
Abstract
Introduction:
Single-use flexible ureteroscopes are an increasingly popular alternative to reusable ureteroscopes. In this study, we performed a benchtop examination of the physical and optical properties of the new Dornier Axis™ (Webling, Germany) single-use ureteroscope.
Methods:
Ten new, never-used Dornier Axis ureteroscopes were assessed for optical performance, maximal tip deflection, and irrigation flow rate with an empty working channel and with insertion of 200 and 365 μm laser fibers, and a 1.9F nitinol basket. All ureteroscopes were then fully deflected 100 times in each direction, and maximal deflection angles were re-measured with and without instruments in the working channel. All measurements were performed in duplicate. In vitro optical testing for resolution, image distortion, and depth of field was performed and compared vs the LithoVue™ (Boston Scientific, Marlborough, MA) single-use ureteroscope. Statistical analyses using paired Wilcoxon rank-sum tests and Kruskal–Wallis multiple-group comparison tests were performed in R.
Results:
Median maximal deflection angles exceeded 300° in both directions before and after 100 full deflection cycles for all groups except the 365 μm laser fiber group. After 100 deflection cycles, there was no change in the majority of working instruments, except a decrease in upward flexion with an empty channel and 200 μm Moses™ laser fiber, and downward flexion with 200 μm Flexiva™ laser fiber (all <10°). After excluding the 365 μm fiber, there was no difference in multi-group comparison for upward and downward flexion pre- and post-cycling. Median flow rate through an empty channel was 48.0 mL/min, and it decreased significantly with all used instruments (p < 0.001). Compared with the LithoVue, the Axis demonstrated superior resolution at all tested distances and less distortion.
Conclusions:
The new Dornier Axis single-use ureteroscope demonstrates excellent tip deflection, which remains unchanged after 100 manual flexions in each direction. The Axis also demonstrates superior optical performance compared with the LithoVue in benchtop testing.
Introduction
Nephrolithiasis continues to increase in incidence in the United States. 1 Ureteroscopy (URS) is the recommended treatment option for distal and mid-ureteral stones that fail medical therapy, a recommended option (vs shockwave lithotripsy) for proximal ureteral stones that fail medical therapy, and for ureteral stones >10 mm or suspected cystine or uric acid stones. URS is also recommended for renal stone burden ≤10 mm in the lower pole and ≤20 mm elsewhere in the kidney. 2,3 Ureteroscope technology has continued to improve since the development of the first rigid ureteroscope several decades ago, culminating in the current generation of reusable, high-definition, digital flexible ureteroscopes that are capable of multiple different functionalities. 4 The drawback of these advanced reusable scopes, however, is that they require significant initial capital investment and subsequently may require frequent repair at considerable cost. 5 –7 Additional concerns include the significant time and skilled labor resources required for appropriate processing and cleaning 8 as well as some case reports that have identified the role of reusable endoscopes in the spread of multidrug-resistant infections. 9,10
As a result of these limitations, single-use ureteroscopes have been developed. Their overall functionality compares well with reusable ureteroscopes in a wide array of clinical scenarios. 11,12 The Boston Scientific (Marlborough, MA) LithoVue™ ureteroscope is the most widely used single-use ureteroscope in the United States. The LithoVue has a 9.5F outer diameter and a 3.6F working channel inner diameter. 13 However, several other single-use ureteroscopes, including the Pusen (Guangdong, China) UScope PU3022, have been developed and are available internationally. 14 Recently, Dornier (Webling, Germany) introduced the Axis™ single-use ureteroscope, which received Food and Drug Administration (FDA) approval in January 2019. 15 The Axis has an 8.5F outer diameter and a 3.6F working channel inner diameter. In this study, we performed benchtop testing of the physical characteristics and durability of the Dornier Axis single-use ureteroscope. We performed bench-top optical testing as well and compared it with the current generation LithoVue scope.
Materials and Methods
An Internal Review Board waiver was provided for this study. Ten new, never-used, Dornier Axis ureteroscopes were assessed for physical, functional, and optical performance. The scope shaft, flow channel, and working channel lengths were measured. Flexion was assessed for maximal tip deflection upward and downward and with insertion of a 200 μm Flexiva™ (Boston Scientific, Marlborough, MA), 200 μm and 365 μm Moses™ laser fibers (Lumenis, Yokneam, Israel), and a 1.9F Zero Tip™ nitinol basket (Boston Scientific, Marlborough, MA) in the working channel. Irrigation flow rate with an empty working channel and insertion of the same instruments was measured by using the Thermedx® FluidSmart® (Thermedx LLC, Solon, OH) Fluid Management System with inflow pressure set at 100 mm Hg with 0.9% normal saline. Flow into a graduated cylinder was measured after 30 seconds and normalized to a rate in milliliters per second. For each flow rate measured, the system was allowed to equilibrate for 30 seconds before measuring the flow rate. All ureteroscopes were then fully deflected 100 times in each direction without any instruments in the working channel (200 total flexions), and maximal deflection angles upward and downward were re-measured with the same working instruments. All measurements were repeated in duplicate.
