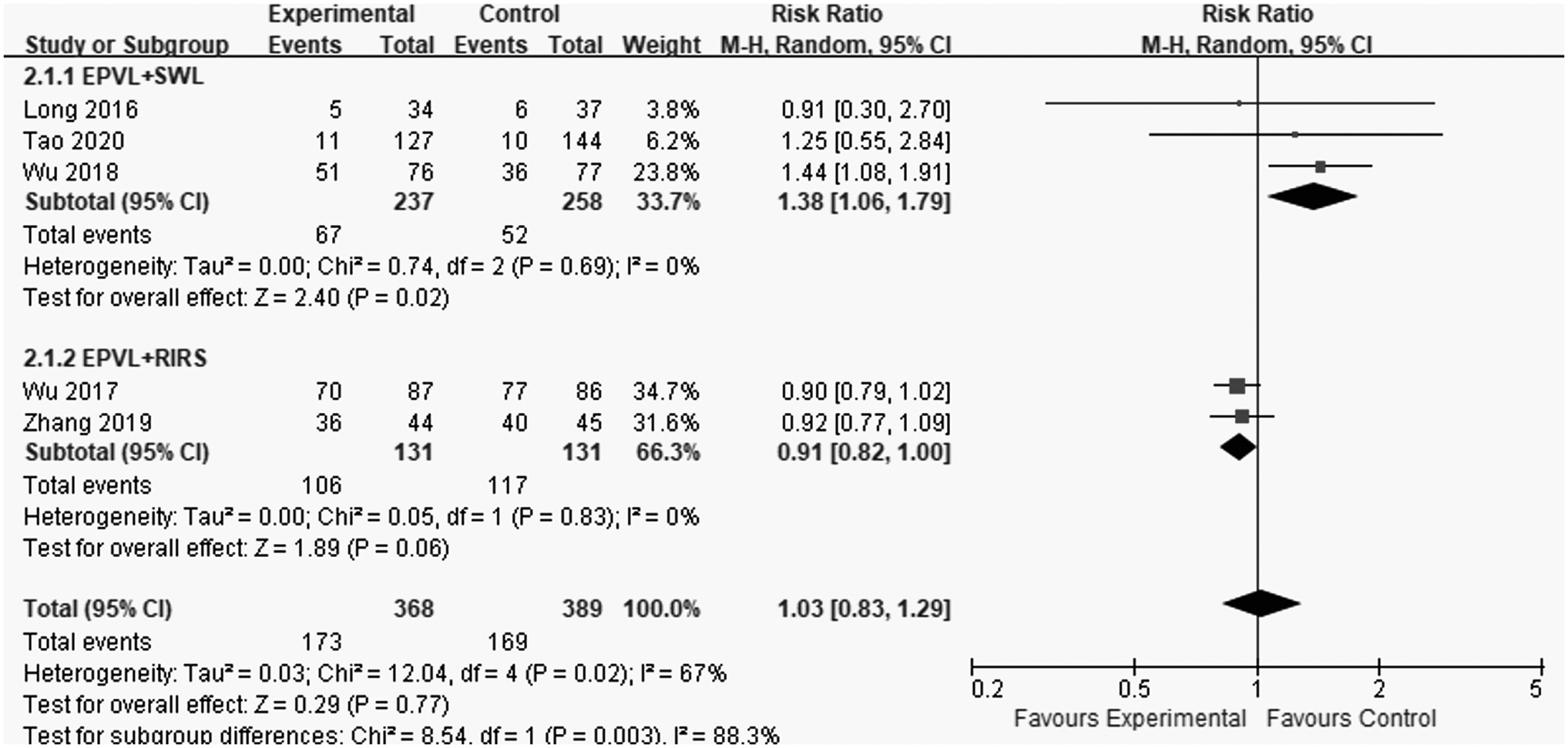
Results of the meta-analysis on the overall complication rate. Experimental: EPVL+SWL or EPVL+RIRS combination therapy group; Control: SWL or RIRS monotherapy group.
