
Abstract
Background:
We present our series of free-hand transperineal prostate biopsy (fTP-Bx) using a novel coaxial needle introducer guide. All cases were performed in the office under local anesthesia (LA) without sedation. The majority received no prophylactic antibiotics.
Materials and Methods:
We retrospectively reviewed the electronic medical records of 242 consecutive fTP-Bx cases using the PrecisionPoint™ Transperineal Access System (PPTAS) performed under LA without sedation by a single urologist (R.J.S.) at Kaiser Permanente Southern California. We compared complication rates of this series of cases to our initial series of 62 fTP-Bx cases without the PrecisionPoint as well as 133 transrectal prostate biopsy cases performed before we adopted the transperineal approach.
Results:
Of the 242 consecutive free-hand transperineal biopsies performed between August 26, 2016 and December 31, 2018, 212 (88%) received no antibiotic prophylaxis. Medians for age, prostate-specific antigen, prostate volume, prostate-specific antigen density, and cores sampled were 63 years, 7.2 ng/mL, 50 mL, 0.15 ng/mL/cc, and 20 cores, respectively. Detection rates of overall and clinically significant prostate cancer averaged 43.4% (105/242) and 14% (35/242), respectively. Average visual analog scale pain rating was 3.9 and average procedure time was 20 minutes. Complication rates of sepsis, acute urinary retention, clot retention, and perianal abscess were 0.0% (0/242), 0.4% (1/242), 1.2% (3/242) and 0.4% (1/242), respectively.
Conclusions:
This series of office-based free-hand transperineal biopsy under LA without sedation performed with the PPTAS contains a large number of cases in which prophylactic antibiotics were not administered, yet there were no complications of postbiopsy sepsis. However, there was one case of a delayed perianal abscess. fTP-Bx under LA enables the easy integration of transperineal biopsy into a normal outpatient clinic workflow.
Introduction
In response to increasing rates of post-transrectal prostate biopsy (TR-Bx) sepsis 1 despite the use of empirical or targeted antibiotic prophylaxis, 2 the author switched to “free-hand” transperineal prostate biopsy (fTP-Bx) in 2015. This increasingly popular and flexible technique replaces the formerly used perineal grid template by using one hand for the ultrasound probe and the other hand for the biopsy-needle instrument, allowing urologists to incorporate the transperineal approach to prostate biopsy into the office setting.
Materials and Methods
Study Population
Between June 1, 2012 and December 31, 2018, one urologist at Kaiser Permanente Southern California performed 133 consecutive TR-Bx's, followed by 304 consecutive fTP-Bx's, all under local anesthesia (LA) without sedation. Although the urologist had experience in residency with transperineal finger-guided biopsy, he had no experience with grid techniques. Initial training for fTP-Bx utilized the study of online video demonstrations, after which the first 62 systematic fTP-Bx cases were performed under LA using a simple 15-gauge transperineal coaxial needle introducer. Then, after a 2 hour in-person training session with the PrecisionPoint™ Transperineal Access System (PPTAS) (Perineologic, Corbin Clinical Resources, LLC, Cumberland, MD) using LA on patients in the outpatient clinic, the urologist went on to perform the remaining 242 cases of systematic fTP-Bx under LA. In the latter group, 42 patients had additional cognitive MRI-fusion biopsies, while 6 had additional software-based MRI-fusion biopsies (Koelis Trinity™, Auburndale, MA). Indications for biopsy included initial screening, repeat biopsy for prior negative TR-Bx's, or active surveillance (AS). Only LA was offered to patients who agreed to undergo fTP-Bx. The rare patient who insisted on sedation or general anesthesia was referred to colleagues who did TR-Bx.
Patient preparation and antibiotic prophylaxis
After assuring a negative preprocedure urine culture, patients were required to self-administer a saline enema 2 hours before the biopsy to decrease the chance of perineal fecal contamination and help ensure a good ultrasound image. Empirical or targeted antibiotic prophylaxis was administered to the TR-Bx cases and the non-PPTAS fTP-Bx cases. However, no antibiotic prophylaxis was administered in the majority (88% [212/242]) of PPTAS fTP-Bx cases. The remaining cases (12% [30/242]) received intramuscular ceftriaxone or oral ciprofloxacin based on their individual risk factors.
