
Abstract
Background:
Robotic pelvic surgery is being increasingly utilized for reconstruction proximal to the genitourinary diaphragm. We describe a combined robotic, transabdominal, and open transperineal approach for complex anastomotic posterior urethroplasty.
Materials and Methods:
We performed a multi-institutional retrospective study of patients who underwent anastomotic posterior urethroplasty by a combined robotic, transabdominal, and open transperineal approach between January 2012 and December 2018. Patient demographics; preoperative, intraoperative, and postoperative clinical data; and complications were reviewed. Urethroplasty success, de novo stress urinary incontinence (SUI), and de novo erectile dysfunction (ED) were evaluated.
Results:
Twelve patients were identified with a mean follow-up of 596 (range 73–1618) days. Mean patient age was 65.9 (range 53.4–76.8). Reconstruction required corporal splitting, prostatectomy, and gracilis muscle flap use in one (8.3%), eight (66.7%), and four (33.3%) patients, respectively. Postoperative urinary leak, thromboembolic event, and wound abscess occurred in one (8.3%), one (8.3%), and two (16.7%) patients, respectively. Stenosis recurrence occurred in two patients (16.7%) at a mean 187.5 (20–355) postoperative days. De novo ED and de novo SUI were reported in two (16.7%) and four (33.3%) patients, respectively. Nine patients (75.0%) underwent placement of an artificial urinary sphincter at a mean interval of 359.2 (111–1456) days after the index procedure, with no subsequent erosion.
Conclusions:
Complex posterior urethroplasty by a combined robotic, transabdominal and open transperineal approach is associated with success and complications rates that are comparable to open techniques and may allow for adjunctive procedures such as prostatectomy. This technique allows for the reconstruction of posterior urethral stenoses that would otherwise have been managed conservatively or with urinary diversion.
Introduction
Posterior urethral stenoses most commonly present to the reconstructive urologist after pelvic fracture urethral injury, and complications of pelvic radiation therapy or bladder outlet procedures. Many of these stenoses extend through the membranous urethra into the proximal bulbar urethra, and thus they present the added complexity of external urinary sphincter proximity and the potential to result in urinary incontinence during repair.
Stenosis length, location with respect to the urinary sphincter, bladder neck integrity, and surrounding tissue fibrosis must be carefully considered during surgical planning for posterior urethral reconstruction. Traditionally these stenoses have been repaired transperineally, abdominally if completely proximal to the urogenital diaphragm, or abdomino-perineally. During transperineal reconstruction, ancillary maneuvers such as urethral mobilization, corporal splitting, supracrural urethral rerouting, and partial or complete pubectomy may be sequentially employed to mobilize the urethra for a tension-free anastomosis. 1,2 Moreover, a transperineal approach to reconstruction of the urethra proximal to the genitourinary diaphragm is inherently transphincteric and will result in urinary incontinence, unless the patient has a normally functioning bladder neck. As a result of both the intrinsic complexity of the repair and the risk of urinary incontinence, treatment with transperineal posterior urethroplasty is often rejected for more conservative management with catheter dependence or more invasive surgery with cystectomy and ileal conduit urinary diversion. 3
Robotic surgery has dramatically changed access to the deep pelvis, and it has shown great promise in the management of recurrent bladder neck contractures and vesicourethral anastomotic stenoses. 4 The shift to a mostly robotic transabdominal approach may provide the advantages of dissection and mobilization of the urethra posterior to the urogenital diaphragm, and the ability to concurrently address any intrapelvic pathology. We describe the technique for a combined robotic-assisted transabdominal and open transperineal approach to posterior urethral stenoses. We aimed at assessing the safety, urethral patency rates, and complications associated with this combined robotic-assisted transabdominal and open transperineal approach to posterior urethroplasty.
Materials and Methods
Study cohort
Under an institutional review board-approved protocol, a retrospective chart review was performed of all patients who underwent anastomotic posterior urethroplasty by a combined robotic-assisted transabdominal and open transperineal approach by two fellowship-trained reconstructive urologists at two tertiary referral centers between January 2012 and December 2018.
