
Abstract
Introduction:
Elevated intrarenal pressure (IRP) during flexible ureterorenoscopy (FURS) is a predictor of postoperative complications. The aim of this study is to evaluate IRP during FURS in a porcine kidney model to determine the safest combination of irrigation device, ureteral access sheath (UAS), and ureteroscope.
Methods:
Urinary tracts were harvested from Landrace pigs slaughtered for the food chain. Two flexible ureteroscopes, 8.7F and 9.5F, were evaluated. Irrigation systems evaluated included the following: TraxerFlow™ (Rocamed, France), SAPS™ single action pumping system (Boston Scientific), Pathfinder Plus™ (Utah Medical), and a manual “bag squeeze.” This experiment was conducted with no UAS, followed by an 11/13F UAS and then a 12/14F UAS. IRPs were measured in the prepared porcine kidney during all possible combinations of scope, UAS, and irrigation system.
Results:
Pressures were significantly reduced when using 12/14F UAS compared with 11/13F UAS (16.45 ± 5.3 cmH2O vs 32.73 ± 35.66 cmH2O, p = 0.006), and when using 11/13F UAS compared with no UAS (32.73 ± 35.66 cmH2O vs 49.5 ± 29.36 cmH2O, p = 0.02). Pressures were significantly reduced with the 8.7F scope compared with the 9.5F scope (24.1 ± 21.24 cmH2O vs 41.68 ± 34.5 cmH2O, p = 0.001). SAPS generates significantly greater IRP than TraxerFlow, Pathfinder Plus, and a “bag squeeze” (p < 0.05). The most dangerous combination was using the SAPS, no UAS, and larger ureteroscope leading to an IRP of 100.6 ± 16.1 cmH2O. The safest combination was using Pathfinder Plus with a 12/14F UAS and smaller ureteroscope giving an IRP of 11.6 ± 3.65 cmH2O.
Conclusion:
IRPs are reduced by selecting larger UAS and a small ureteroscope. The SAPS generates significantly higher IRPs than other irrigation systems. To maintain safe IRPs during FURS, urologists should use large UAS, narrow ureteroscopes, and be cautious in the selection of an irrigation device.
Introduction
Technology is rapidly advancing in the surgical management of urinary tract calculi. The management options for renal and proximal ureteral calculi are flexible ureterorenoscopy (FURS), percutaneous nephrolithotomy (PCNL), and extracorporeal shockwave lithotripsy (SWL). 1,2 Typically, PCNL has been the treatment preference for larger calculi, but recent advances in FURS technology have led to it being utilized more frequently for larger stones. 3 –5 FURS has a shorter hospital stay and less complications, which often makes it a popular choice among urologists. 3 FURS procedures for urolithiasis have been increasing on a yearly basis over the past decade, while SWL and PCNL has decreased. 5
Elevated intrarenal pressure (IRP) during FURS is a predictor of postoperative complications such as infection and kidney injury. 6 The resting IRP in an unobstructed kidney is 0 to 2 cmH2O. 7 As IRPs increase, there are a variety of complications that may occur. Kidney injury and reduced arterial blood flow can occur at an IRP of 20 to 40 cmH2O. 8 IRPs of 40.8 to 47.6 cmH2O can cause pyelovenous backflow, 9 and forniceal rupture will occur at 81.6 to 95.2 cmH2O. 10
The variables in FURS that potentially may affect IRP are as follows: ureteroscope diameter, ureteral access sheath (UAS) diameter, and type of irrigation system. Larger diameter UASs reduce IRP while improving flow. 11 There are now a wide range of newly developed irrigation systems available for FURS to improve flow and vision. It has been shown that extremely high IRPs can be generated with some of these irrigation systems in a kidney bench model. 12 There is a lack of data on the ideal combination of ureteroscope, UAS, and irrigation system required to maintain safe IRP. The aim of this study is to evaluate IRPs in an ex vivo porcine kidney model using various combinations of ureteroscope, UAS, and irrigation system to determine the safest combination.