In vitro optical testing was then performed for both Dornier Axis and Boston Scientific LithoVue ureteroscopes. Resolution testing was performed with a 1951 United States Air Force (USAF) test pattern card (Edmund Optics, Barrington, NJ) at 3, 5, 10, 20, and 50 mm. Testing was completed by using the manufacturers' respective proprietary monitors within an opaque box in a dark room to remove ambient light. Distortion was measured with a multi-frequency grid distortion target where: Distortion = (Actual distance − Theoretical distance)/Theoretical distance × 100. Depth of field was determined by using the Edmund Optics depth of field test target.
Normality of data was assessed with the Shapiro–Wilk test. Statistical analyses using paired Wilcoxon rank-sum tests and Kruskal–Wallis multiple-group comparison tests were performed in R version 3.6.1 (R Core Team, 2019) and reported as “median [interquartile range].” Threshold for significance was set at p < 0.05.
Results
The Dornier Axis scope shaft, flow channel, and working channel length were 65.7 ± 0.05, 78.6 ± 0.09, and 93.0 ± 0.1 cm, respectively. A full ureteroscope is shown in Figure 1. The Dornier Axis produced flexion >300° in both directions while empty and with instruments in the channel, except for the 365 μm fiber (Table 1 and Fig. 2). After 200 total deflections, there were slight decreases in upward flexion with an empty channel, upward flexion with a 200 μm Moses fiber, and downward flexion with a 200 μm Flexiva fiber (all 2% or less of median pre-cycling deflection). There were no other significant differences in maximum deflection. No scope failures were observed during flexion testing. Representative flexion is shown in Figure 1. On Kruskal–Wallis multiple-group comparison testing, there was a statistically significant difference between flexion with an empty channel and with instruments inserted (downward deflection pre-cycle p = 0.001, post-cycle p = 0.012). The most notable difference was using the 365 μm fiber. Excluding the 365 μm fiber, there was a <10° difference among the medians of the remaining groups and there was no statistically significant difference among the empty channel and remaining channel tools in flexion before and after cycling. Detailed results are shown in Table 1.
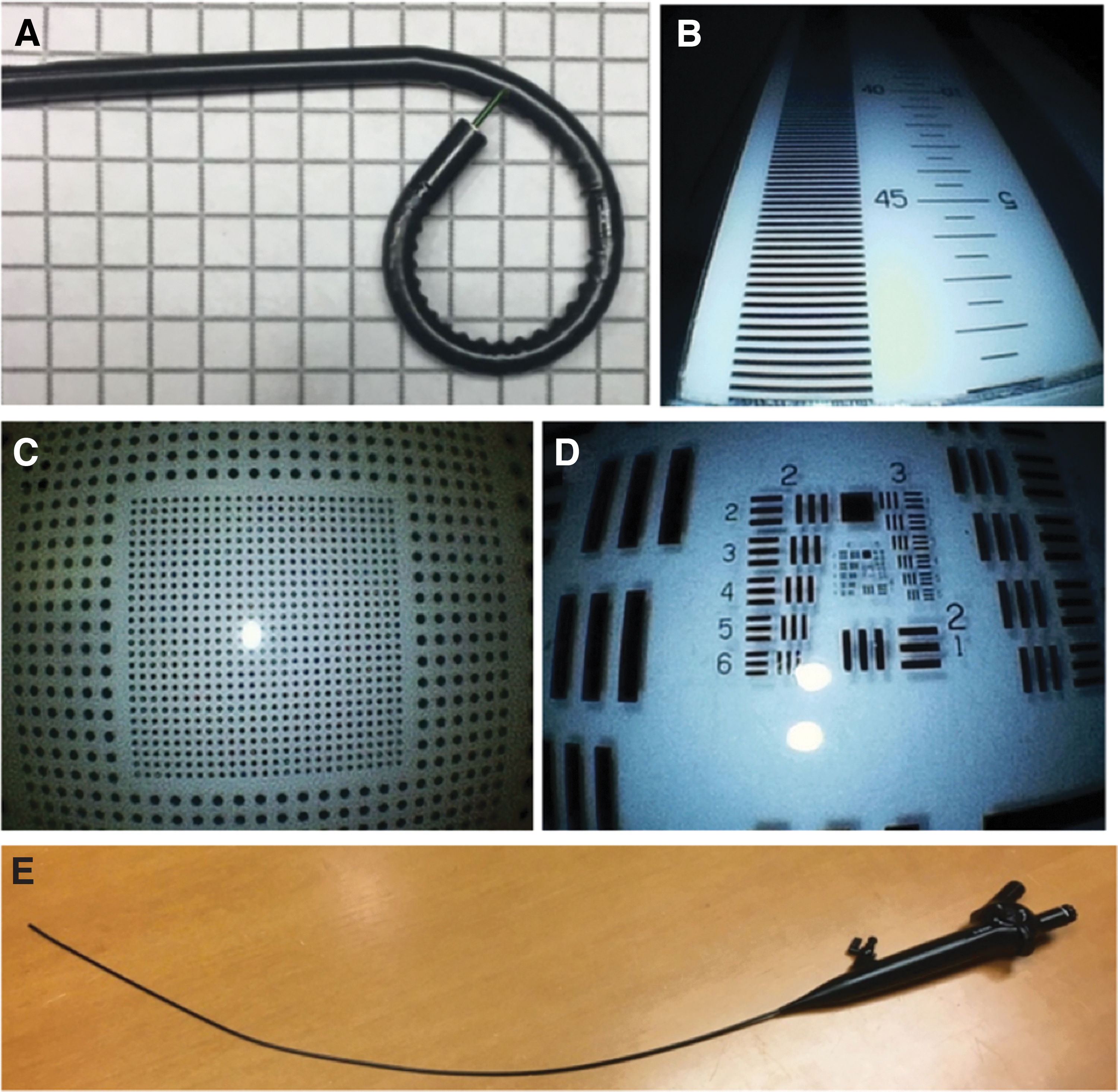

Dornier Axis median (interquartile range) downward flexion with pre- and post-cycling testing. micrometer (μm); French (F). Color images are available online.
Pre- and Post-cycling Upward and Downward Average Flexion of Dornier Axis Single-use Ureteroscopes
Flow rate with various working channel instruments before flexion cycling.
p < 0.05.
IQR = interquartile range.
The irrigation flow rate was highest with an empty channel and decreased with introduction of various instruments through the channel. The 1.9F basket was observed to have the largest negative impact on flow (Table 1).
