
Abstract
The gold standard surgical treatment for muscle invasive bladder cancer is radical cystectomy and urinary diversion. This procedure has historically been performed as an open surgery. With the advances of robotic surgery, robotic cystectomy and urinary diversion has gained popularity with the ability to perform intracorporeal urinary diversions in addition to extirpative surgery. Herein, we detail our technique for intracorporeal ileal conduit.
Featured Video
https://stream.cadmore.media/player/0298a47b-ec57-4347-abea-0d0d126e2674

Indications
An intracorporeal ileal conduit is indicated in instances where a urinary diversion is desired. Although this procedure is usually performed in combination with radical cystectomy for oncologic purposes, urinary diversion is also indicated in dysfunctional bladders. This can be a result of persistent bleeding, obstructed ureters, poor compliance with upper tract deterioration, recurrent infections, and inadequate storage with urinary incontinence. 1
Preoperative Preparation
The patient's fitness for general anesthesia and surgery is evaluated, and patients may visit with various consultants for risk stratification and optimization. All patients see a stoma therapy nurse preoperatively for stoma site marking and additional education. Reference materials are provided regarding diversion types and patients are encouraged to attend support group meetings in advance of surgery. These visits are best performed before the day of surgery to both ease patient anxiety and allow adequate time for understanding.
At our institution, enhanced recovery after surgery (ERAS) protocols are employed, wherein patients are encouraged to consume a high-protein diet leading up to the day of surgery. A high-protein high-carbohydrate supplement is recommended on the night before and the morning of surgery. 2 Patients continue a normal diet until the night before surgery and are kept with nothing by mouth after midnight. No mechanical bowel preparation is used. 3,4
The μ-opioid receptor antagonist alvimopan is administered 1 hour before surgery. Patients also receive a combination of oral non-narcotic pain medications, including gabapentin, acetaminophen, and celecoxib, with dose adjustments made for age or comorbidities. A broad-spectrum antibiotic (second-generation cephalosporin) is administered intravenously as well. Some surgeons may choose to add antifungal coverage in patients with diabetes. In addition to sequential compression devices (SCDs), patients will receive 5000 units of subcutaneous heparin upon induction of anesthesia. 5 An orogastric tube is placed intraoperatively and removed at the conclusion of the procedure.
Patient Positioning
Patients are initially positioned on a nonskid foam pad in the supine position for induction of general anesthesia and endotracheal tube placement. SCDs are placed on the lower extremities and the patient is placed in a low lithotomy position with arms tucked and all pressure points and joints padded with foam. A warming blanket is applied to the upper body just above the rib line. An alcohol-based prep is used to prep entirety of the abdomen from just above the xiphoid to the mid-thighs, including genitalia. In female patients, betadine or chlorhexidine is used for vaginal prepping.
Surgical Steps
Port placement
Initial access into the abdominal cavity is obtained approximately four fingerbreadths (6–7 cm) above the umbilicus in the midline using a Mini Port™ 2 mm Introducer (Covidien, New Haven, CT). Pneumoperitoneum is established to a pressure of 15 mm Hg, and if using Xi, an 8-mm robotic port is placed at this site (12-mm port if using Si). This will be the site of the robotic camera. The peritoneal cavity is now inspected for access injury and adhesions. Other ports are now placed for a six-port configuration: four robotic ports, one 12-mm Airseal assistant port (CONMED, Utica, NY), and one 15-mm assistant port (Fig. 1). The three additional robotic ports are placed in one line, about two to three fingerbreadths cephalad to the umbilicus. It is important to place the right-sided robotic ports supraumbilical to facilitate bowel work during the intracorporeal diversion. A 12-mm Airseal continuous insufflation assistant port is placed in the left upper quadrant just caudal to the left costal margin. The 15-mm assistant port is placed at the horizontal level of the umbilicus just medial to the left anterior axillary line. A suture passer device is used to preplace fascial closing sutures in each of these assistant ports for simple closure at the conclusion of the procedure. The patient is placed in steep Trendelenburg position before robot docking.