Procedural details for fTP-Bx with PPTAS
Patients were placed in the dorsal lithotomy position on an examination table furnished with simple gynecologic heel stirrups in an outpatient clinic procedure room. After displacing the scrotum cephalad with tape and injecting 10 mL of 2% lidocaine gel into the rectum, the perineal skin was prepped with 10% povidone iodine solution. The PPTAS was then snapped onto a biplane transrectal ultrasound probe (Fig. 1). Five milliliters of 0.5% lidocaine mixed with 8.4% sodium bicarbonate solution in a 9:1 ratio was injected into the perineal skin 2 cm lateral to the midline raphe on either side at a point aligned midway between the posterior and anterior capsule of the prostate as guided by reference to the transverse plane ultrasound image. The 15-gauge hollow coaxial needle was placed in the lowest aperture of the PPTAS, and after switching to the sagittal plane ultrasound image for further guidance, a 22-gauge 7-inch spinal needle was inserted through the coaxial needle, keeping it in line with the biplane side fire ultrasound probe as it was guided toward the areas to be anesthetized. An additional 10 mL of the anesthetic solution was infiltrated into the ischiorectal fat, pelvic diaphragm, and periapical triangle. Although a larger volume of lidocaine was occasionally required, in no case did the dose surpass the standard maximum of 4.5 mg/kg (equal to 63 mL of 0.5% lidocaine in a 70 kg male) 3 and care was taken to lower the dose for thinner patients to avoid cardiotoxicity. The hollow coaxial needle was then slid forward on the PPTAS carriage and “popped” through the anesthetized perineal skin into the ischiorectal fat on the side to be biopsied. An 18-gauge × 20 cm Bard® Max-core® biopsy instrument was then passed through the coaxial needle introducer, using a “fan pattern” 4 to sample the posterior peripheral zone (which included the lateral horns), proximal basal peripheral zone and the anterior prostate (which included the fibromuscular stroma and transitional zone) (Fig. 2). Biopsy cores were spaced about 1 cm apart in sampling the peripheral and anterior zones and thus the number of biopsies varied with the size of the prostate. The procedure was repeated on the contralateral side.