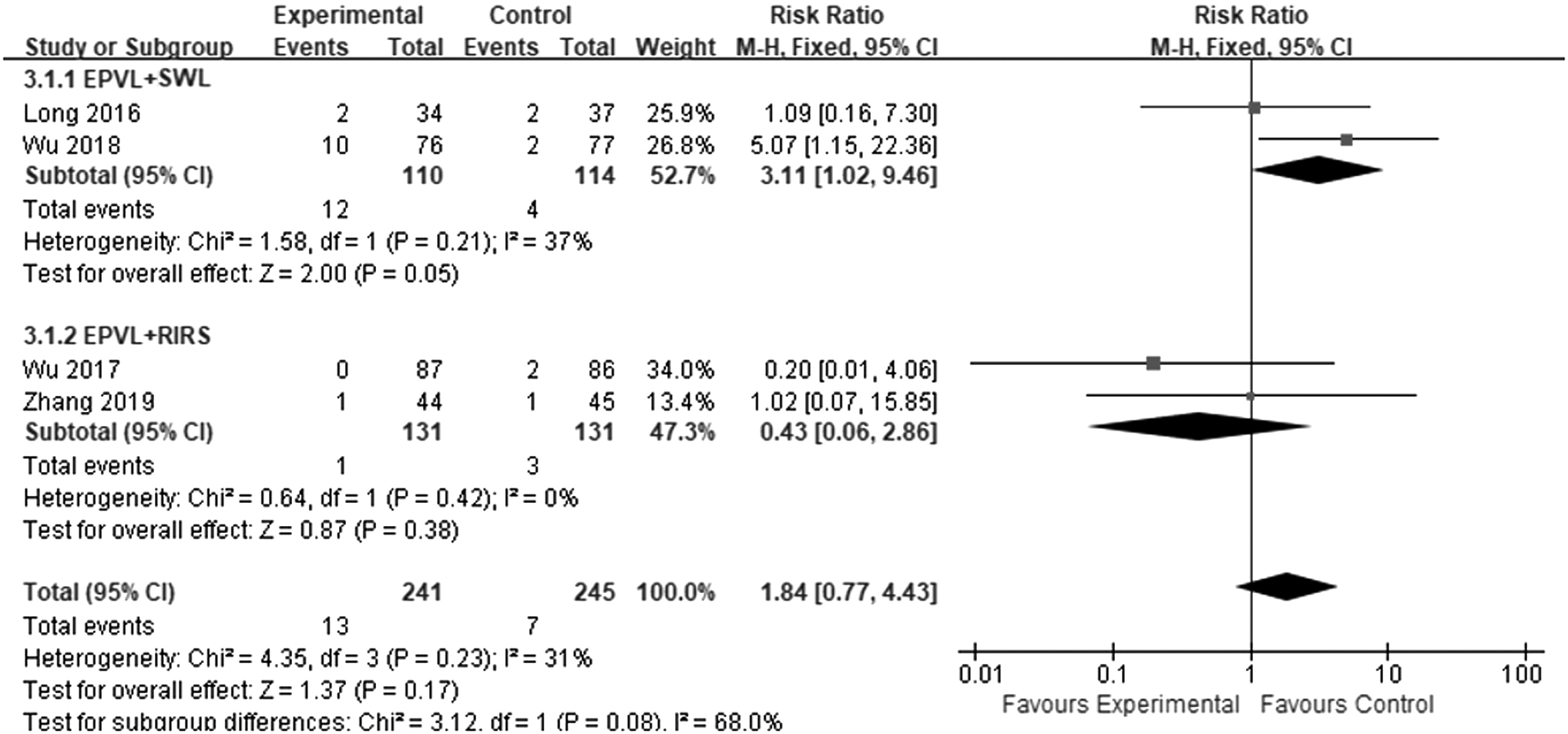
Results of the meta-analysis on the incidence of lumbago. Experimental: EPVL+SWL or EPVL+RIRS combination therapy group; Control: SWL or RIRS monotherapy group.
In terms of specific incidence of complications, all the selected six RCTs that reported the most common complications in EPVL add-on therapy after SWL or RIRS were hematuria, urine WBC rise, flank pain, and fever. Our pooled results indicated that the EPVL add-on therapy did not significantly influence the incidence of complications mentioned above compared with SWL or RIRS monotherapy in total effect analysis (hematuria: RR = 0.92, 95% CI: 0.75–1.13, P = 0.41; urine WBC rise: RR = 0.89, 95% CI: 0.75–1.06, P = 0.19; flank pain: RR = 1.84, 95% CI: 0.77–4.43, P = 0.17; fever: RR = 0.59, 95% CI: 0.17–2.14, P = 0.43) (Supplementary Figs. S13–S15 and Fig. 3). The subgroup analysis demonstrated that EPVL could significantly reduce hematuria at both 3 and 4 weeks after EPVL+RIRS therapy (Supplementary Fig. S13). Still, no statistical difference for urine WBC rise was found at any time points (Supplementary Fig. S14). Three RCTs recorded the incidence of dizziness while no statistical difference was found (RR = 2.77, 95% CI: 0.88–8.72, P = 0.08) (Supplementary Fig. S16). In general, the overall complication rate increased in the EPVL+SWL group but was similar between EPVL+RIRS and RIRS group. The incidences of hematuria, urine WBC rise, flank pain, and fever were not different between the EPVL+SWL or EPVL+RIRS combination therapy group and the SWL or RIRS monotherapy group in total effect analysis. In the subgroup analysis between EPVL+SWL and SWL, the incidence of dizziness was similar while that of flank pain increased obviously.