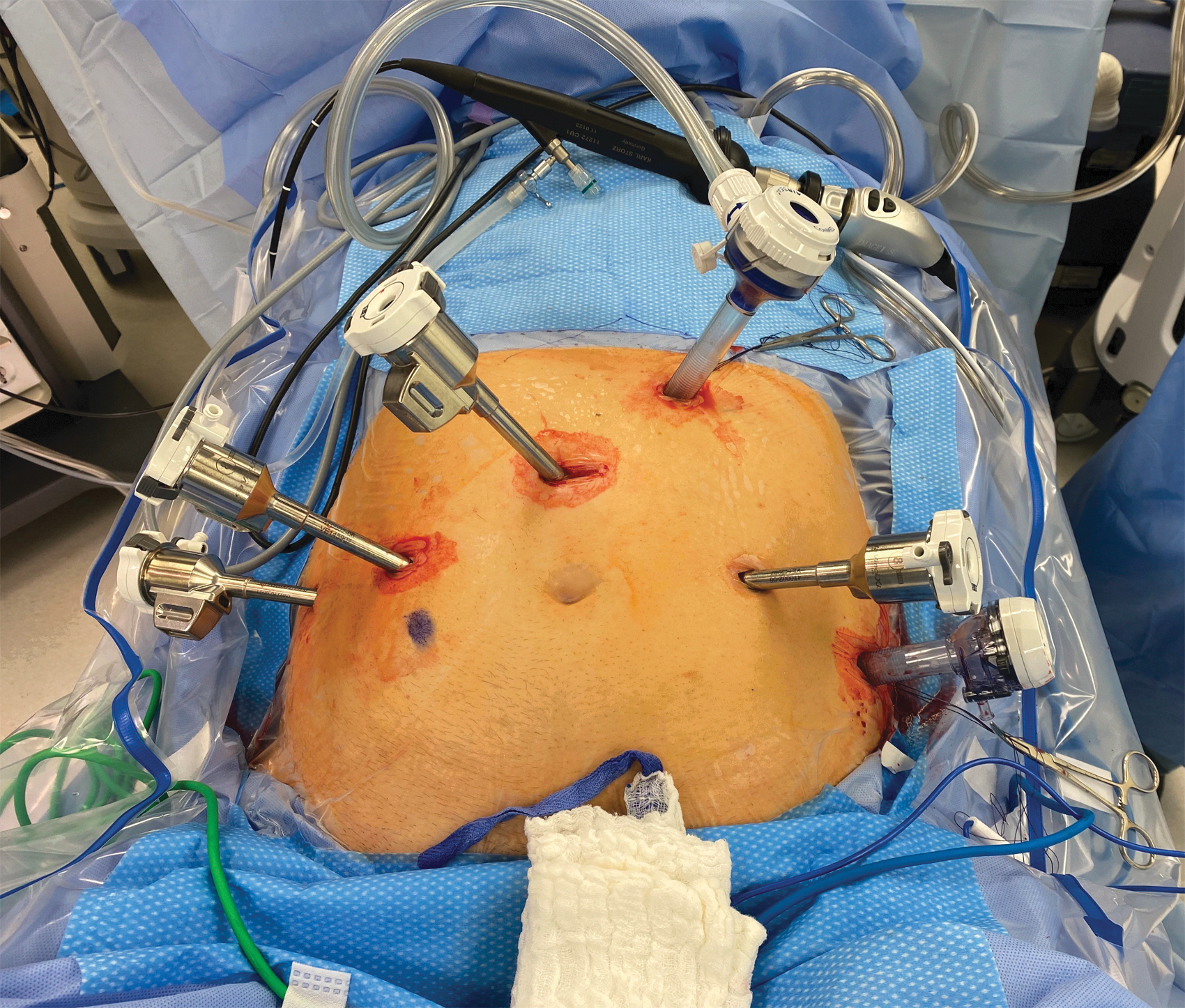
Port placement.
Radical cystectomy with bilateral extended pelvic lymphadenectomy
The technique for the extirpative portion of the procedure at our institution has been previously described. 6 Some modifications have been made in recent years, including use of the robotic vessel sealer in place of the endoscopic stapler for pedicle control in non-nerve sparing cases.
