
Abstract
Background:
To create and evaluate a realistic, anatomically accurate, and user-friendly bladder phantom for reproducible endourological training purposes and endoscope mastery.
Materials and Methods:
The anatomy of full bladders was mapped from human computed tomography datasets. After a 3D model development process, content evidence and response process evidence (RPE) of the phantom were evaluated using the system usability scale (SUS), 5-point Likert scale questionnaires, and task execution of experienced urologists (U) and endoscopy-naive medical students (MS) in two training sessions (first vs second). Required validation cohort sizes (1:10) of the evaluating urologists (n = 12) and students (n = 115) were precalculated. Time measurements were recorded. Students were additionally evaluated by a validated global psychomotor assessment score (GPSS). Group comparisons were calculated by the Mann–Whitney U test. All tests were two sided with p < 0.05 considered statistically significant.
Results:
Content evidence was assessed by urologists with an “excellent” SUS score of 89.4 ± 5.9 and an average “agreement” of ≥4 pts in the Likert scale questionnaires. RPE was assessed by intra- and intergroup time comparison for the execution of endoscopic tasks (cystoscopy [CY], guidewire insertion, and tumor biopsy). For CY, U: first 17.6 ± 4.4 seconds vs second 12.4 ± 2.0 seconds, p = 0.002; MS: first 56.6 ± 28.2 seconds vs second 28.6 ± 14.7 seconds, p < 0.001; U vs MS: first U 17.6 ± 4.4 seconds vs first MS 56.6 ± 28.2 seconds, p < 0.001, second U 12.4 ± 2.0 seconds vs second MS 28.6 ± 14.7 seconds, p < 0.001. Significant time differences were documented for all tasks and sessions (p < 0.001). Additionally, significant GPSS differences were recorded between the sessions (GPSS: first 20.4 ± 5.1 pts vs second 24.7 ± 4.0 pts, p < 0.001).
Conclusions:
Our low-fidelity 3D-printed bladder, called BladCap, is an easy-to-assemble, inexpensive, and robust phantom. We present data, which establish construct validity to support use as a clinical training device.
Introduction
Cystoscopy (CY) is the key clinical technology for diagnosis and follow-up of numerous urological diseases, including bladder cancer. 1 At the same time, CY is the main technique for many endourological tasks, such as biopsies or guidewire insertion (GWI) for subsequent retrograde upper urinary tract interventions. 2 Mastery and internalization of these challenging tasks are thus the foundation for endourological training. However, the hand-eye coordination for the visualization of the entire bladder surface as well as the necessary blind control of the different working channels of the endoscope can confront beginners with difficulties that could potentially be overcome by enhanced skills training.
There is an interdisciplinary surgical consensus that, for reasons of patient safety, the initial training of a surgical procedure should not be performed on the patient to create an environment in which one can intentionally learn from one's own mistakes. 3 This maxim is very true for CY as the patients are usually awake during this procedure and inaccurate CY execution can increase transoperative pain and the risk of hematuria. 3
However, it is not only physicians in training who can benefit from ex vivo models, but also experienced urologists (U) can practice an innovative endoscopic technology on a model before its first clinical implementation. In addition, organ phantoms can be used in student education. In urology, the opportunity for medical students (MS) to perform endourological procedures on phantoms could arouse interest in the specialty and strengthen the understanding of endourology for potential residents. 4
Urological training devices have been evaluated in the past, mainly focusing on transurethral resection or ureterorenoscopy. 5 A valid overview of the available urological 3D-printed phantoms is given in a recently published review. 6 However, of 22 publications of phantoms intended for use in teaching, most are kidney and adrenal gland (14) or prostate (5) models. Only three studies focus on the urinary tract, of which only one phantom is additionally equipped with a bladder. A high-fidelity 3D model of the TURBT was presented by the University of Rochester. 7 However, an acquisition does not seem possible at the moment. Drawbacks of the existing models include poor availability and limited standardization for their respective validation. Furthermore, some models differ substantially from genuine bladder anatomy, whereas others are good representations but have high acquisition costs. Finally, some models are only virtual representations. For these reasons, an expansive application of current bladder models seems unlikely. 8 The aim of this study was therefore to develop and evaluate a cost-effective, anatomically accurate, and user-friendly 3D-printed bladder phantom to train basic endourological skills under intervention-like conditions.