Discussion
The prevalence of nephrolithiasis had been increasing from 6.4% to 7.54% between 2013 and 2016 in China. 27,28 Similarly, it was reported that every 1 out of 11 people suffers from urinary stones in the United States. 29 With an annual medical cost of more than $10 billion, urinary stone causes a vast and growing burden to public health and it has become the most expensive urologic disease. 30 In recent years, SWL and RIRS have been widely applied for their excellent therapeutic effect, minimally invasive properties, low complication rate, and favorable patient tolerance. 2,6 However, the SFRs of SWL or RIRS were lower than PCNL, 5,31 and residual stone fragments are likely to lead to unexpected stone movement, potential enlargement, and even reocclusion of the urinary tract. 8,32 Therefore, a noninvasive device, EPVL, has been applied to help discharge the residual stone fragments and improve the SFR after SWL or RIRS.
Our meta-analysis demonstrated that the EPVL add-on therapy significantly increased the SFR both within and more than 3 weeks after SWL or RIRS, in which results of subgroup analysis remained consistent with the total effect analysis. Moreover, the SFR improvement in EPVL+RIRS and RIRS was more significant than that in the EPVL+SWL and SWL groups. The superiority of EPVL in SFR after SWL or RIRS can be explained by EPVL's mechanism, which combines the inverted position with mechanical percussion, adjusts the angle of the therapeutic bed according to the patient's condition, and finally removes the stone fragments from the body. 21,25 At the same time, EPVL can pressure the patients’ renal area with the main oscillator, thereby promoting the separation of stones and tissues in the patient's kidney. The accompanying ultrasonic examination equipment can accurately observe the position of the stones. The combination of the oscillator and ultrasound can promote the expulsion of residual stone fragments. 22
Moreover, we also found higher SFRs of stones in the renal pelvis, lower calix, and multiple locations in the EPVL+RIRS group, which indicated that EPVL could promote the clearance of stones that were difficult to discharge. Previous studies have found that it is more difficult to discharge residual stone fragments in the lower calix than those in the middle or upper calix. 33 This can be related to the deposition of stone fragments by the gravity factor and the unique anatomy of the lower calix, although this hypothesis is still controversial. 11,34,35 Pace and associates 36 found that mechanical percussion and inversion therapy in Trendelenburg position could substantially increase the SFRs of residual stone fragments in the lower pole than the observation group at 3 months after SWL (40% and 3%, respectively, P < 0.01). The results indicated that percussion, inversion, and position were possible to affect the stone expulsion in the lower calix, which was consistent with our results. The therapeutic bed of EPVL could adjust patient into Trendelenburg position flexibly with a rotation angle from −26° to 26°, in which the lower renal calix is in a relatively higher position with the caliceal opening facing down. Therefore, it can be concluded that EPVL can promote the stone expulsion in the lower calix along with mechanical percussion. 21
However, in our meta-analysis, the SER 1 day after EPVL + SWL did not increase significantly compared to SWL monotherapy. This can be attributed to the incomplete recovery of urinary tract mucosal edema caused by tissue hypoxia coming out of interstitial capillary rupture after SWL, which can prevent residual stone fragments from being discharged. 37 In addition, Long and coworkers 22 reported that the mean time for first expulsion in EPVL+SWL group was 11.2 minutes and in SWL group was 9.17 hours (P = 0.016). In EPVL+RIRS and RIRS groups, the time for stone clearance was 15.4 ± 1.0 and 19.0 ± 1.5 days, respectively (P = 0.02). 24 These results indicated that EPVL might shorten the therapeutic time and accelerate stone discharge. Besides, it might be easier for medical staff to collect stone samples from patients in the EPVL group for further component analysis during the treatment period, which could help to make a precise and personalized treatment plan. However, more data about therapeutic time are needed to make a more rigorous conclusion.