Distal ileal division and formation of the conduit segment
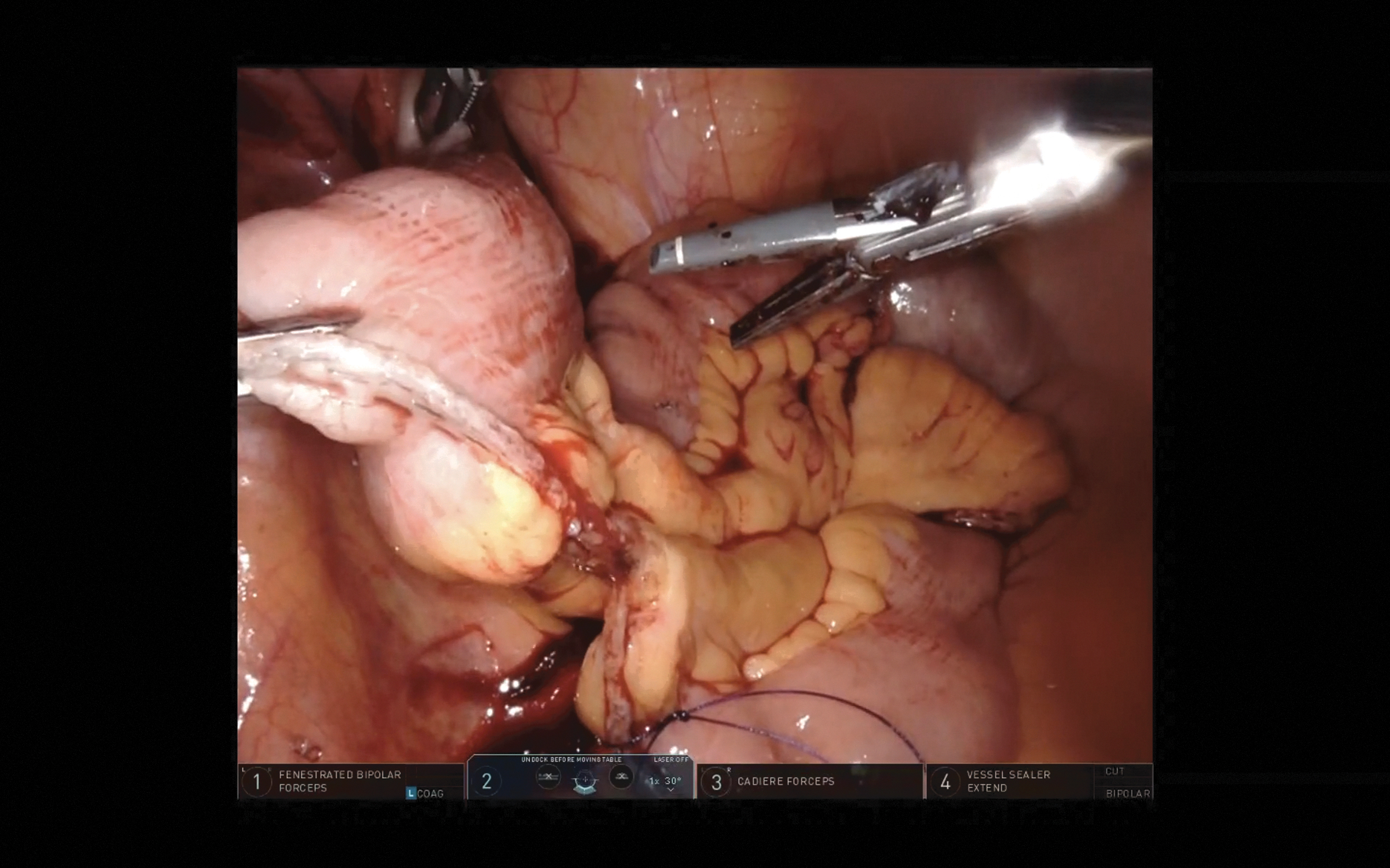
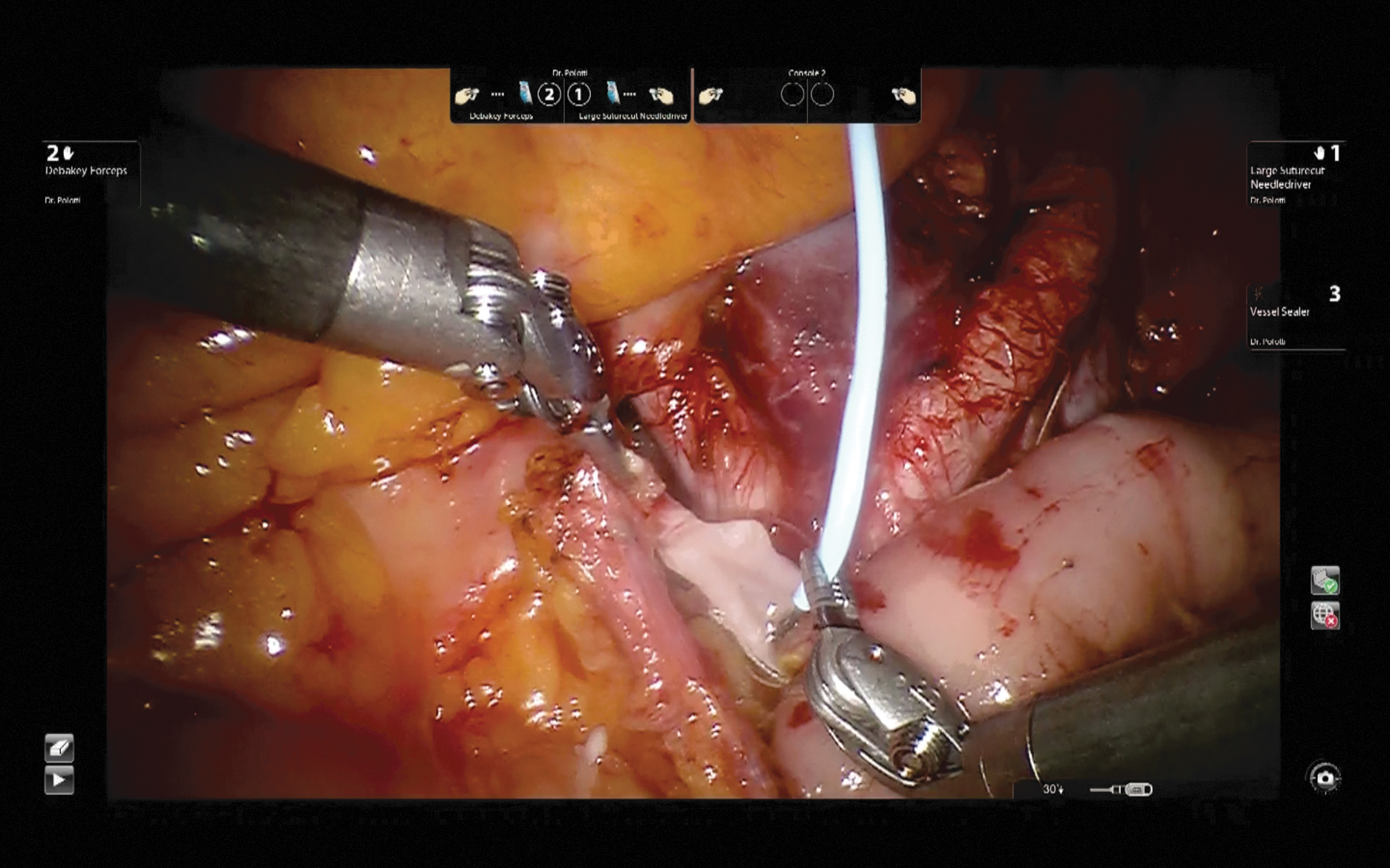
A Cadiere forceps is used in the right arm, fenestrated bipolar forceps is placed in the left robotic arm, and a vessel sealer is placed in the fourth arm. The cecum and the terminal ileum are identified, and any interloop adhesions are carefully divided. The terminal ileum is divided ∼15 cm from the ileal-cecal junction using a 60-mm laparoscopic stapler with a blue 3.5 mm cartridge stapler load (Ethicon Endo-Surgery). This handheld powered stapler is brought in through the 15-mm assistant port and divides the small bowel and a portion of the mesentery (Fig. 2). As soon as the bowel is transected, a dyed (blue) 2-0 polyglactin tagging suture is placed on the mesenteric border of the distal ileum to mark the end that will be used in the planned side-to-side bowel anastomosis. Next, a vascular staple load (white 2.5-mm cartridge) is used to deepen the mesenteric defect to allow for distal (stomal end) mobility for the conduit. When the distal bowel and mesenteric division is complete, a 15-cm conduit segment is measured proximally from the distal division, and the bowel is divided at this point using a 60-mm laparoscopic stapler with a blue load. Surgeons may choose to use a marked Penrose drain or umbilical tape to assist with bowel measurement.