Materials and Methods
This study was performed in adherence to the Declaration of Helsinki, and all patients gave approval to participate in this study. Additionally, approval of the Institutional Ethics Review Board (Ethics Committee II, University of Heidelberg, Germany, Reference No. 2015-459N-MA) was obtained. The participation of the students was voluntary and unpaid.
BladCap phantom development
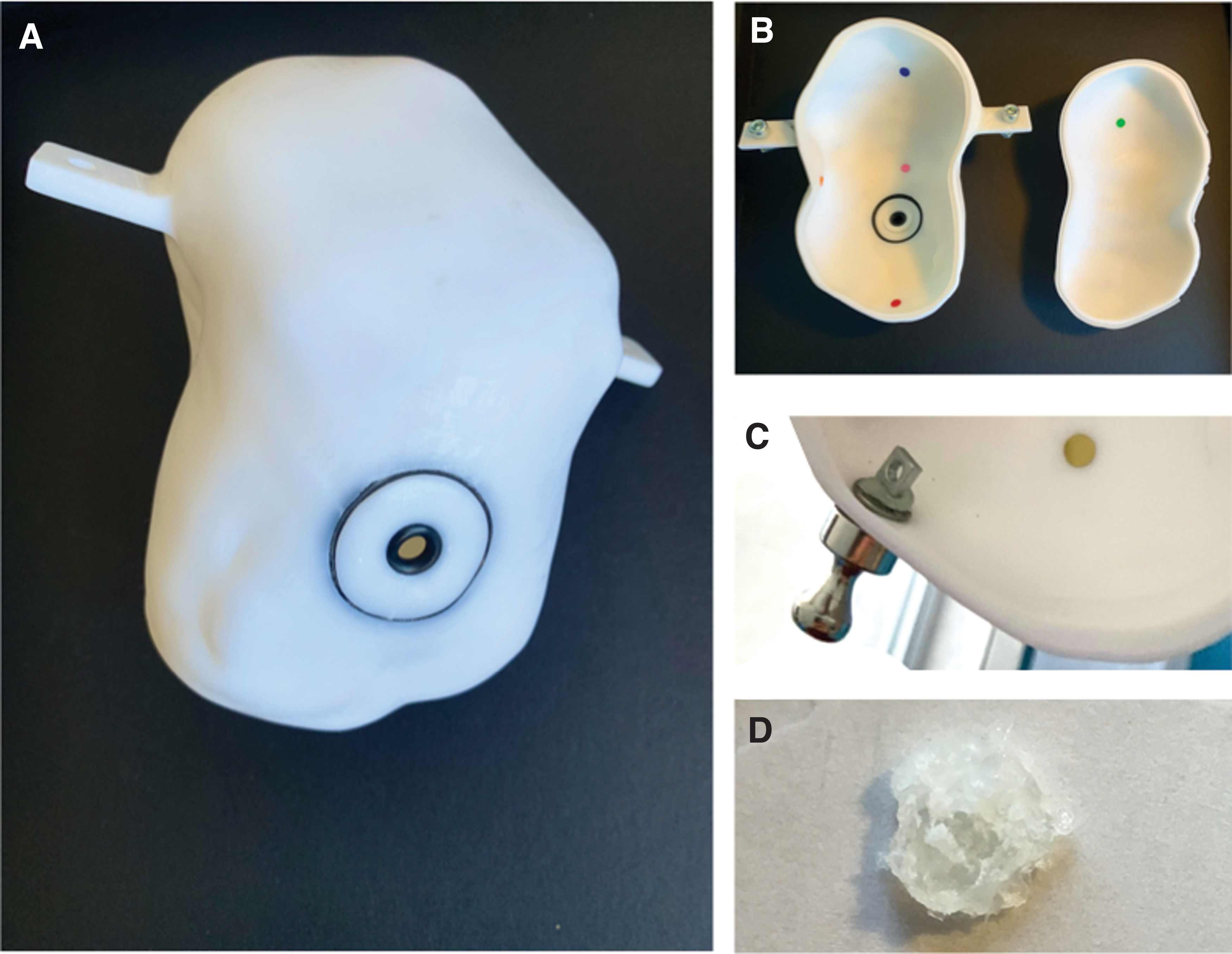
After segmenting full patient bladders from high-resolution computed tomography datasets, stereolithography (SL) files were extracted. A subsequent 3D reconstruction was performed using 3D Builder and SolidWorks® software (Dassault Systems, Waltham, MA). Following extensive testing with 3D plaster printing, polymer was chosen as the basic material for the phantom due to its durable properties. The bladder phantoms were then printed by SL laser using a FormLabs® 2 printer (Formlabs, Inc., Somerville, MA) and suspended from a metallic framework. For endoscopic exploration, the phantoms were further customized to enable standardized performance of the surgical tasks described below. For this reason, seven bladder regions (trigone, posterior wall, left and right wall, dome, anterior wall, and bladder neck) were marked with colored spots (Fig. 1B) to allow monitoring of the completeness of a performed CY. Moreover, two different sizes of sham ureteral orifices were introduced, which were suspended from a metal disc so that they could be moved by external magnets (Fig. 1C). Sham orifice allowed GWI training or ureteric catheter manipulation and intubations. Sham bladder tumors (ethylene-vinyl acetate) were also fixed to an externally movable metal disk by a hot glue gun and served as a biopsy model (Fig. 1D).