Our approach of robotic transabdominal dissection for urethral stenosis proximal to the external urinary sphincter has previously been reported. 4 The current study focuses on patients who required perineal mobilization to complete the anastomosis via a combined robotic-assisted transabdominal and open transperineal approach.
Procedure
This progressive approach to posterior urethral stenosis begins with the robotic-assisted transabdominal dissection. The robotic portion is performed initially, as some of the stenoses can be reconstructed purely from a transabdominal approach, thus obviating the need for transperineal dissection (Supplementary Video SV1). Avoiding corporal rerouting of the traditional progressive transperineal approach further facilitates subsequent artificial urinary sphincter (AUS) placement in patients who experience stress urinary incontinence (SUI).
Dissection of the bladder, prostate if present, and urethra then proceeds in the same fashion as would be performed for a prostatectomy. Prostatectomy with vesicourethral anastomosis may be performed if indicated based on the presence of prostatic urethral stenosis or other prostate pathology. Denser fibrotic tissue is typically encountered as the dissection proceeds toward the prostate apex, depending on the stenotic urethral segment and the stenosis etiology. Relaxing incisions are made in the posterior peritoneum if anastomotic tension on the urethra is anticipated.
The urethra is then transversely incised, and if healthy urethral mucosa is not encountered, the urethra is further mobilized distally from the dorsal vein, pelvic floor, and any surrounding fibrotic tissue. As the urethra is transected, this approach does not spare the bulbar arteries.
To determine whether perineal mobilization of the urethra is needed, a test suture in the posterior bladder neck is used to determine whether it will reach the urethra without tension. If with maximal bladder mobilization and the pneumoperitoneum lowered to 5 mm Hg, a gap still exists between the bladder neck and the urethra, the open transperineal approach is then performed for further urethral mobilization. If the robot is docked from the side, the transperineal approach can be performed concurrently (Fig. 1a, b).
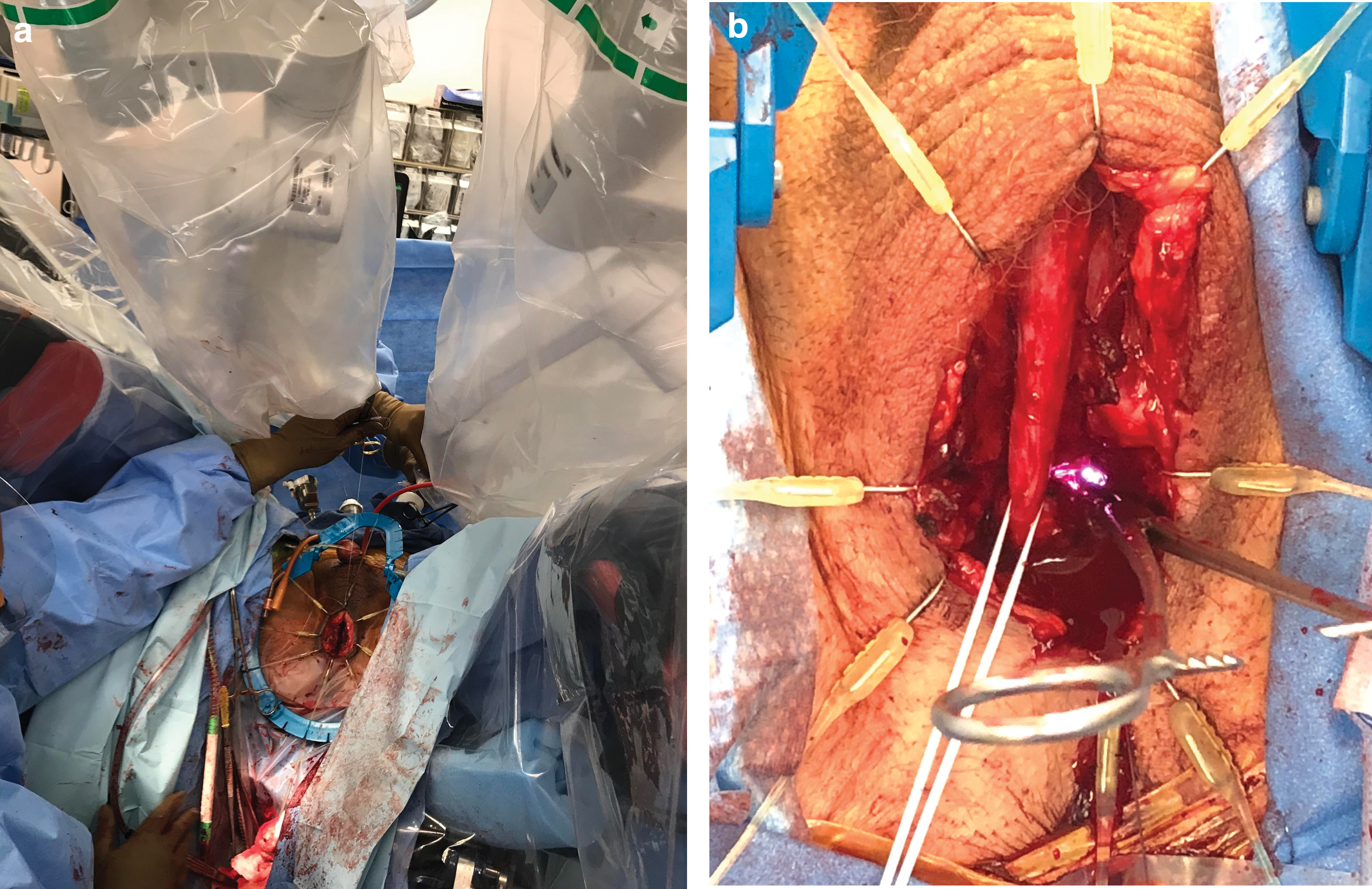
The robotic system is side-docked to allow for concurrent perineal access
