
Abstract
Background:
We wished to determine whether newly available flat panel detector (FPD) c-arms were (1) associated with lower radiation dose during ureteroscopy (URS) than conventional image intensifier (CII) c-arms and (2) to compare fluoroscopic image quality between the units.
Materials and Methods:
We retrospectively reviewed 44 consecutive patients undergoing URS at a pediatric hospital, with c-arms assigned by availability in the operating room. We performed dosimetry experiments using the same c-arms on standard phantoms.
Results:
Patient and case characteristics did not differ significantly between the two groups of patients. The median dose in the FPD group was less than a quarter of the dose in the CII group, 0.48 [0.42, 0.97] mGy vs 2.2 [1.1, 3.8] mGy, p < 0.0001. The FPD dose remained at less than one-third of the CII dose accounting for any difference in fluoroscopy time, and remained significant in a multivariate model including fluoroscopy time and patient weight (β = 2.4, p = 0.007). Phantom studies showed higher image quality for FPDs at all simulated patient sizes, even at lower radiation doses.
Conclusions:
This is the first report comparing radiation dose from c-arms of image intensifiers and FPDs in adults or children. Use of an FPD during URS was associated with a substantially decreased absorbed dose for patients while simultaneously improving image quality.
Introduction
Digital radiography using flat panel detectors (FPDs) has so fundamentally changed the way fluoroscopic and plain film images are processed that it has been clear for decades that “the future of radiography will be digital.” 1 Digital imaging has only recently become available in mobile units, and so only analog X-ray imaging with conventional image intensifiers (CIIs) with a c-arm has been available for the urologist in the general operating suite. The difference in image detectors is analogous to film vs digital photography, the latter allowing for digital image processing and contrast enhancement.
Radiation exposure from fluoroscopy-guided procedures is important for all patients, and becomes particularly relevant when treating children because of their greater radiosensitivity and longer life span. 2,3 With the increasing incidence of pediatric nephrolithiasis, there has been a corresponding increase in cumulative radiation exposure related to diagnosis and treatment of this disease. 4 There are several studies tracking the radiation exposure associated with fluoroscopy during surgical treatment of stones, but there are only six studies measuring doses in pediatric patients. 5 –9 Furthermore, there are no studies on differences in radiation exposure from FPDs vs CIIs in fluoroscopy-guided endourologic procedures in adults or children.
Our operating room purchased several FPD c-arms and maintained several modern CII c-arms as well, allowing us to compare the difference. During clinical care we had observed that when provided with an FPD unit, image quality appeared higher and radiation dose appeared lower. Our primary hypothesis was that absorbed radiation dose would be lower in a cohort of children undergoing ureteroscopy (URS) with an FPD portable c-arm compared with those undergoing URS with a CII unit during the same time period by the same surgeons.
We wished to ensure that the effect seen was due to the detector type alone, and not due to differing settings between the machines or other modifiable factors. As c-arm settings were already optimized for minimum dose by clinical engineers, we could not alter these, and instead conducted a second study with phantoms. Our secondary hypothesis was that the dose differences seen clinically would persist in phantom measurement and that image quality from FPDs would be superior.
Materials and Methods
After IRB approval, we performed a retrospective review of all cases undergoing URS in our institution between January 2018 and January 2019, selecting this period as the time of maximum overlap between the two units. This was designed to minimize the impact of any environmental factors, changes in practice patterns, or other sources of bias from using temporally distinct periods.
We used two mobile c-arms present in our operating suite, both from Philips (Koninklijke Philips N.V, Amsterdam, Netherlands). The CII is a Philips BV Pulsera; the FPD is a Philips Veradius Unity. Both units have doses set according to ALARA and Image Gently® principles, and each is monitored yearly by clinical engineers.
We performed a fluoroscopy time out before using c-arms, standardizing factors such as c-arm settings and the distance of the detector from the patient. These are outlined in our prior work 9 ; adherence to this time out is prospectively tracked for all urologic cases involving fluoroscopy. C-arms were assigned at the moment of the case by the operating room fluoroscopy team based on availability. Absorbed dose, or cumulative reference point air kerma, was defined as the radiation dose to air at 30 cm from the image detector.
During in vitro work, poly(methyl methacrylate) (PMMA) phantoms consisting of 10, 15, and 20 cm of PMMA were exposed at manual kVp settings (60, 65, and 75 kVp) on each machine, and the corresponding mA and entrance skin dose rate for each phantom size and menu were then recorded. Measurements were taken at 30 cm from the detector surface for both groups. The differing thickness of phantoms is designed to account for the varying anterior–posterior (A-P) measurements of patients at a pediatric hospital.