BladCap evaluation
In recent years, the criteria to evaluate surgical simulators have changed from the description of validity types (i.e., face, content, construct validity) to a consideration of the entire interventional curriculum, the ability of the trainer to differentiate between skill levels and the transfer of skills from simulation to surgery. 9 However, the use of this framework for validity is lacking in the surgical education literature, 10 especially in urology. Many studies on urological simulators refer to a description of validity types. 5 By the presentation below, we have tried to provide an appropriate illustration of the outdated and newer validation criteria to enable a comparison with current studies. The phantom was evaluated for content evidence (expert consensus on realism [ECR] and suitability for training, previous face and content validity) and response process evidence (RPE; previous construct validity, ability of a simulator to distinguish between different levels of experience within a group, over time, and between several groups with different levels of experience) by urologists (board-certified urologists and residents) and MS with a rigid, 17F. cystoscope in white light CY.
ECR (previously face validity)
ECR was assessed by urologists performing the endoscopic tasks on BladCap, as described below. After completion, an extensive evaluation was carried out with Likert-type-based questionnaires, which were used to calculate the system usability scale (SUS) 11 score (Supplementary Table S1). The SUS is based on a 10-item questionnaire, consisting of 5 positive and 5 negative affirmations. For evaluation 5 points are subtracted from the sum of positive answers, the sum of negative answers is subtracted from 25. Both numbers are added and multiplied by 2.5 to reach a maximum value of 100 allowing a percentile interpretation.
Expert consensus on suitability for training (previously content validity)
Expert consensus on suitability for training (ECT) was assessed by urologists after endoscopic task completion using a 5-point Likert-type questionnaire. Statements were rated from “strong disagreement” (1), to “indifference” (3), to “strong agreement” (5). Average and standard deviation (SD) were calculated for every statement. An average rating >3.9 were considered as agreement to the respective statement, values <3.0 as disagreement, and values in between as indifference.
RPE (previously construct validity)
For RPE, we assessed whether people with different levels of experience, namely urologists and MS, could be distinguished based on their experience with BladCap. Based on urologists' time results for endoscopic tasks, we performed a sample size calculation for the required number of study participants to be enrolled in a prospective RPE validation trial. Therefore, a two-tailed t-test at α = 0.05 and power (1 − β) = 0.9 was conducted. We assumed a 10 seconds higher time consumption for students compared with urologists (SD to be at 4.35 seconds). The respective sample size calculation yielded a study enrollment ratio of 1:10, resulting in 11 urologists and 110 MS required, respectively. Consequently, 12 urologists and 115 MS were enrolled in the validation study and performed predefined tasks twice using BladCap in different training sessions. The tasks were evaluated and contrasted over time. The following tasks were completed: Cystoscopy All colored spots (bladder regions) had to be visualized for task completion (time recording was conducted from the beginning of the insertion of the cystoscope until complete visualization of all spots). Guidewire insertion nsertion of a guidewire into two artificial orifices, large and small (time recording was conducted from the beginning of the insertion of the guidewire until complete penetration of both orifices). Tumor biopsy (TB) Endoscopic detection and biopsy of a sham tumor (time recording was conducted from the beginning of the insertion of the forceps until the tumor was pulled toward the endoscope).