Distal ileal division.
Discard segment
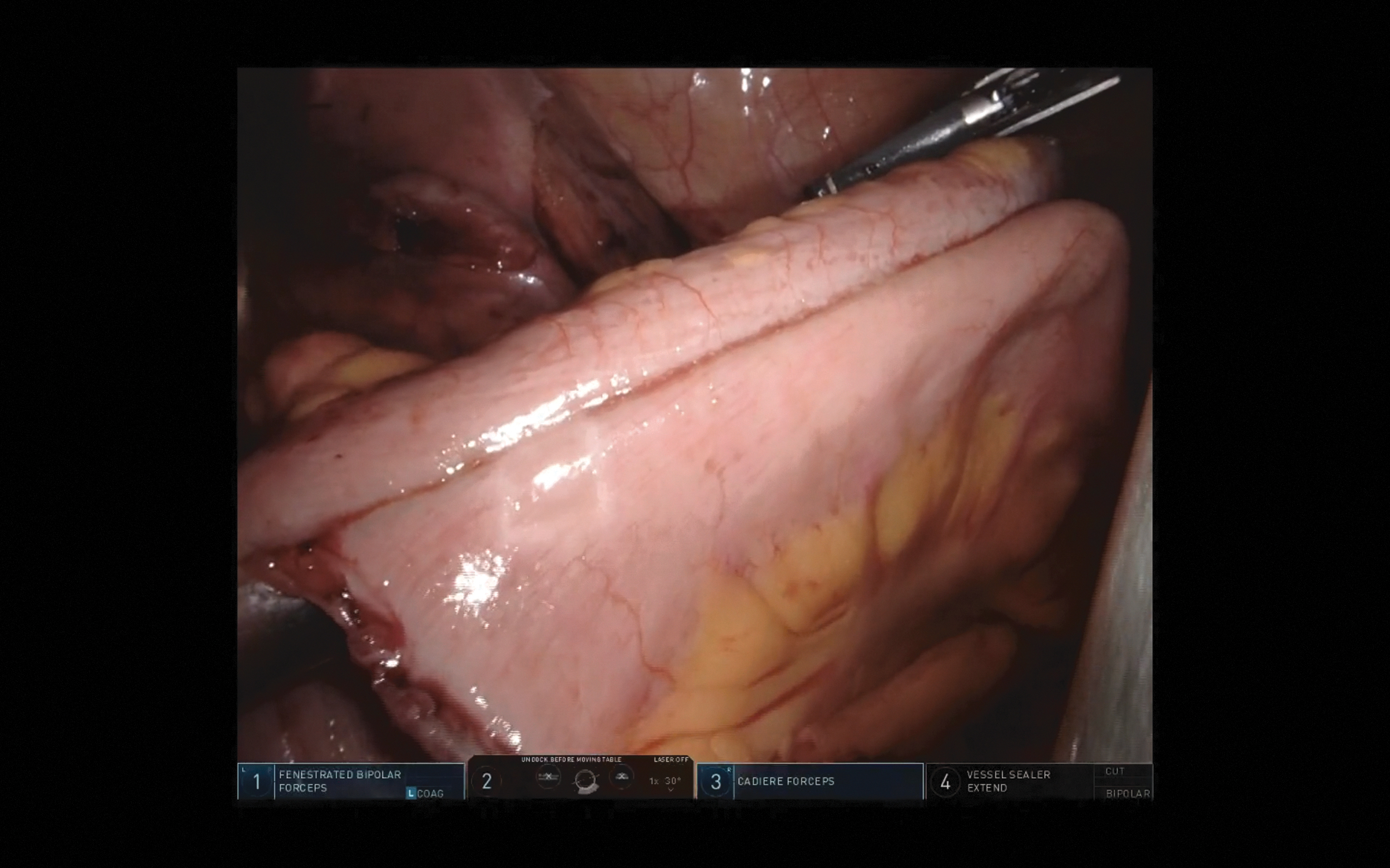
A 5-cm segment of small bowel, proximal to the proximal end of the conduit, is removed as the discard segment to achieve further conduit mobilization without the need to deepen the mesenteric defect in this area. A blue stapler load is used to divide the bowel discard segment, this time through the 12-mm upper assistant port. As soon as this bowel division is performed, another dyed (blue) 2-0 polyglactin tagging suture is placed on the mesenteric border of the proximal ileum, allowing easy identification of the ends to be used in the ileal-ileal anastomosis. The mesentery of the discard segment is divided using the vessel sealer just along the edge of the bowel, preserving as much mesentery as possible (Fig. 3). The discard segment is removed through the 15-mm port using laparoscopic spoon forceps.
Discard segment.
Ileal-ileal anastomosis
It is important to ensure the ileal-ileal anastomosis is completed anteriorly to the conduit segment for proper anatomic configuration. The conduit segment is dropped caudally toward the pelvis and an opening is made in the antimesenteric ends of the staple line of the bowel ends marked by the dyed sutures. The right arm is then switched back to the Cadiere forceps. The laparoscopic stapler with a blue load is advanced through the 15-mm port. The jaws are opened and the stapler is held steady. The surgeon uses the dyed