Descriptive statistics were generated. Bivariate comparisons used the Fisher's exact test or Wilcoxon rank sum; a logistic regression was performed using variables selected a priori to have the most impact on dose (fluoroscopy time and body mass index [BMI]). A two-tailed p < 0.05 was used as the threshold of significance with analysis performed in JMP®, Version Pro 14. SAS Institute, Inc., Cary, NC.
Results
Forty-four consecutive patients were identified and included: 22 patients underwent URS with CII fluoroscopy and 22 with FPDs. Table 1 describes the cohort, and the symmetric group size was by chance. Median age was 16.6 years [IQR 11.7, 19.3], gender was 52% (n = 23) female, and BMI was 21.2 kg/m2. We placed stents in nearly all cases (97.6%), used sheaths in half of cases, and stones were renal in 27 cases (61.4%) and ureteral in 25 cases (56.8%), some patients had both. There were no differences between the cohorts with respect to age, gender, weight, BMI, proportion of patients presented, placement of a stent or a ureteral access sheath, stone location, greatest stone dimension, or procedure duration. There were no differences in provider access to and usage of different c-arms.
Description of Full Cohort with Comparison of Demographic Factors, Complexity, and Dosimetry by Group
Format: median [IQR].
Wilcoxon rank sum.
Fisher's exact test.
Categories not mutually exclusive; a single patient may have stone in both kidney and ureteral location.
IQR = interquartile range.
Importantly, fluoroscopy time did not differ between the groups, with 0.3 [0.1, 0.53] minutes for the CII group and 0.2 [0.1, 0.3] for the FPD group. Absorbed dose was 2.2 mGy [1.1, 3.8] in the CII group and 0.48 [0.42, 0.97] in the FPD group, p < 0.001. Simple division by time provides the dose per minute, and it remains substantially different: 7.8 mGy/min in the CII group vs 2.4 mGy/min in the FPD group, p = 0.0002 (Fig. 1). We performed a logistic regression including the covariates of fluoroscopy time and patient weight, and the difference again remained significant (β = 2.4, p = 0.007).
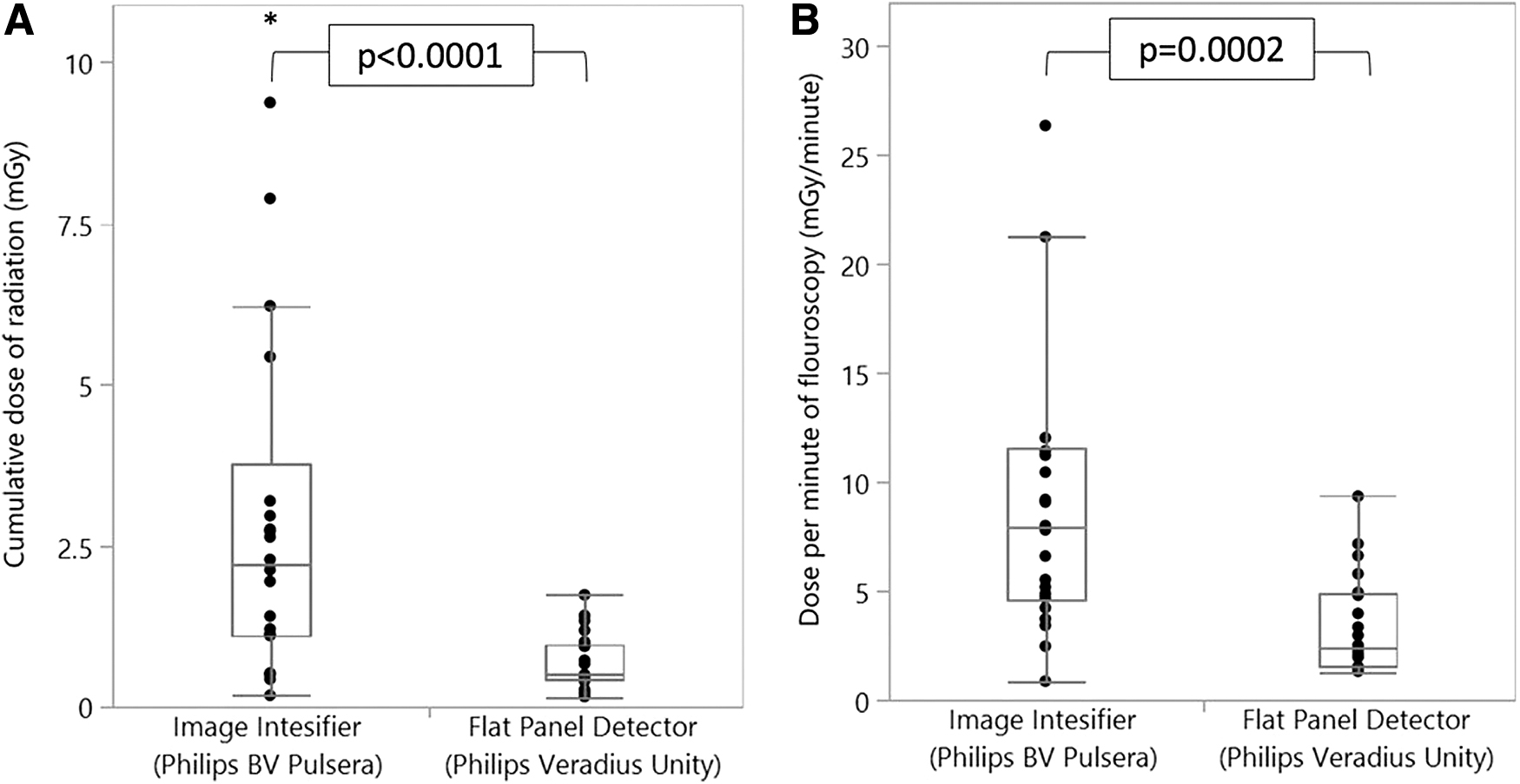
The figure shows the marked difference in dose between imagine intensifier and FPD. This is true for cumulative dose during the case