The urologists performed the tasks individually in two consecutive sessions so that the previous user could not be copied. The execution time was recorded manually.
The prospectively enrolled student groups consisted of a maximum of six students per lesson. None of the students had previous endourological experience. After a theoretical introduction to basic endourological interventions, the instructor demonstrated the detailed assembly of a cystoscope and its components. Then, the above-described endourological tasks were slowly executed by the instructor with a detailed description of possible obstacles or hints. The students then performed the tasks. After the first run, additional support by the instructor was offered for a training time of about 30 minutes (5–7 minutes per student). A second round with another completion of the tasks was then added. The first and second sessions were manually time recorded as described above, compared with the subgroup, and benchmarked to the urologists' performance.
In addition to time evaluation, psychomotor skills of students were assessed by a cystoscopic adaptation of the previously described and validated global psychomotor assessment score (GPSS) for ureterorenoscopy. 12 This tool consists of seven sub-items that objectively record aspects of practical skills. Each sub-item is assigned between 1 and 5 points. The sum of the points of the sub-items was then added to the GPSS score. Sub-item Knowledge of Instruments was not collected in this study because the students did not have any prior knowledge of the instruments. The remaining sub-items were applied and assigned as follows: (A) Respect for Tissue, (B) Time and Motion, (C) Handling Scope, (D) Flow of Operations, (E) Use of Assistants, and (F) Knowledge of Specific Procedure (Supplementary Table S2). A GPSS evaluation was not conducted on urologists since they already had prior endoscopic knowledge.
Statistical analysis
The data are expressed as mean ± SD. Statistical analysis was performed with JMP® software (version 14.0.0; SAS Institute, Cary, NC). Mean group comparisons were calculated by the Mann–Whitney U test. All tests were two sided with p < 0.05 considered statistically significant.
Results
BladCap design
First-generation bladder phantoms (n = 7) were successfully printed and evaluated by three urologists (F.B., B.G., M.C.K.) for training purposes. Suggestions for improvement were constantly incorporated into the redesign of BladCap. Consequently, for second-generation bladder phantoms (n = 4) custom fixation loops were designed and printed with the phantom (Fig. 1A). After adjustment, the fixation loops allowed the suspension of the phantom in a customized metallic framework or scaffold. This facilitated sufficient stability during endoscopy for an in-depth realistic ex vivo CY of the corresponding bladder (Fig. 1A, B). The phantoms were printed with filling levels between 350 and 500 mL. Furthermore, the bladder neck was redesigned as a 28-mm disk with a circular orifice of 10 mm. Inner and outer margins were covered by custom-fit rubber loops, which, in the event of an extended endoscopic leverage, allow the bladder neck to protrude without damage (Fig. 1A). The manufacturing cost of the final prototype phantom, including the metallic mount, was about 400€ (CT-scan ≈70€, STL-processing and 3D printing ≈300€, skeleton ≈30€). Series production costs would probably decrease significantly.
Content evidence
ECR and ECT were evaluated by endourology-experienced urologists (n = 12) with an average of 180 cystoscopies per capita. The urologists' responses to the questionnaires allowed for calculation of a SUS score of 89.4 ± 5.9, which translated to an “excellent” rating for BladCap (Fig. 2). ECT was additionally assessed by 5-point Likert-scale questionnaires. On average, a medium-to-strong agreement (≥4) was noted for all aspects questioned (Fig. 3).