stay sutures to guide the two ends of the bowel on to the separate jaws of the stapler. The surgeon ensures that there is no mesentery or extraneous bowel segments caught in the staple line and that there is no twisting of the bowel segments (Fig. 4). Another blue load of the stapler is used to extend the side-to-side anastomosis. The surgeon lifts the stapled bowel segments and a 60-mm laparoscopic stapler with a blue load from the 12-mm assistant port to staple the top and seal the side-to-side anastomosis. A complete staple line may require two staple loads. The excised bowel is removed with laparoscopic spoon forceps.
Ileal-ileal anastomosis.
Inspection with indocyanine green
12.5 mg of intravenous indocyanine green in 5 mL of sterile water is administered and fluorescence imaging with the Firefly function of the robotic system is used to confirm the vascular integrity of the ileal conduit, the distal ends of the ureters, and the ileal-ileal anastomosis (Fig. 5).
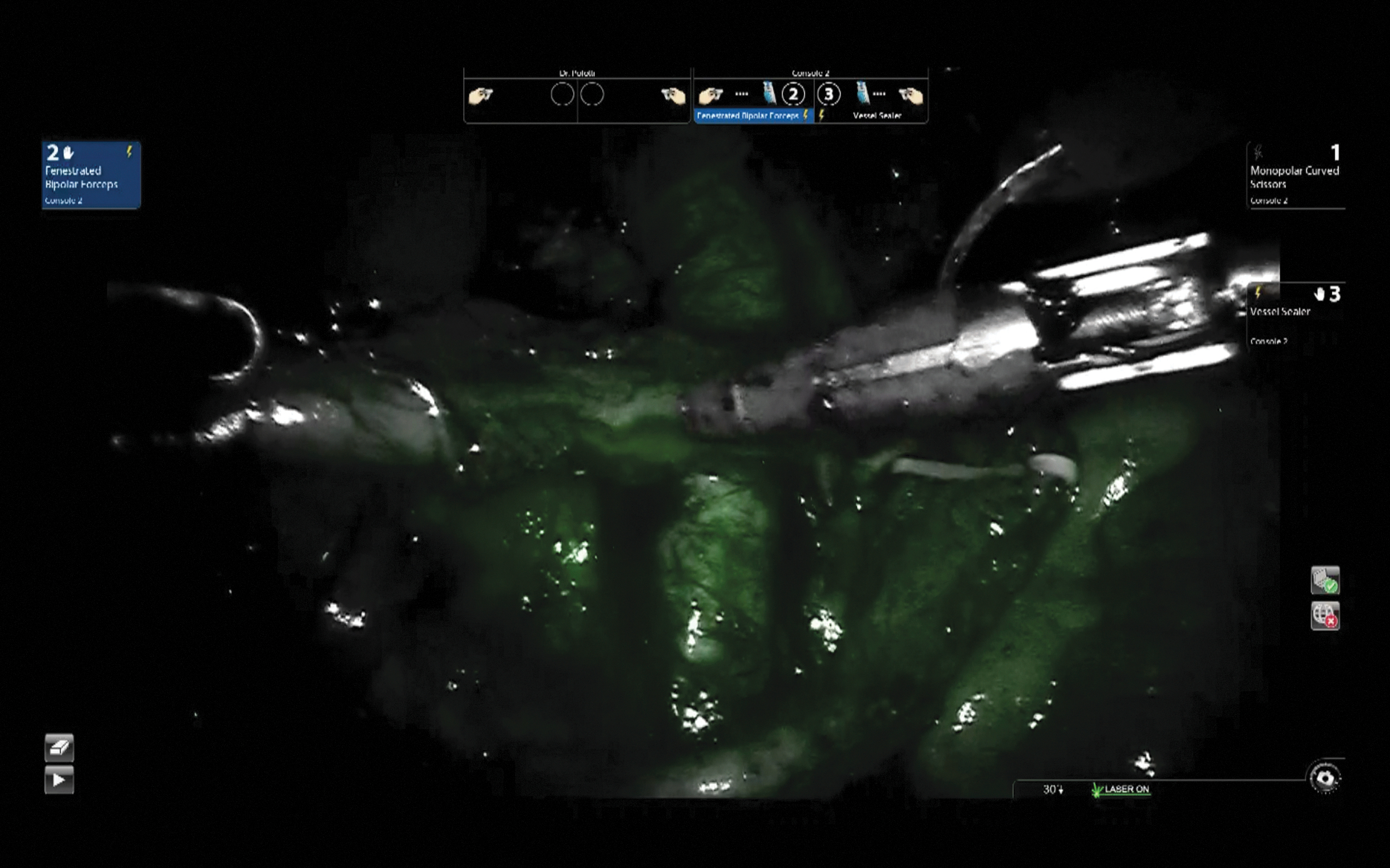
Inspection with indocyanine green.
Ureteroileal anastomosis and ureteral stent placement
In preparation for the ureteroileal anastomoses, a robotic Debakey forceps is placed in the left arm and a monopolar scissors is placed in the right arm. The left ureter is transposed to the right side under the sigmoid mesentery. The left ureter is anastomosed first. The ureter is transected partially with the scissors and periureteral tissue is cleaned proximally. The ureter is spatulated for 1 to 1.5 cm. An area on the proximal end of the conduit is selected for ureteral anastomosis and a small opening is made into the lumen of the conduit. A SutureCut needle driver is placed in the right arm to complete the anastomoses. The anastomosis is performed using a combination of interrupted and running 4-0 polyglactin sutures on a cutting needle. After completing the posterior wall with interrupted 4-0 polyglactin, a 6F Double-J stent intubated with a straight Glidewire is advanced through a Mini Port 2 mm Introducer placed in the suprapubic area (Fig. 6). After the stent is in place with the distal curl within the conduit, the excess distal ureter is completely transected and the anterior anastomosis is completed using a 4-0 polyglactin in a running manner. These steps are repeated for the right ureter. The proximal end of the conduit is then under sewn with a 3-0 V-Loc suture to exclude the staple line from contact with urine, decreasing the rate of stone formation. After pelvic drain placement, the stomal end of the conduit is exteriorized with the assistance of a laparoscopic locking Allis forceps through the previously marked stoma site. The abdomen is desufflated to reduce tension and a rosebud stoma is then created in the usual manner. A trimmed 18F red rubber catheter is placed into the conduit with the tip below the fascia and secured to the stoma with a 2-0 nylon suture.