In phantom studies, at all simulated patient A-P diameters, dose was at least 11% lower for the FPD unit even while imaging at twice the frequency of the CII unit. Image quality was judged in paired line phantoms; the closer the two lines that can be visually discerned implies a higher resolution. Appendix Figure A1 shows the experimental setup. Figure 2 shows one sample image, in which the blurriness is evident even when the FPD is providing a lower dose. Appendix Figure A2 shows the higher signal-to-noise ratio and higher contrast at all simulated patient thicknesses and image acquisition rates.
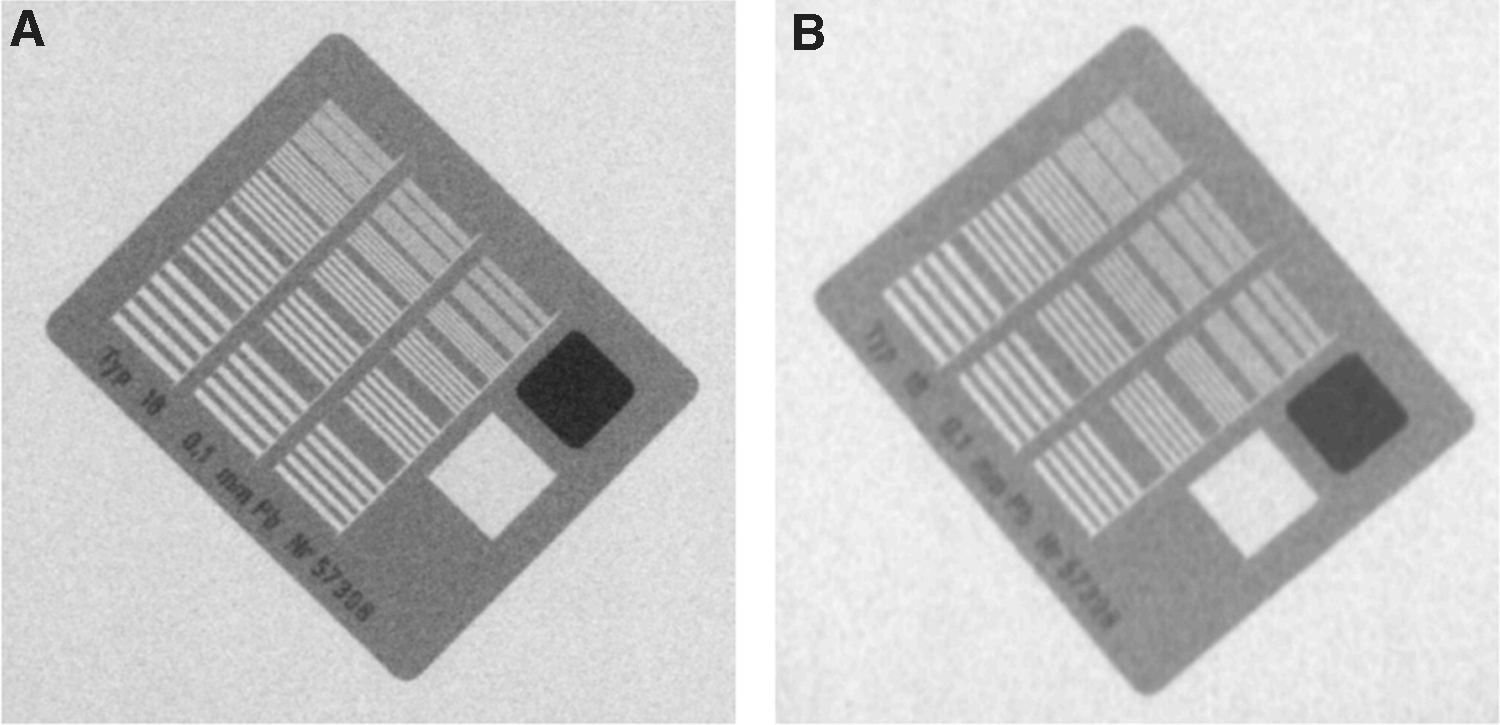
Phantom images of paired line phantoms (
Discussion
Fluoroscopy has an established role in safe performance of URS, and authors have appropriately focused on dose. Dudley et al. prospectively monitored radiation exposure of pediatric patients undergoing fluoroscopic urologic procedures. They found that in 32 pediatric patients who underwent URS, the mean radiation dose exposed to children was 1.21 mGy with a mean fluoroscopy time of 38.3 seconds. 8 A similar study by Ristau and colleagues on 93 pediatric patients undergoing URS for stone treatment demonstrated an average fluoroscopy time of 1.6 minutes and mean estimated effective dose was 2.3 mSv for 93 patients. 7 The authors found that the calculated average effective dose was 0.024 mSv/s for fluoroscopy. According to current guidelines, it was accepted that the maximum safe radiation dose is 50 mSv per year, with an average dose <20 mSv per year over any 5-year period. 10 These data show that fluoroscopy usage during URS is an important source of exposure to pediatric patients. Our study fits in this range, on the lower end of exposure and fluoroscopy time.
A number of investigators have assessed factors that impact radiation dose in fluoroscopy during URS including surgeon vs technologist control, 9 protocols or checklists, 11 adjustments in fluoroscopy settings, 12 and level of training of surgeon. 13,14 Cabrera et al.'s study is the only study investigating difference in exposure during URS based on device type comparing a fixed fluoroscopic device and mobile C-arm, but both units were CIIs. 15
The results of our study demonstrate a significant decrease in intraoperative radiation dose in the FPD group as compared with the CII group during ureteroscopic treatment of stones in pediatric patients. In FPD systems, the amount of radiation required to produce the image is not specific as in CII X-ray systems, where more radiation makes the film darker and decreases the contrast of the examination. Hence, although FPDs should reduce radiation dose due to improved detective quantum efficiency, results of comparative dose investigations in fixed fluoroscopic systems have been mixed, 16 –19 perhaps as FPD technology has improved over time. In the early generation of FPDs, the signal amplification necessary in low-dose images introduced inherent electronic image noise and actually decreased image quality in fluoroscopic applications. 