The open transperineal approach begins with a midline perineal incision and dissection down through the subcutaneous fat and connective tissue to the bulbospongiosus muscle. The bulbospongiosus muscle is then longitudinally incised in the midline. The urethra is mobilized circumferentially, down through the urogenital diaphragm, taking down the perineal body in the process. The urethra is then transversely incised distal to the stenotic urethral segment. The distal urethra is dorsally spatulated 1 cm. A holding suture is placed through the dorsal apex of the urethrotomy and passed above the urogenital diaphragm to allow advancement of the distal urethra into the pelvic cavity for the urethrovesical anastomosis. At this point, there will be a communication through the pelvic floor, resulting in loss of pneumoperitoneum. The AirSeal device (ConMed, Utica, NY, USA) can help maintain pneumoperitoneum. Alternatively, a moist sponge can be placed in the perineal wound and sealed with a 3M® Ioban® antimicrobial surgical drape (3M Medical®, Saint Paul, MN, USA) to maintain pneumoperitoneum for the subsequent robotic-assisted vesicourethral anastomosis portion of the procedure.
The holding suture previously placed on the distal urethra is grasped robotically to pull the urethra into the pelvis (Fig. 2). Then, the robotic-assisted urethrovesical anastomosis is performed with two 3-0 barbed monocryl sutures in a running fashion, tied anteriorly over an 18F urethral catheter. Anastomotic integrity is tested with a fluid leak test. Unilateral or bilateral gracilis muscle flaps may be utilized to provide a well-vascularized tissue bed to the urethral anastomosis and robust tissue interposition to the rectum without tension. A #10 closed-suction drain is placed through one of the lateral trocar sites, in close proximity to the bladder, and left to bulb suction.

A holding suture placed on the distal urethra from the perineal approach is grasped robotically to pull the urethra into the pelvis. This facilitates robotic-assisted vesicourethral anastomosis. Color images are available online.
Postoperative care
The pelvic closed-suction drain is left in place until drainage is less than 30 mL over 24 hours. Voiding cystourethrogram (VCUG) is performed 3–4 weeks postoperatively.
Follow-up
Patients were followed at 3–6 and 12 months postoperatively with history, including subjective voiding and sexual function symptoms, uroflowmetry, postvoid residual urine measurement, and 16F flexible cystoscopy. Thereafter, patients were followed annually with the aforementioned evaluation except that flexible cystoscopy was reserved for patients with a significant change in voiding symptoms or uroflowmetry.