Ureteroileal anastomosis.
Postoperative Care
The patient is then extubated at the conclusion of the procedure and the orogastric tube removed. Postoperative ERAS protocols are followed, which include alvimopan twice a day, several non-narcotic analgesic medications, gastrointestinal and deep vein thrombosis prophylaxis, early clear liquid diet, and early ambulation. Patients are continued on prophylactic antibiotic coverage. Body fluid analysis of creatinine from drain fluid is performed during the hospitalization. As patients progress toward discharge, midlines intravenous catheters are placed for home infusions of 1 L Lactated Ringer's every other day for 14 days to decrease risk of dehydration. The red rubber catheter may be removed before discharge and ureteral stents remain for up to 3 weeks.
Troubleshooting
A few points of troubleshooting are worth mentioning. Bleeding along a bowel or mesenteric staple line can be easily controlled with gentle monopolar or bipolar cautery. Generally, suturing is not necessary and may cause additional points of mesenteric bleeding. If the small bowel is difficult to work with and falls superiorly out of reach, it may be beneficial to undock the robot and reduce the angle of Trendelenburg to mitigate this issue.
In certain cases, the integrity of the ureter may necessitate removal of a longer distal segment. If there is concern for tension on the anastomosis or need to make up additional length, the ureters can be mobilized further proximally, using caution not to further compromise vascularity. In addition, anchoring sutures can be used between periureteral tissue and superficial mesenteric tissue to reduce tension. Similar technique can be applied to the proximal end of the ileal conduit to release tension.
List of Instruments
Robotic instruments
Monopolar scissors
Fenestrated bipolar forceps
Cadiere forceps × 2
Vessel sealer
Debakey forceps
SutureCut needle driver.
Disposable instruments
60-mm laparoscopic stapler
Blue (tissue) 3.5-mm staple cartridges
White (vascular) 2.5-mm staple cartridges.
Alternate or Modification of Technique If Applicable
Creation of an intracorporeal ileal conduit is also possible through use of the robotic stapler. In this method, a 12-mm robotic trocar would need to be used in the left lateral position to accommodate introduction of the stapler. Some surgeons may choose to use longer length stents for ease of stent removal and possible avoidance of looposcopy in the office setting. Finally, some surgeons choose to imbricate the ileal-ileal anastomotic staple line to seal the staple line away from adjacent bowel segments, possibly reducing adhesion or fistula formation.
Clinical Outcomes
Table 1 reports data from a few early case series 7 –9 first describing outcomes in patients who undergo intracorporeal ileal conduit urinary diversion.
Early Case Series Describing Intracorporeal Ileal Conduit
EBL = estimated blood loss; NR = not received; LOS = length of stay.
Footnotes
Patient Consent Statement
The author(s) have received and archived patient consent for video recording/publication in advance of video recording of procedure.
Recommended Videos from Videourology
1. Videourology 2020 Vol. 34, No. 3.
Simultaneous Perineal Urethrectomy and Robotic Radical Cystectomy with Extended Pelvic Lymph Node Dissection and Intracorporeal Ileal Conduit.
Stefan Jeglinschi, Imad Bentellis, Mathieu Carlier, Louis Denimal, Brannwel Tibi, Daniel Chevallier, Matthieu Durand, and Youness Ahallal.
2. Videourology 2021 Vol. 35, No. 4.
Single-Port Robot-Assisted Laparoscopic Radical Cystectomy with Intracorporeal Ileal Conduit.
Joshua K. Palka, Grant M. Henning, James T. Gross, and Eric H. Kim.
3. Videourology 2015 Vol. 29, No. 1.
A Simplified Approach to Intracorporeal Robot-Assisted Laparoscopic Ileal Conduit Formation.
Benjamin A. Sherer, Michael R. Farrell, and Leslie A. Deane.
Author Disclosure Statement
Dr. Mihir Desai has financial disclosures with PROCEPT BioRobotics (consultant) and Auris Surgical (consultant). The remaining authors have no disclosures. The remaining authors have no disclosures.
Funding Information
No funding was received for this article.