fTP-Bx using PrecisionPoint™ Transperineal Access System. (Modified Screenshot from Instructional Video Courtesy of Perineologic, Corbin Clinical Resources, LLC, Cumberland, MD). fTP-Bx = free-hand transperineal prostate biopsy
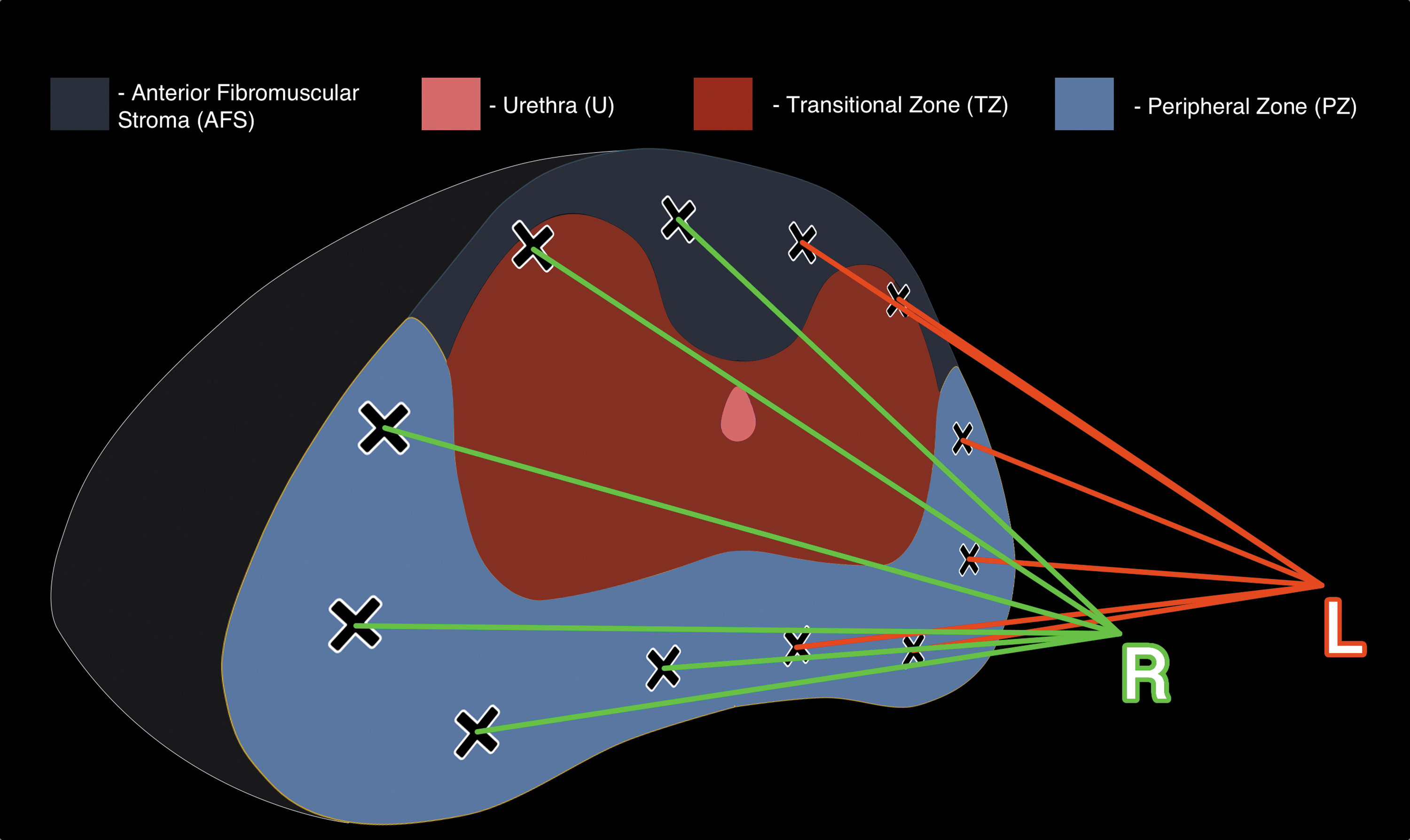
Template used for transperineal prostate biopsy with fan-pattern technique.
To access the anterior sectors of different-sized prostates, the coaxial needle introducer was repositioned into one of the four more anterior apertures of the PPTAS carriage to adjust the introducer's position relative to the ultrasound probe while reusing the same perineal puncture site used for the more posterior biopsy cores. (Instructional videos on fTP-Bx under LA with the PPTAS are readily available on the web at:
Pain ratings
Pain ratings were assessed by a nurse 5 minutes after the procedure on 169 of the last 172 consecutive patients in the series using a Visual Analog Scale (VAS) from 1 to 10. For the last 98 patients who had experienced prior TR-Bx's, the patient was also asked to assign a VAS pain rating for what he remembered of the prior TR-Bx experience.
Study outcomes and data collection
The primary outcome was cancer detection rate (CDR). Secondary outcomes included demographic data, antibiotic prophylaxis, procedural times, VAS pain rating, and complication rates. Institutional Review Board approval (No. 11438) was obtained for retrospective data analysis of outcomes collated by querying the Kaiser Permanente HealthConnect® electronic medical record for ICD-9 codes and order codes. We used chart reviews for compilation of demographic data, pathology results, antibiotic use, procedural times, and VAS pain ratings. We captured complications by reviewing the charts of all patients seen in the emergency department within 30 days after the prostate biopsy. Complications were then assigned a Clavien classification grade.