The EPVL after SWL or RIRS was well tolerated, and no severer complications were observed. The overall complication rate was higher in EPVL + SWL groups than in the SWL groups (P = 0.02), while it was similar between the EPVL + RIRS groups and the RIRS groups (P = 0.06). Considering that the SWL is already a minimally-invasive operation, the rising overall complication rate in the EPVL + SWL group can be explained by the excessive activity of residual stone fragments during the accelerated expulsion by EPVL, resulting in increased hematuria and low back pain. Besides, the increased dizziness was likely to result from the rotation of the therapeutic bed. 22,23 Moreover, the incidences of common complications were similar between the EPVL+SWL or EPVL+RIRS combination therapy groups and the SWL or RIRS monotherapy groups according to our pooled analysis. Only one RCT reported incidence of Steinstrasse in the EPVL+SWL and the SWL subgroup, whereas no significant difference was found. It is worth mentioning that although the incidence of flank pain was found higher in the EPVL+SWL groups than the SWL group, the P-value was exactly equal to 0.05, which was a marginal P-value. Considering the relatively insufficient number of samples, studies, and different locations of stones, we are cautious about this conclusion. More data are needed for further analysis to get more rigorous conclusions.
The objective of this sympathetic review and meta-analysis was to assess the safety and efficacy of EPVL after SWL or RIRS in urolithiasis patients. Although heterogeneity was observed in some meta-analysis, it mainly came from intergroup due to the different types of therapies, while not from intragroup. Besides, most of the results in subgroup analysis remained consistent with the total effect analysis. Therefore, the results of this meta-analysis were of great clinical significance, and it is expected that our study will contribute to the clinical guidelines for better efficacy in urinary stone treatment after RIRS or SWL.
However, there were several limitations to our analysis. First, this meta-analysis only selected six RCTs with relatively insufficient sample size. Second, the follow-up time of each RCT was not consistent, and more long-term follow-up data were not available, so that we could not evaluate the long-term safety and efficacy of EPVL. Third, the data of the baseline mean stone size were different in subgroups, with 1.5–11.2 mm in the EPVL+SWL and the SWL groups and 15.2–20.91 mm in the EPVL+RIRS and the RIRS groups. Besides, the analysis was not successfully completed in terms of the end points such as SFR in proximal ureter, hospitalization time, the incidence of perirenal hematoma, and red skin due to the limited data size. The limitations mentioned above are possible to bring bias to the results. Still, the study inclusion, data extraction, and meta-analysis were all strictly performed to reduce the impacts of these deficiencies on the analysis results. Nevertheless, more high-quality and long-term RCTs are required to verify the efficacy and safety of EPVL after SWL or RIRS in patients with urinary stones.
Conclusion
Our meta-analysis indicated that EPVL is an effective and tolerated therapy with higher SFRs (especially in the lower calix, multiple locations, and renal pelvis) after SWL or RIRS in the urolithiasis patients. Lower complication incidences after EPVL +RIRS were found, but the overall complication rate (especially the incidence of flank pain) was higher after EPVL +SWL. Based on the results of our meta-analysis, large-scale multicenter RCTs are required to provide more reliable evidence.
Footnotes
Availability of Data and Materials
The data supporting the conclusions of this article are shown within the article and its supplementary files.
Authors' Contribution
Conception and design: Chi Yuan, Zhongyu Jian; Acquisition of data: Chi Yuan, Zhongyu Jian, Xi Jin; Analysis and interpretation of data: Chi Yuan; Xi Jin, Yucheng Ma, Hong Li; Drafting of the article: Chi Yuan, Zhongyu Jian, Xi Jin, Yucheng Ma; Critical revision of the article for important intellectual content: Chi Yuan, Zhongyu Jian, Hong Li, Kunjie Wang; Statistical analysis: Chi Yuan, Zhongyu Jian, Yucheng Ma; Obtaining funding: Hong Li, Kunjie Wang; Administrative, technical, or material support: Xi Jin, Yucheng Ma; Supervision: Kunjie Wang.
Author Disclosure Statement
The authors declare that there is no conflict of interests regarding the publication of this article.
Funding Information
This study was found by 1.3.5 project for disciplines of excellence, West China Hospital, Sichuan University (ZYGD18011, ZY2016104, ZYJC18015), Project of Sichuan Provincial Health Department (ZH2017-101), and Project of Sichuan Provincial Health Department (2018SZ0118).
Supplementary Material
Supplementary Figure S1
Supplementary Figure S2
Supplementary Figure S3
Supplementary Figure S4
Supplementary Figure S5
Supplementary Figure S6
Supplementary Figure S7
Supplementary Figure S8
Supplementary Figure S9
Supplementary Figure S10
Supplementary Figure S11
Supplementary Figure S12
Supplementary Figure S13
Supplementary Figure S14
Supplementary Figure S15
Supplementary Figure S16
Supplementary Table S1
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.