The Dornier Axis demonstrated superior resolution at all measured distances compared with the LithoVue (Table 2 and Fig. 3). In addition, the Axis had less distortion compared with the LithoVue (−6.7% [(−9.6%)–(−2.7%)] vs −20.9% [(−22.4%)–(−10.6%)], p = 0.028). There was significant difference in the depth of field that favored the LithoVue (Axis vs LithoVue 4.5 [4.3–4.5] vs 5.0 [5.0–5.0] cm at 15 line-pairs/mm, p = 0.014). Representative optical testing images are shown in Figure 1.
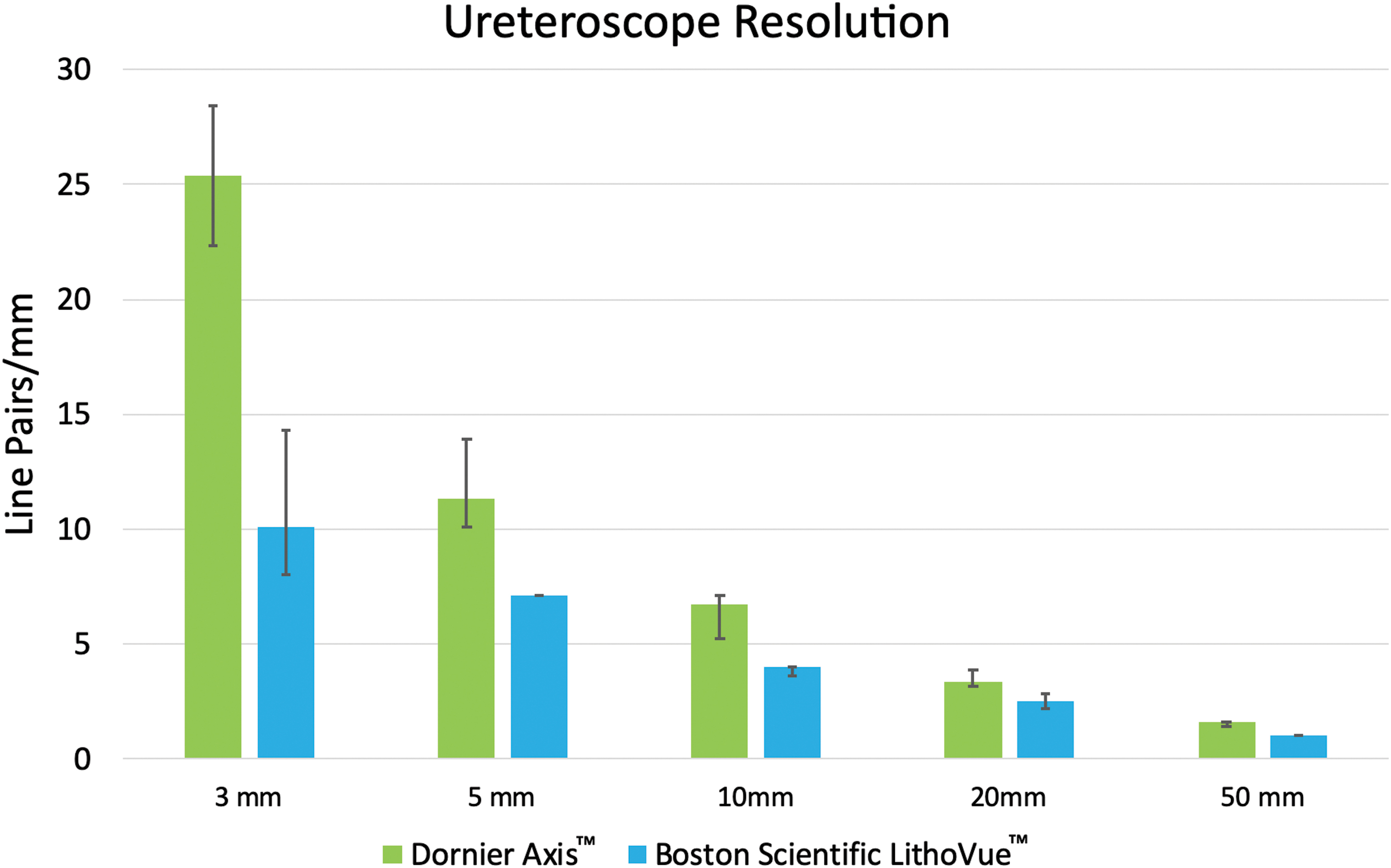
Optical resolution comparison between Dornier Axis and Boston Scientific LithoVue™ single-use ureteroscope. Median (interquartile range) line-pairs per millimeter p < 0.05 for all tested distances. Color images are available online.
Single-Use Ureteroscope Optical Resolution Comparison
Discussion
Incorporation of single-use ureteroscopes into the practice of urology continues to increase, and device manufacturers correspondingly continue to bring new models to market. 14,16 Scope consistency and durability are crucial factors in the decision to use single-use scopes or not. To our knowledge, this is the first benchtop or clinical testing completed for the Dornier Axis single-use ureteroscope.
The Dornier Axis scope demonstrated excellent flexion capability, with >300° of flexion achieved in either direction with or without an empty working channel. This measured value, in fact, exceeds the manufacturer's claim of 275°, 17 and it also exceeds the flexion measurements obtained during prior benchtop testing of several other bi-directional single-use and reusable ureteroscopes. 11 The Axis also demonstrated impressive durability, with no scope failure after 200 total flexions. There was a minimal statistically significant decrease in flexion with the empty channel, Flexiva 200 μm and Moses 200 μm laser fibers (all 2% or less). The clinical impact of this is likely insignificant. Except for the 365 μm laser fiber, the Dornier Axis retained >300° flexion with instruments in the working channel. After eliminating the 365 μm laser fiber, there was no difference among flexion in the working channels pre- or post-cycling using Kruskal–Wallis multiple-group comparison testing. We have previously reported benchtop of single-use ureteroscopes (LithoVue and PU3022a; Zhuhai PUSEN Medical Technology, Guangdong, China) with a similar experimental design. In that study, maximum flexion of the LithoVue was 291.1° ± 6.1° and that of the PU3022a was 280.3° ± 6.6°. The Axis demonstrates greater flexion with all tested instruments compared with our prior testing, although statistical conclusions cannot be drawn. The LithoVue and PU3022a decreased to 257.8° ± 9.5° and 253.4° ± 15.8° after 200 cycles of deflection. They were noted to lose 3% to 5% of their maximal deflection with instruments in the channel before flexion testing. 