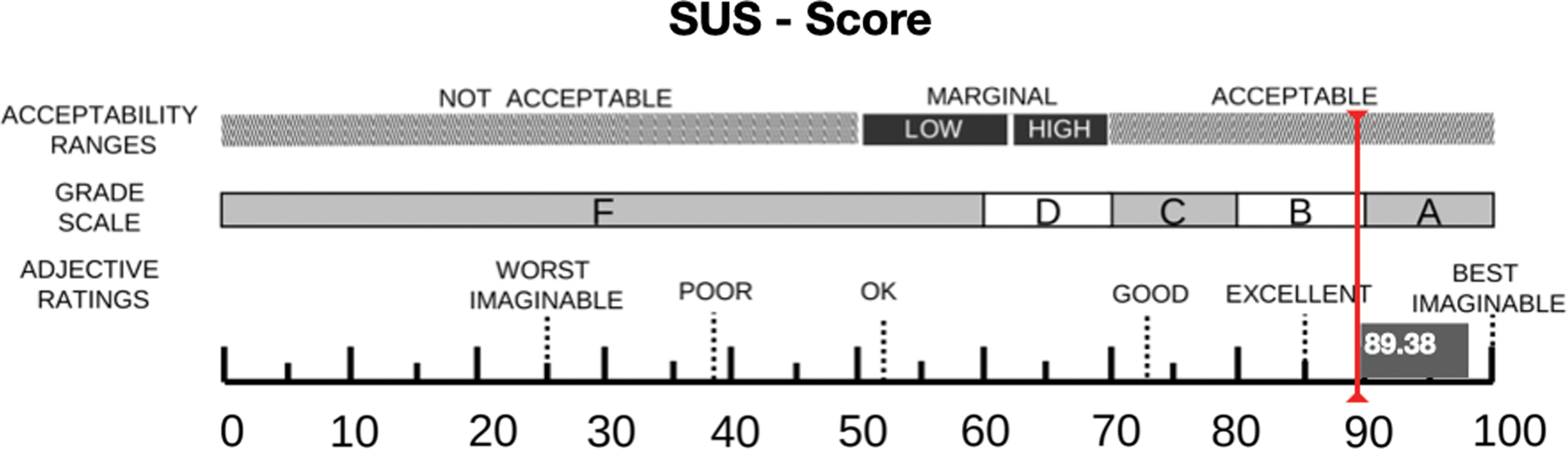
The system usability scale score certified by urologists reaches 89.4, which attests to BladCap “acceptable” usability. Color images are available online.
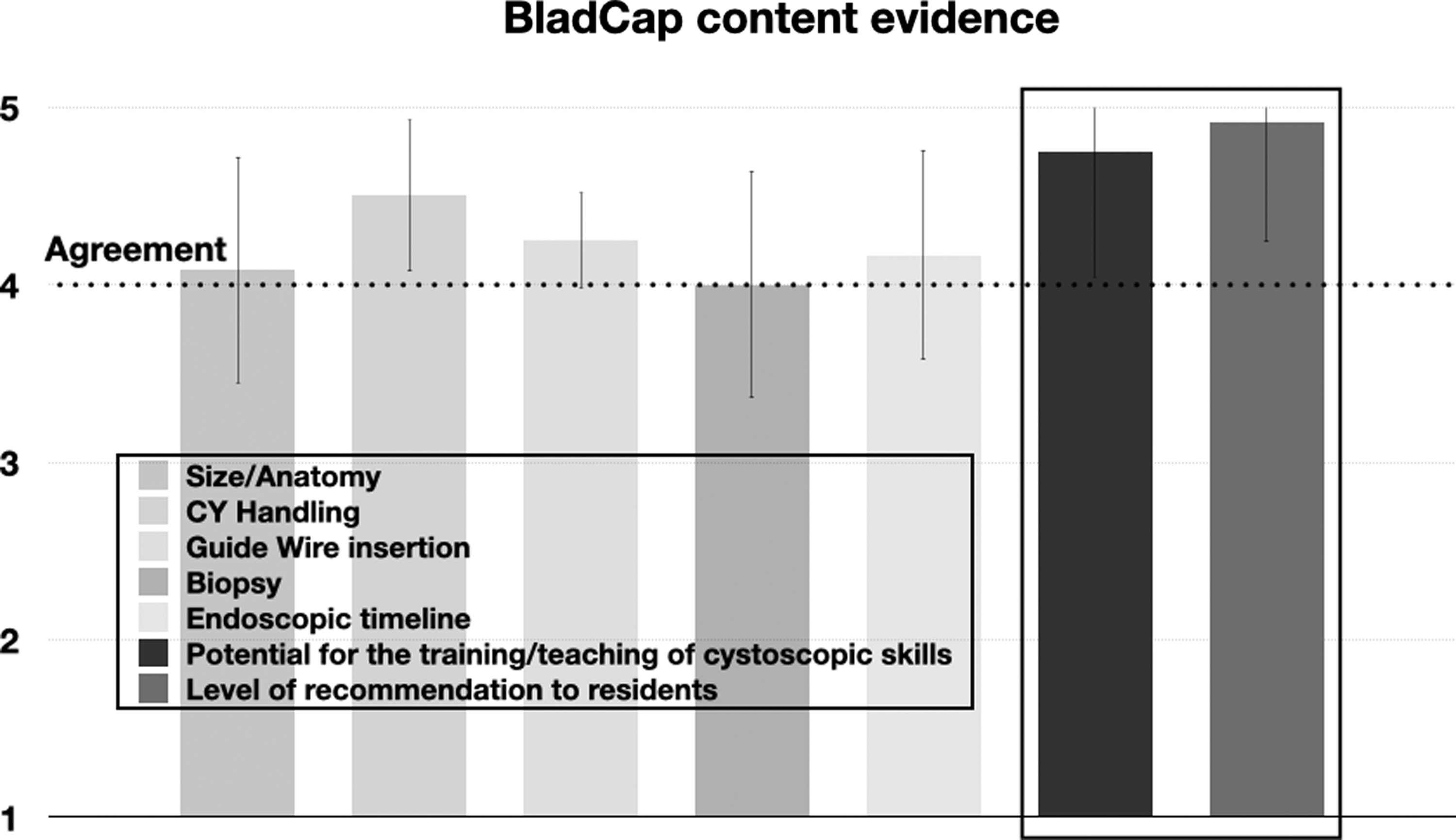
BladCap content evidence. Highest scores were achieved in the recommendation for residents and as potential tool for endourological training.