20 Manufacturing of FPDs with electronic noise characteristics low enough to achieve good signal-to-noise ratio under low exposure conditions has popularized their use in pediatric interventional radiology in the past decade, and several studies investigating these newer generation FPDs have been promising. 21 –23 In one such study, Miraglia and colleagues. performed biliary procedures in pediatric patients after liver transplantation on CII- and FPD-based fixed angiographic units. These authors found that the FPD system was associated with a lower dose area product (DAP) in each category of procedures: percutaneous transhepatic cholangiogram with biliary catheter placement (21.6 Gy cm2 vs 30.89 Gy cm2), cholangiogram with balloon dilation (10.13 Gy cm2 vs 10.38 Gy cm2), and cholangiogram with catheter removal (5.89 Gy cm2 vs 10.38 Gy cm2). The same group confirmed these findings in 96 children undergoing fluoroscopic central venous catheter placement using FPD- or CII-based fixed angiographic systems. Mean DAP with FPD was 15.9 Gy cm2 vs 113.5 Gy cm2 with CII for nontunneled catheter placements and 37.1 Gy cm2 vs 84.6 Gy cm2 for tunneled catheter placements. Dose reduction was also demonstrated by Weis et al. who compared FPD vs CII in a phantom study as well as in a separate analysis comparing the two technologies in age-matched patients who underwent voiding cystourethrograms and upper gastrointestinal studies. 23
Our study additionally demonstrated that FPDs produced higher image quality when compared with CII using paired line phantoms, which is in agreement with prior data favoring FPDs in quality of image. 23 –25 Bogaert and colleagues. showed that the use of FPD increased image quality by intrinsic better performance with no difference in radiation dose in cardiac procedures. 25 Two other studies demonstrated better image quality at lower radiation doses using FPDs. 23,26 This may be useful to the urologist in identifying smaller residual stones or details of a pyelogram with abnormal anatomy, but image quality was not specifically examined in the clinical portion of our study.