Methods
Porcine kidney preparation
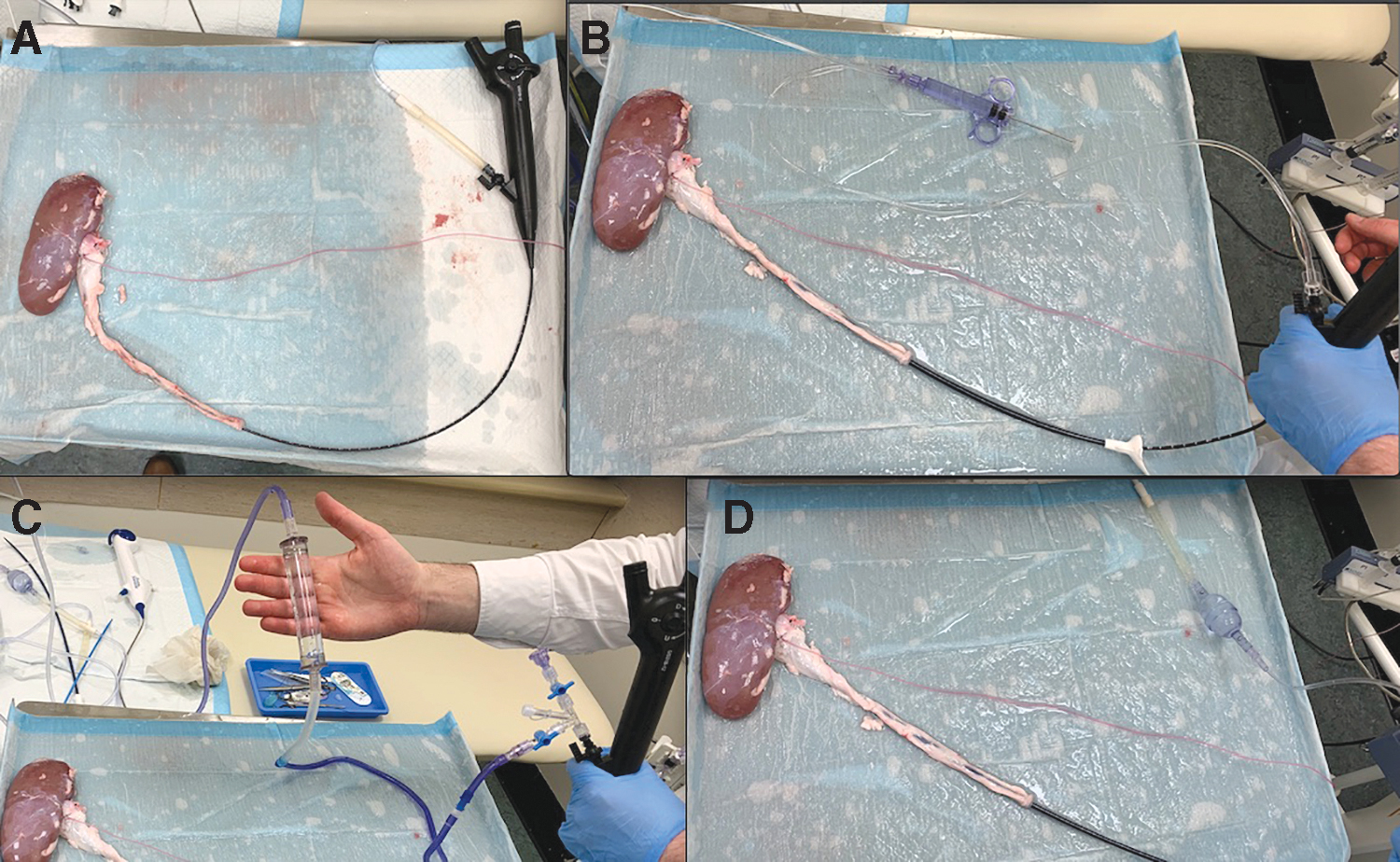
Two entire intact urinary tracts were harvested from a Landrace pig that had been slaughtered for the food chain by a licensed veterinarian. The organs were harvested within 4 hours of the animal's death and within 6 hours of experimentation. In preparation of the testing, Gerota's fascia was dissected from the kidney and the ureter was trisected at the level of the bladder. A 5F cystometry pressure transducer was inserted directly into the renal pelvis via a small incision and then sutured in place to ensure that a water-tight seal was achieved (Fig. 1A). IRPs were recorded with a urodynamic machine with all measurements calibrated to atmospheric pressure.