Urologists reported that BladCap had an appropriate anatomy (4.1 ± 0.6) and the ability to perform realistic endoscopic tasks, including haptic feedback (CY handling [4.5 ± 0.65], GWI [4.3 ± 0.6], biopsy [4.0 ± 0.71], and endoscopic timeline [4.2 ± 0.7]). BladCap received high approval ratings as a useful endoscopy trainer (4.8 ± 0.4) and was strongly recommended to residents for endourological training purposes (4.9 ± 0.3).
Response process evidence
The execution time of the different endoscopic tasks by the urologists differed between the first and second training sessions. A significant time difference could be determined between the two runs for CY and GWI (CY: first 17.6 ± 4.4 seconds vs second 12.4 ± 2.0 seconds, p = 0.002; GWI: first 20.0 ± 6.5 seconds vs second 14.7 ± 4.0 seconds, p = 0.046). For TB, the tendential time reduction of the second session did not reach a level of significance (TB: first 13.9 ± 3.5 seconds vs second 11.7 ± 2.7 seconds, p = 0.088) (Fig. 4A).

Between the first and second training sessions of the students, a significant reduction of the execution time was observed for all tasks (CY: first 56.6 ± 28.2 seconds vs second 28.6 ± 14.7 seconds, p < 0.001; GWI: first 63.0 ± 41.6 seconds vs second 37.3 ± 23.5 seconds, p < 0.001; TB: first 53.8 ± 26.9 seconds vs second 29.5 ± 18.6 seconds, p < 0.001) (Fig. 4B).
For the intergroup comparisons of the training times between U and MS, highly significant differences were determined for each task in each run (all comparisons p < 0.001) (Fig. 4), including CY (second U 12.4 ± 2.0 seconds vs second MS 28.6 ± 14.7 seconds, p < 0.001).