Variables
Patient demographics, preoperative and postoperative clinical data were obtained. Urethroplasty success was anatomically defined by atraumatic passage of a 16F flexible cystoscope. Urinary incontinence was defined as patient-reported use of >1 pad per day or undergoing surgical treatment for SUI. Erectile dysfunction (ED) was defined as the patient-reported inability to maintain an erection sufficient for penetration.
Postoperative complications were recorded by using the Clavien-Dindo classification system 5,6 (CDG; I, II, IIIa, IIIb, IVa, IVb, V).
Data maintenance and statistical analysis
Data from the customized REDCap® database were securely exported to Microsoft® Excel® version 2016 (Microsoft Corporation®, Redmond, WA, USA) for descriptive statistical analysis. 7
Results
Study cohort descriptive statistics
A total of 12 patients underwent anastomotic posterior urethroplasty with a mean follow-up of 596 (range 73–1618) days. Median follow-up was 475 days. Patient demographics are found in Table 1. Mean age for the study cohort was 65.9 (range 53.4–76.8) years. Mean weight and body mass index were 85.2 (range 63.8–108.9) kg and 26.9 (range 21.6–33.3) kg/m2, respectively. Median age-adjusted Charlson Comorbidity Index 8 was 4 (range 0–6), indicating a moderately morbid study cohort. Overall, 10 patients (83.3%) had previous radiation therapy for prostate cancer, one (8.3%) of whom also had a salvage prostatectomy.
Study Cohort Descriptive Statistics (N = 12 Subjects)
DVIU = direct vision internal urethrotomy; EBRT = external beam radiation therapy.
Intraoperative data can be found in Table 2. Given that some patients required additional procedures such as corporal splitting or prostatectomy, more than one urethral reconstruction technique may have been used for a given patient.
Intraoperative Data (N = 12 Subjects)
Postoperative complications varied in severity (Table 3). In the immediate postoperative period, one patient (8.3%) demonstrated contained urinary extravasation at the urethral anastomosis site on VCUG that was conservatively managed with observation (CDG I); one patient (8.3%) developed a deep venous thrombosis and a pulmonary embolus that required anticoagulation (CDG II); and two patients (16.7%) developed wound abscesses, one of which required bedside drainage (CDG I) and one of which required percutaneous drainage under general anesthesia (CDG IIIb). Posterior urethral stenosis recurrence requiring surgical intervention occurred in two patients during the follow-up period (16.7%; CDG IIIb). Of note, the recurrent stenoses occurred in the patients who had developed wound abscesses in the initial postoperative period. Mean time from the index procedure to the detection of the posterior urethral stenosis recurrence was 187.5 (range 20–355) days. One recurrence was treated with a subsequent posterior urethroplasty with oral mucosal graft, and one recurrence was treated with radical cystectomy and the creation of an ileal conduit for urinary diversion.
Postoperative Complications After Posterior Urethroplasty by Combined Robotic Transabdominal and Open Transperineal Approach (N = 12 Subjects)
De novo ED occurred in two patients (16.7%), both of whom were treated medically (CDG II). De novo SUI occurred in 4 patients (33.3%), all of whom were treated with AUS placement (CDG IIIb) [Table 4]. Of the six patients (50.0%) who exhibited SUI before the index procedure and the four patients (33.3%) who developed de novo SUI after the index procedure, a total of nine patients (75.0%) underwent placement of an AUS at a mean time from the index procedure of 359.2 (111–1456) days. To date, none of the patients who underwent subsequent AUS placement have experienced urethral atrophy or erosion requiring AUS explantation.
Stress Urinary Incontinence Management (N = 12 Subjects)
AUS = artificial urinary sphincter; SUI = stress urinary incontinence.
Discussion
To our knowledge, this is the first study describing a combined robotic-assisted and open transperineal approach for complex posterior urethroplasty. Our study indicates that challenging stenoses involving the posterior urethra can be successfully reconstructed with acceptable morbidity. This further advances the emerging approach to the posterior urethra as primarily a robotically-driven operation.
Literature describing the use of the robotic platform to facilitate urethral reconstruction is very limited. Unterberg and colleagues 9 reported using the robot for the assistance of perineal urethroplasty, in which open urethral dissection is performed first. The robot is docked at the time of urethral anastomosis to facilitate suture placement. In this series, most patients had strictures limited to the bulbar urethra, and only 10% involved stenoses of the prostatic urethra.