Statistical analysis
Continuous variables were analyzed with paired or unpaired two-tailed Student t-tests based on the sample origins. Nominal variables were analyzed by the chi-square with Yates correction test or Fisher exact test based on sample sizes. Statistical significance was considered at p < 0.05. All statistical analyses were performed with GraphPad Prism 8®.
Results
Our experience with fTP-Bx under LA: PPTAS group (n = 242)
Clinical and demographic information
The results discussed below pertain to the 242 cases of fTP-Bx under LA performed with the PPTAS unless otherwise specified (Table 1).
Baseline Clinical and Demographic Information
fTP-Bx = free-hand transperineal prostate biopsy; LA = local anesthesia; PPTAS = PrecisionPoint™ Transperineal Access System; PSA = prostate-specific antigen; TR-Bx = transrectal prostate biopsy.
The median values for age, prostate-specific antigen (PSA), prostate volume, PSA density, number of cores taken, volume of lidocaine, and procedural time were 63 years, 7.2 ng/mL, 50 mL, 0.15 ng/mL/cc, 20 cores, 30 mL, and 20 minutes, respectively.
Of the 242 fTP-Bx cases, 126 (52%) had a prior TR-Bx, 75 (31%) had a prior MRI, 48 (20%) had a PI-RADS ≥4 lesion on the MRI, and 25 (10%) were on AS. One hundred fifty (62%) were white, 38 (16%) were Hispanic, 36 (15%) were Asian, 6 (2%) were black, and 12 (5%) were listed as “other.”
VAS pain ratings
The average Visual Analog Scale (VAS) pain rating obtained at the end of the procedure from 169 of the last 172 consecutive patients was 3.9 (Table 2). The average VAS pain rating for the 98 patients with a history of TR-Bx was 4.1 for fTP-Bx and 4.6 for the prior TR-Bx (p = 0.0297).
Visual Analog Scale Pain Ratings
AS = active surveillance; VAS = Visual Analog Scale.
CDR: PPTAS group
For the 242 cases of fTP-Bx under LA with PPTAS, the CDR was 43.4% (105/242) for overall prostate cancer (PCa) and 14% (35/242) for clinically significant prostate cancer (csPCa) (Table 3). Anterior cancer was detected in 60% (63/105) of those with positive biopsies. In cases naive to prostate biopsy, the overall CDR was 51% (57/111). In cases with prior negative TR-Bxs, the overall CDR was 25% (24/97). Anterior cancer was found in 21% (20/97) of those with prior negative TR-Bx's, and 80% of the time (16/20) the cancer was located only in the anterior region.
Cancer Detection Rate and Pathology
Refers to overall PCa (≥GG1) unless otherwise specified.
csPCa = clinically significant prostate cancer; PCa = prostate cancer.
Of the 75 cases with a prebiopsy MRI, the overall CDR was 39% (29/75). Of the 48 cases that underwent cognitive and software MRI/US-TBx where the MRI demonstrated a PI-RADS 4 or 5 lesion, the overall CDR was 33% (16/48). Overall CDR for AS cases was 60% (15/25).
CDR: fTP-Bx under LA, coaxial needle introducer only group, and TR-Bx group
Compared to the CDR of the fTP-Bx PPTAS group, the overall CDR of the 62 cases of fTP-Bx's with coaxial needle introducer only (performed by the same urologist 2015 to 2016 before PPTAS FDA approval) was 32% (20/62) (p = 0.1476), while the overall CDR of the 133 cases of systematic 12-core TR-Bx's (performed by the same urologist 2012 to 2015) was 39% (52/133) (p = 0.4451) (Table 3).
Pathologic analysis: PPTAS group
Of the PCa's, 66.6% detected were grade group 1, whereas 19.0%, 3.8%, 1.9%, and 8.5% were grade groups 2, 3, 4, and 5, respectively (Table 3).
Complications presenting to emergency department: PPTAS group (Table 4)
The various complications are described in greater detail in Supplementary File A.
Complications
NR = not recorded.
Sepsis
There were no cases of postprostate biopsy sepsis (0% [0/242]).