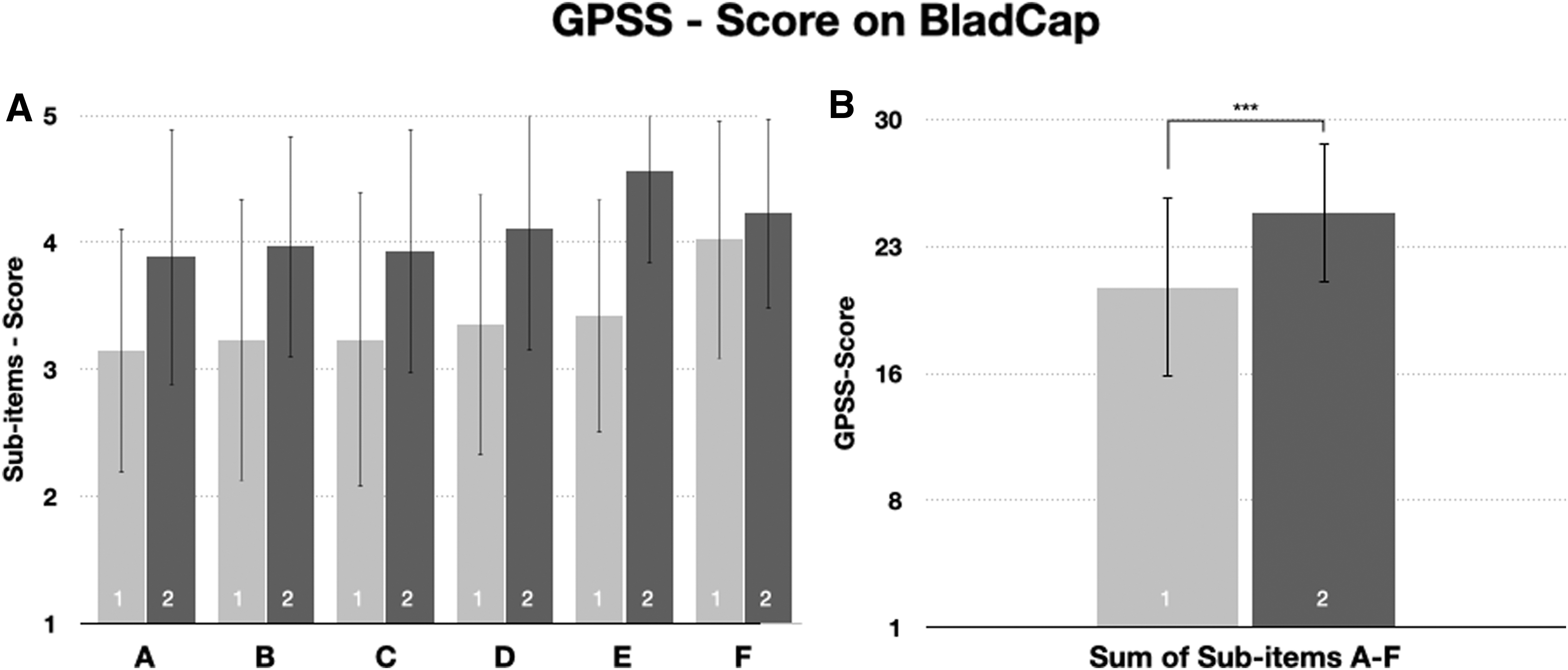
In addition to time recording, the evolution of practical skills among the MS was recorded between sessions using the GPSS. The individual sub-items A-F showed differences between the first and second runs (A: first 3.2 ± 1.0 pts vs second 3.8 ± 1.0 pts; B: first 3.2 ± 1.1 pts vs second 4.0 ± 0.9 pts; C: first 3.2 ± 1.2 pts vs second 3.9 ± 1.0 pts; D: first 3.4 ± 1.0 pts vs second 4.1 ± 1.0 pts; E: first 3.4 ± 0.9 pts vs second 4.6 ± 0.7 pts; F: first 4.0 ± 0.9 pts vs second 4.2 ± 0.8 pts). These results were reflected in the total GPSS, which improved significantly in the second run (GPSS first 20.4 ± 5.1 seconds vs second 24.7 ± 4.0 seconds, p < 0.001), attesting to a positive practical training effect for BladCap (Fig. 5).
Discussion
CY is an essential skill required for almost all urologists regardless of which subspecialty is pursued. It is the basis for skill development of all endourological procedures as well as one of the most important basic diagnostic tools. 1 There is broad surgical consensus that ex vivo practical training sessions should be performed before patient intervention. 13 Ex vivo training devices allow for trial and error in a safe environment. 14 Early training of hand/eye coordination is important in the development of surgical skills. 15 However, while the use of simulators before carrying out critical maneuvers is standard in aviation or the military, the medical field seems to lag behind. 3 Training in CY is essential, since past studies have shown that trainees subjectively report significantly less viewing of the entire bladder surface. 16 Other investigations on transurethral resections of bladder tumors have shown that the first 45 executions are associated with the poorest results in terms of recurrence-free survival. 17 These studies highlight the importance of ex vivo endoscopic training in urology. Since the success of practical learning depends upon an early onset of training, the integration of phantoms in medical education would be an ideal approach. Subsequent prospective studies will have to be performed to clarify such benefits.