Devices examined
Two different sized single-use flexible ureteroscopes were evaluated; the LithoVue™ (Boston Scientific), which has a 9.5F diameter, and the Innovex (Innovex Medical Co, China), which has an 8.7F diameter.
Two different sized UASs were evaluated: the Navigator™ (Boston Scientific) 11/13F sheath, and the Flexor® Parallel™ (Cook) 12/14F sheath.
Irrigation systems evaluated included the following: TraxerFlow™ (Rocamed, France) (Fig. 1C), SAPS™ single action pumping system (Boston Scientific) (Fig. 1B), Pathfinder Plus™ (Utah Medical) (Fig. 1D), and a manual “bag squeeze” by the same participant through the experiment. These systems were selected to evaluate a broad range of irrigation device design concepts in the study such as a large chamber system, small chamber system, and syringe-based system.
Experiment protocol
For each experiment, the tip of the ureteroscope was placed in the renal pelvis to standardise pressure measurements throughout the experiments. The tip of the UAS (if used) was placed at the pelviureteric junction, as shown in Figure 1. The irrigation bag was kept at a height of 100 cm above the kidney. The working channel of the ureteroscope was unoccupied during the experiment. The irrigation system was operated by the same surgeon (E.M.C.) throughout the experiments except for the manual bag squeeze, which was conducted by an assistant (M.E.). An “activation” of each device involved one brisk squeeze of the chamber or pushing the syringe until the full capacity of the chamber/syringe was emptied (TraxerFlow 30cc, SAPS 10cc, Pathfinder Plus 20cc).
Each experiment involved five activations of each irrigation system. The maximum IRP reached with each of the five activations was recorded. The IRP was allowed time to plateau before the next activation. After five activations, a mean ± standard deviation for that experiment was calculated. This whole process was conducted with no UAS, followed by the 11/13F UAS and then 12/14F UAS. The whole process was then repeated with the other ureteroscope. This resulted in 120 total activations/measurements. The first porcine kidney was replaced after 60 activations to minimize the risk of repeated trauma leading to false results. This resulted in mean IRPs for all possible combinations of irrigation system, UAS, and ureteroscope.
Statistical analysis
Numerical data are presented as mean ± standard deviation. Categorical data are given as numbers and percentages. Statistical analysis was performed using one-way ANOVA (SPSS 26.0 for Mac). We considered a p-value of <0.05 to be statistically significant.
Results
The greatest IRPs were generated with the SAPS followed by TraxerFlow, Pathfinder Plus, and then “bag squeeze” (Table 1). The most dangerous combination was using the SAPS, no UAS, and 9.5F ureteroscope, leading to an IRP of 100.6 ± 16.1 cmH2O. The safest combination was using “bag squeeze,” 12/14F UAS, and a 8.7F ureteroscope, which resulted in an IRP of 11.6 ± 2.1 cmH2O, or by using Pathfinder Plus with a 12/14F UAS and 8.7F ureteroscope giving an IRP of 11.6 ± 3.65 cmH2O. Pressures reached the threshold for forniceal rupture (>81.6 cmH2O 10 ) when the SAPS was used with no UAS or with the 11/13F UAS. Pressures reached the threshold for pyelovenous backflow (>40.8 cmH2O 9 ) when the Pathfinder Plus was used with no UAS, or when the TraxerFlow was used with no UAS or the 11/13F UAS.
Maximum Intrarenal Pressures (cmH2O) Generated with Each Irrigation System
Data are presented as mean ± standard deviation.
Italic values indicate pressures capable of causing pyelovenous backflow.
Bold values indicate pressures capable of causing forniceal rupture.
UAS = ureteral access sheath.
UAS vs no UAS
Pressures were significantly reduced when using 12/14F UAS compared with 11/13F UAS (16.45 ± 5.3 cmH2O vs 32.73 ± 35.66 cmH2O, p = 0.006) and when using 11/13F UAS compared with no UAS (32.73 ± 35.66 cmH2O vs 49.5 ± 29.36 cmH2O, p = 0.02). These findings are illustrated in Table 2.