18 Ideally, incorporation of flexion with a 272 μm laser fiber would have also been completed. However, this was not available for this study. We suspect that the flexion of a 272 μm fiber would likely lie between the flexion observed for the 200 and 365 μm fibers, although exactly where it would fall is unknown. The flow rate decreased as expected with increasing instrument caliber within the working channel, and these results appear consistent with those found by others in previous studies when matched for specific working channel instruments. 11,18 –20
Of particular clinical relevance is the optical performance demonstrated by the Axis, which surpassed that of the LithoVue with both greater resolution and less image distortion. These findings are consistent with the Axis manufacturer's claim that its complementary metal oxide semiconductor (CMOS) imaging chip possesses 160,000 pixel-sensors compared with ∼62,000 sensors in the LithoVue CMOS chip. Given that the LithoVue's optics and resolving power have been found to be at least comparable, if not superior, to many other single-use and reusable ureteroscopes across numerous prior studies, 19 –21 the results of our testing indicate that the Axis also compares favorably with re-usable flexible ureteroscopes. Notably absent from our testing herein, however, was the presence of an aqueous or blood-tinged fluid environment. Color checked card testing was felt to be limited without a blood-tinged fluid environment. Blood tinged urine, as is often encountered during complex upper tract endoscopy, is a well-known struggle point in URS, and at least one prior observational study of experienced ureteroscopists identified that the LithoVue specifically could be problematic in cases with hematuria. 22 The authors claimed that this issue could be attributable to differences between the CMOS imaging chip present in the LithoVue and the charge-coupled device imaging chip present in many reusable digital ureteroscopes. Specifically, CMOS chips are known to be more sensitive to red color, which negatively affected subsequent steps of light and color balancing required to produce the eventual live image. It remains to be seen whether this issue with red color processing will persist as other CMOS-equipped single-use ureteroscopes, including the Axis, continue to enter the market. The LithoVue did demonstrate a better depth of field; however, the clinical meaning of this remains unknown, as the difference was small. Similar to the ability to visualize in hematuria, should the Axis have reports of difficulty with field depth, this would require further study.