Simulators in urology
There are several CY simulators of varying quality that have been described in urological literature, 18 –22 but none of them has achieved widespread educational use. This may result from some of them being strictly virtual trainers, whereas others combine CY with ureterorenoscopic training. Furthermore, the acquisition of the simulators in some cases is costly. 23 Comparisons between simulators are limited due to a lack of standardized validation measures. 24
BladCap processing and validation
With the development of BladCap, we aimed to create a realistic, easy-to-produce, robust, and functionally reproducible phantom with haptic feedback for the purpose of simulating basic endourological tasks. By incorporating a direct view of accurate anatomy of the bladder and its correct position in the body during CY, we intended to increase intervention-specific comprehension. To provide a robust evaluation against the most common, but highly subjective, validation criteria of face and content validity, we objectified the construct validity of BladCap by prospective intra- and intergroup comparisons of probands with alternative endourological skillsets. In addition, objectivity in practical skill assessment was enhanced by recording the GPSS using BladCap. Results show that the initial positive subjective evaluation of BladCap by urologists can also be measured by temporal and practical training effects across different skill levels. Thus, BladCap can be a useful simulator for initial training in endourological practice and also for the training of experienced endoscopists on new types of endoscopes. In fact, we were able to use BladCap in a previous study to train surgeons on a novel variable-view rigid endoscope (EndoCAMeleon®). After mastering the endoscope-specific functions in BladCap, the endoscope was safely used in a clinical pilot study. 25
Training simulators can be classified as either high or low fidelity depending on the complexity of the model. Randomized controlled prospective studies have shown that low-fidelity models are not inferior to high-fidelity models in terms of training effects. 18 BladCap is a low-fidelity phantom with objective anatomical accuracy but without the ability to vary bladder volume or realistically represent bladder tissue. CY, GWI, or TB, however can be efficiently trained on BladCap. We are convinced that BladCap allows us to present endourologic trainees with the nonspherical, realistic anatomy of the bladder without over-challenging them for completion of robust and goal-orientated endourological tasks. Thus, structure and functionality are in a better balance in terms of complexity, which reinforces the usability of BladCap. BladCap is one of the few 3D-printed bladder phantoms available. Because of the processing work, anatomical variations can be quickly applied to the phantom, resulting in increasing levels of difficulty of an already familiar model. The favorable manufacturing costs along with practical and effective training possibilities should position BladCap as an attractive simulator for urological training.
Limitations
A limitation of the study is that we did not capture consequence evidence (transferability of the simulation to the real world or ability to reach expert levels after repeated simulations) for BladCap, which was not considered advisable in the first presentation of BladCap. This is planned for the next-evaluation step and requires longer planning and a multicenter setting. In addition, we did not include real-life endpoints, such as an effect on patient pain perception during CY after user training on BladCap. Furthermore, this study setting does not allow a valid statement about an actual influence of endoscopic complications in a real CY. Also, the time recording was done by means of a manual chronometer, which may be susceptible to minor inaccuracies. However, the global time differences were high enough to render this irrelevant. The fact that the urologists also showed significant time changes between the attempts demonstrates a habituation effect on the model, which calls into question the improvements of the beginners through the teaching session. However, the subgroup differences between the attempts were constantly different as well, which neutralizes the effect. Furthermore, time measurement was the only common endpoint of both groups. Other endpoints, such as tumor detection rate or recurrence rate, were not possible due to model limitations. Finally, a bias may have been introduced by some students who may have been able to recognize and correct the mistakes of the previous group. However, this effect is likely insignificant due to the cohort size (n = 115).
Conclusion
The acquisition of endourological skills and the ability to perform detailed cystoscopies are highly important in surgical training and urological practice. In this study, we designed an anatomically accurate model for training purposes. A high content and RPE was shown with significant differences in all tasks and trials. The future implementation of this model in resident or student education has the potential to accelerate training in a safe and supportive environment.
Footnotes
Author Contributions
F.W.: project development, data collection, figure editing, and article drafting; L.v.R.: phantom development, endoscopic training, and data collection; M.N., B.G.: endoscopic exploration, S.H., R.S.-I., A.M.: project supervision and article editing; M.R.: project supervision; M.C.K.: project development, statistical guidance, and figure and article editing.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
The work was supported by the German Federal Ministry of Education and Research. Project 13GW0203A: “Digital platform with 4PI real-time endoimaging for endoscopic 3D reconstruction, visualization, and aftercare support in the healthcare of patients with bladder carcinoma”.
Supplementary Material
Supplementary Table S1
Supplementary Table S2
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.