Comparison of Maximum Intrarenal Pressures (cmH2O) Generated According to Ureteral Access Sheath and Ureteroscope Selection
Data are presented as mean ± standard deviation.
p-Values in bold indicate statistical significance.
Large ureteroscope vs small ureteroscope
Pressures were significantly greater with the 9.5F scope compared with the 8.7F scope (41.68 ± 34.5 cmH2O vs 24.1 ± 21.24 cmH2O, p = 0.001). These findings are illustrated in Table 2.
SAPS vs Pathfinder Plus
Using no UAS, the SAPS created significantly higher pressure than Pathfinder Plus with either the 8.7F scope (p = 0.04) or the 9.5F scope (p < 0.0001) (Table 3). Using the 11/13F UAS, the SAPS created significantly higher pressure with either the 8.7F scope (p < 0.0001) or the 9.5F scope (p = 0.02). Using the 12/14F UAS, the SAPS created significantly higher pressure with either the 8.7F scope (p = 0.02) or the 9.5F scope (p < 0.0001).
Comparison of Intrarenal Pressures (cmH2O) Generated by SAPS vs Pathfinder Plus, SAPS vs TraxerFlow, and TraxerFlow vs Pathfinder Plus
Data are presented as mean ± standard deviation.
p-Values in bold indicate statistical significance.
SAPS vs TraxerFlow
While using no UAS, the SAPS created significantly higher pressure than TraxerFlow with either the 8.7F scope (p = 0.02) or the 9.5F scope (p < 0.0001) (Table 3). While using the 11/13F UAS, the SAPS created significantly higher pressure than TraxerFlow with the 8.7F scope (p < 0.0001), but no difference was noted when using the 9.5F scope. While using the 12/14F UAS, the SAPS created significantly higher pressure than TraxerFlow with either the 8.7F scope (p = 0.04) or the 9.5F scope (p < 0.0001).
TraxerFlow vs Pathfinder Plus
In general, there was no significant difference between TraxerFlow and Pathfinder Plus, as illustrated in Table 3, except when using no UAS +8.7F scope, and 11/13F UAS +9.5F scope. In these two scenarios, the TraxerFlow generated higher pressures (p = 0.04, p < 0.0001).
Bag squeeze vs other systems
Bag squeeze generated lower pressures than the other three irrigation systems (Table 4). The difference was statistically significant except when comparing bag squeeze with the Pathfinder Plus with the 9.5F scope. There was no difference between these two irrigation methods regardless of UAS.
Comparison of Intrarenal Pressures (cmH2O) Generated by Manual “Bag Squeeze” and Other Irrigation Systems
Data are presented as mean ± standard deviation.
p-Values in bold indicate statistical significance.
IRP = intrarenal pressure.
Discussion
Currently, a variety of technologies for FURS are evolving to improve vision for surgeons. Elevated IRP is a predictor of postoperative complications after FURS. 6 There are no clear guidelines for urologists to select the optimum equipment to obtain satisfactory vision without increasing morbidity. There are three main findings in this study. The first is that the safest combination for FURS favors using a large UAS, narrow ureteroscope, and the Pathfinder Plus or a “bag squeeze” for irrigation. The second finding is that SAPS causes significantly greater IRPs than both TraxerFlow and Pathfinder Plus systems, and is capable of reaching pressures capable of forniceal rupture 10 when used with a small UAS or no UAS. The third finding is that IRPs are significantly reduced by using smaller ureteroscopes and larger UAS. These are important considerations for urologists that may change existing practices.