We propose that the transabdominal approach allows for access to the deep pelvis to facilitate dissection of the bladder neck and proximal urethra and to perform prostatectomy and bladder neck reconstruction if indicated. The anastomoses are performed with robotic assistance above the urogenital diaphragm, whereas the mobilization of the more distal urethra and any ancillary maneuvers are performed via the open transperineal approach to manage any bulbar component of the stenosis and gain the necessary length on the urethra to allow for a tension-free anastomosis.
A more comparable patient cohort may be found in a study of high-risk long-segment urethral strictures treated with augmented urethroplasty using ventral buccal mucosa graft reinforced with a gracilis muscle flap bed. 10 In this series, 45% of patients underwent radiation therapy, and 50% demonstrated stenosis of the posterior urethra. Palmer and colleagues describe a mean stricture length of 8 cm, with no cases of complete urethral obliteration, thus lending to reconstruction with buccal mucosa graft augmentation. 10 In our study, 25% of the patients had complete urethral obliteration with stenoses short enough for the anastomotic approach. Similar urethral patency outcomes between the two approaches suggest that both work well for complex posterior urethral stenoses depending on the presence of urethral obliteration and the length of the stenosis. 11 –13
The development of urinary incontinence is an important consideration for patients with membranous urethral stenosis, especially after radiation. De novo SUI developed in 28.6% of patients in a study by Hofer and colleagues of anastomotic urethroplasty for radiation-induced bulbomembranous urethral strictures. 13 With a mean follow-up of 3.5 years of 10 patients with pre-existing SUI and 12 patients with de novo SUI, 9 patients (40.9%) underwent AUS placement without mention of the subsequent need for removal. Chung and colleagues 14 reported de novo SUI in 23.2% of patients with an intact bladder neck after transperineal anastomotic urethroplasty with or without gracilis muscle flap for radiation-induced and traumatic posterior urethral stenoses, a patient cohort most akin to that of the current study. Chung and colleagues further report that at a mean study follow-up of 18 months, three patients (18.8%) with SUI after the index procedure underwent subsequent AUS placement, two of which had subsequent AUS removal for erosion or poor coaptation.
An important rationale for the robotic-assisted transabdominal and open transperineal urethroplasty is the potential decrease in AUS erosion risk by minimizing bulbar urethral mobilization. Prior bulbar urethral mobilization, in particular, has been demonstrated to be an independent risk factor for AUS cuff erosion when controlling for history of pelvic radiation. 15 By mobilizing the bladder neck distally, there may be less tension on the bulbar urethra from the anastomosis. In our study, of the six patients (50.0%) who had preoperative SUI and the additional four patients (33.3%) who developed de novo SUI after the index procedure, nine patients (75.0%) underwent subsequent placement of an AUS without removal at a mean study follow-up of 19.3 months. Longer-term data are needed to determine whether this technique reduces AUS erosion and revisions.
Limitations of this study include its retrospective nature, small sample size, lack of an open transabdominal approach comparison arm, and short-term follow-up. Multi-institutional collaborations from high-volume reconstructive urologic practices located in diverse regions may be warranted. Patient-reported changes in quality of life would be an important complement to objective surgical outcome data in future studies.
Conclusion
This study builds on the outcomes of a previously described robotic bladder neck reconstruction and posterior urethroplasty approach without concurrent perineal dissection. 4 In this study, we found that even when perineal urethral dissection is necessary, the combined robotic-assisted transabdominal and open transperineal approach results in urethral patency, anastomotic urinary leak, de novo SUI, and de novo ED rates that are comparable to traditional posterior urethroplasty in similar patient populations. This technique facilitates reconstruction of posterior urethral stenoses that are often otherwise managed conservatively or with the end-stage option of urinary diversion.
Footnotes
Authors' Contributions
The contributions of each of the authors were as follows: study conception and design: J.A.C., A.J.V., D.C., and L.C.Z. Acquisition of data, analysis and interpretation of data, drafting of article, and critical revision: J.A.C., A.J.V., G.W.D., S.S., N.A.S., D.C., and L.C.Z.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.
Supplementary Material
Supplementary Video SV1
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.