DAP is higher in the FPD group, the only measure of exposure which is greater. DAP is the measure of dose times the exposed area, and given that dose is so much lower, this discrepancy implies we had exposed a broader area in the FPD group. The FPD is quite large, a square with 26.2 cm sides, and provides a field of view 66% larger than the comparable CII. This suggests that if we were to have collimated more with the FPD, using a field of view closer to that of the CII, then the FPD exposure would be even lower than already reported. This is an opportunity for quality improvement. Dose estimates using DAP would be expected to be less accurate than those expressed in accumulated reference point air kerma in mGy, given the pediatric size of patients and differences in collimation. 27
Groups have investigated whether it is possible to eliminate fluoroscopy from URS altogether. Effective ultrasound-guided URS has been well documented in adults and Morrison and colleagues. have shown promising results in a small sample of children. 28 It is worth noting that ultrasound imaging of the mid-ureter is limited by the iliac ala and bowel, a second provider is typically needed to perform the ultrasound, and stenting may be challenging. Other groups have gone as far as performing URS without any form of imaging other than what is seen through the ureteroscope and tactile sensation of the instruments in the hand. 29 However, the authors excluded many cases in which use of fluoroscopy was considered necessary to perform the procedure safely due to anatomic concerns or the surgeon's judgment. It is our opinion that the safety afforded by fluoroscopy justifies its addition to URS.
There are several limitations in this study. The study is retrospective, and there may be differences in collimation and other aspects of c-arm use that are not captured. We expected most surgeon-induced variation to be in the form of fluoroscopy time and, reassuringly, the primary outcome of absorbed dose did not differ with respect to fluoroscopy time. Although the groups are of modest size and appear matched with respect to clinical characteristics and stone complexity, there may be subtle differences that impact dosimetry. We did not measure fluoroscope position and patient A-P thickness, and so calculation of more precise measures of exposure such as entrance surface air kerma is not possible, as might have been possible in a prospective study. We instead used values obtained from our C-arms to calculate DAP and reference point air kerma as surrogate measurements, and the compliant tolerance of their accuracy is as high as ±35%. Although the groups are small, the effect size is so tremendous that the probability of chance alone producing such an effect size is negligible, as reflected in the p-values, and it is doubtful that a larger cohort would substantially change the effect estimate. We also lack operator-focused dosimetry, but assuming similar distances from the source, dose would be expected to be reduced for both patient and operator with FPD. Our clinical and bench findings reflect units from only a single manufacturer. As image processing is a critical aspect of FPDs, it is likely that there are both software and hardware components specific to each company that impact image quality and dose. Every major manufacturer now has at least one FPD c-arm offering (GE: OEC Elite FPD, OEC One FPD; Siemens: Cios Alpha; Ziehm: Vision RFD). There is a physical limitation in that the head of the FPD is rectangular, and although far thinner, it is generally slightly broader than a cylindrical CII. It, therefore, fits less easily between the patient's knees in lithotomy position. Relaxing the lithotomy position helps. We did not have trouble imaging the bladder in our patients, but the operator should be more conscious of where potential patient contact points may lie when moving the larger and wider head of the unit.
The final limitation does not affect the data itself, but pertains to cost. FPD c-arms cost approximately two to three times more than their CII counterparts at the time of this submission. Although costs may fall in the future, this capital expenditure may not be within reach of all centers. Although FPD c-arms are more expensive, they are less subject to degradation than CII c-arms, and over time this degradation in efficiency may lead to higher radiation doses to achieve acceptable image quality. 30 In addition, FPDs are expected to have a longer lifetime and fewer repairs required based on the solid-state nature of its critical components and the flat panel's less complex structure, and so cost considerations should be amortized with this in mind.
Conclusion
This is the first study comparing CII and FPD c-arms in adult or pediatric URS. FPD c-arms are associated with dramatically lower radiation dose, with patients imaged using FPDs being exposed to less than a quarter of the dose compared with the traditional CII. In addition, direct comparison shows substantially higher image quality for FPDs, even at lower doses. Although the components are more complex and the purchase cost is higher, FPDs should be considered part of a comprehensive ALARA strategy for URS.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.