There are limited data in the literature comparing contemporary irrigation systems for FURS and there is no advice in the EAU guidelines regarding the safest combination of UAS, ureteroscope, and irrigation device. 1 Proietti and colleagues evaluated SAPS, TraxerFlow, and a number of other similar devices in an artificial kidney model. They noted higher pressures with SAPS compared with TraxerFlow when the working channel of the scope was empty and closed. 12 These findings are similar to our study. Our study adds to these findings as we conducted our study in a porcine kidney rather than an artificial bench model. Proietti and coworkers also conducted their study with a 10/12F access sheath. 12 We have added to this research by evaluating three other scenarios: no UAS, 11/13F UAS, and 12/14F UAS. We also found that manual “bag squeeze” generates significantly lower pressure than the irrigation systems assessed. Previous studies have unsurprisingly shown that manual compression of the irrigation bag produces inconsistent and unreliable results with regard to changes in pressure. 13 We did note that using a smaller scope led to safer pressures. Sener and colleagues also recommended that smaller ureteroscopes be used to reduce IRPs during FURS. 14 The range of IRPs in our study was 11.6 to 100.6 cmH2O, which is similar to the range 40.8 to 199.35 cmH2O reported in a review by Tokas and colleagues. 15
A secondary finding of this study is that pressures were significantly reduced when using 12/14F UAS compared with 11/13F UAS and when using 11/13F UAS compared with no UAS. A similar study noted reduced IRPs in a porcine kidney when comparing 12/14F UAS with 10/12F UAS. 11 Rehman and colleagues evaluated the effect of UAS on IRP in human cadaveric kidneys and had similar findings to our study. They also noted that the reduction in IRP did not improve any further with UAS larger than 12/14F. 16 We chose not to evaluate any UAS larger than 12/14F as we do not commonly use them in our practice. Studies have shown that using a UAS improves vision by establishing a continuous outflow, reduces IRP, and reduces operating duration. 17,18 Although we have shown a clear benefit in this study in using a UAS, urologists must be cognizant of the risk of ureteral damage. 19
A limitation of the present study is that we did not assess the effects of these irrigation systems on intraoperative visual quality. We have provided urologists with important data on how to select the safest equipment for FURS, however, we cannot comment on the visual quality that would result from this selection. For example, in this study, we recommend caution if using the SAPS, but it has been shown to be the most effective irrigation device in terms of vision. 20 Another limitation is that there may be variations in the force applied by the main operator with each device. This is particularly true during a manual “bag squeeze.” We attempted to minimize this confounder by using the same surgeon (E.M.C.) for all tests. IRPs recorded during FURS in cadaveric porcine kidneys are higher than in live anesthetized pig kidneys 21 possibly due to loss of elasticity after death. Despite this, we feel that the pressures recorded in the present study are not an overestimation of the dangerous levels which can be generated during FURS. A recent study continuously monitoring IRP during FURS in humans noted pressures ranging from 289.3 to 436.9 cmH2O. 22 These findings are similar to our study and should prompt urologists to exercise caution during retrograde intrarenal surgery. Our study was conducted with an unoccupied ureteroscope working channel, which is a possible limitation. IRPs are reduced when the working channel is occupied. 12 The majority of operative time during an FURS is spent with the working channel occupied, and therefore, one could argue that our study overestimates the true intraoperative pressures.
This is the first study of its kind to provide urologists with clear guidelines for FURS equipment selection to minimize morbidity. 6 We have developed a novel “quick reference” table (Table 1) that urologists and trainees may refer to when planning surgery, which contains a “traffic light” system of pressures. This tool may lead to changes in everyday practice that would reduce patient morbidity.
Conclusion
Irrigation systems used during FURS are capable of generating dangerously high IRPs. The SAPS generates significantly higher IRPs than other irrigation systems, and the Pathfinder Plus appears to be the safest irrigation system. IRPs can be significantly reduced by using narrow ureteroscopes and large UAS. To maintain safe IRPs during FURS, urologists should use large UAS, narrow ureteroscopes, and be cautious in the selection of an irrigation device.
Footnotes
Ethics Statement
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional research committee and with the 1975 Helsinki Declaration and its later amendments or comparable ethical standards.
Acknowledgments
The authors wish to acknowledge Colette Hales (Theatre Nurse, Mercy University Hospital), Michael O'Leary (Veterinarian, Department of Agriculture) and Staunton Foods for their contributions to this study.
Authors' Contribution
E.M.C.: article writing; L.C.Y.: data collection and article writing; M.E.: data collection; K.P.: data collection; C.M.B.: project development; D.B.H.: project development and article writing.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received.