Although each individual health care system, hospital, and practice are unique, health care expenditure will continue to be scrutinized to obtain maximal cost efficiency. 5 Prior studies have been mixed about the cost-effectiveness of single-use vs reusable ureteroscopes. 5,23,24 One analysis showed that single-use ureteroscopes are financially favorable when performing fewer than 100 ureteroscopic procedures per year. 7 However, at very high-volume centers, single-use ureteroscopes avoid the reprocessing time and potential time delays associated with reusable ureteroscopes. 24 There may be other scenarios where the availability of a single-use ureteroscope is favorable, such as a history of highly multidrug-resistant bacteria or anatomy that requires significant torqueing or turning of the device that is more likely to result in damage and repair costs. 24 Ultimately, the determination of cost-effectiveness is highly complex and health system-specific.
This study was a benchtop study and, therefore, has limitations in the clinical conclusions that can be drawn from it. Specifically, the scopes were flexed in free space rather than torqued against resistance in a tight collecting system, they were not tested in an aqueous or bloody environment, and lasers were not used; we, therefore, cannot conclude how those conditions may affect Axis function. Similarly, isolated torque testing was not performed, as it was felt that the flexion and torque testing could not be independently tested without compromising the results of the other. In addition, we did not perform testing to any current reusable ureteroscopes. This is, in part, due to the limited ability to access a brand new reusable ureteroscope to complete flexion testing and due to the limited ability to obtain several clinical ureteroscopes to complete appropriate statistical analysis of optical testing. It would have been ideal to test the LithoVue flexion in this exact design. However, prior benchtop testing of the LithoVue by our group has been published. 11,18 Lastly, since it is a relatively new-to-market product, we do not have access to costing data and, therefore, no reasonable economic analysis was performed. Nonetheless, it appears that the Dornier Axis is a viable new single-use ureteroscope with excellent functional and optical performance. Further clinical use, testing, and economic analysis are warranted to evaluate their incorporation into the URS market.
Conclusions
The Dornier Axis is a new single-use disposable ureteroscope that demonstrates excellent benchtop flexion capability and durability. It demonstrates superior benchtop optical resolution compared with the LithoVue. Further study in a clinical environment is warranted.
Footnotes
Authors' Contributions
P.W., R.S.T., and R.Q. contributed to project design, testing, statistical analysis, and article writing and editing. B.K. contributed to article writing and editing. G.M.P. and M.E.L. contributed to project design, article writing and editing.
Author Disclosure Statement
G.M.P. and M.E.L. serve as consultants for Boston Scientific. P.W., R.S.T., R.Q., and B.K. have no conflicts of interest to disclose.
Funding Information
Dornier provided the single-use Dornier Axis™ ureteroscopes and optical box for this study.