Urinary retention and gross hematuria with clot retention
There was one case of urinary retention (0.4% [1/242]) (Clavien I) and three cases of clot retention (1.4% [3/242]) secondary to gross hematuria (two were Clavien I). One of the clot retention cases required clot evacuation with fulguration of an arterial bleeder in the distal prostatic urethra under GA (Clavien IIIb).
Delayed complication: perianal abscess (Fig. 3)
There was one case of a delayed perianal abscess in a 74-year-old male smoker who had diabetes mellitus. He was one of the 212 PPTAS patients (87.6% [212/242]) not given prophylactic antibiotics (Clavien IIIb).

Left perianal abscess (indicated by arrow) shown on computerized tomography of pelvis with intravenous contrast 5.7 weeks after fTP-Bx (ruler lines: A = 2.8 cm, B = 1.8 cm).
Complications presenting to emergency department: coaxial needle sheath group (n = 62)
Sepsis
There were no cases of postbiopsy sepsis (0% [0/62]).
Clot retention
There was one case of clot retention treated with Foley catheterization Clavien I).
Light headedness
There was one case of acute, moderate, intermittent lightheadedness during the biopsy, thought to have occurred after the patient received 20 mL of 1% lidocaine injection into the perineum (Clavien I).
Complications presenting to emergency department: TR-Bx (12 core systematic) under LA (n = 133) (3 years of TR-Bx's performed before the adoption of fTP-Bx)
Sepsis
There was one case (1/133 [0.075%]) of severe post-TR-Bx sepsis requiring a 2-month long hospital admission because of complications of necrotizing leukoencephalopathy, which resulted in permanent diffuse paresis and permanent severe cognitive impairment (Clavien IVb).
Discussion
CDR of overall PCa and csPCa
In this retrospective review of a single institution, single surgeon experience with fTP-Bx under LA with PPTAS, we found that our CDR for overall PCa was comparable to our TR-Bx CDR for overall PCa. However, our CDR for csPCa using fTP-Bx under LA with PPTAS was lower than that seen in several large series of fTP-Bx 5 –7 although higher than that seen in another large series of fTP-Bx. 8 The lower csPCA CDR is likely due to selection bias since 25% of our fTP-Bx's were referrals from other urologists of patients with prior negative TR-Bx's, often with low PSA densities. Indeed, our median PSA density was only 0.15.
VAS pain rating
The average VAS pain rating was 3.9 for 169 cases. In addition, the VAS pain rating for 98 fTP-Bx patients who had already had a prior TR-Bx procedure was 4.1 for their fTP-Bx procedure and 4.6 for what these patients remembered of their prior TR-Bx (p = 0.0297). Although these pain ratings are higher than other average VAS pain ratings among several large series of fTP-Bx under LA in the literature, 5,6,9 it should be noted that we used a VAS between 1 and 10, not the 0 to 10 used by similar studies, and this may have artificially elevated the final ratings compared to ratings found in the literature. The use of 0.5% lidocaine instead of the 1% to 2% lidocaine used in the other large series 5,6,9 may have also contributed to causing the higher average rating.
Procedural times
Our average procedural time for fTP-Bx is slightly longer than average procedural times in other large series of fTP-Bx. 5 –7 This may be due to the greater average number of cores we took and the larger average volume of anesthetic we injected.
Sepsis
There were no cases of postbiopsy sepsis among the first 62 coaxial needle sheath fTP-Bx's. Likewise, there were no cases of postbiopsy sepsis among the 242 PPTAS fTP-Bx's even though 88% of these latter patients received no antibiotic prophylaxis. The absence of sepsis complications despite the avoidance of antibiotic prophylaxis in most of these patients contrasts with the one case of severe sepsis among the 133 TR-Bx's performed with antibiotic prophylaxis in the 3 years before our switch to fTP-Bx. Although this difference in postbiopsy sepsis rate is not statistically significant (p = 0.3547), the sample sizes are relatively small. Indeed, the incidence of post-TR-Bx sepsis ranges between 1% and 3% in the literature 10 and reviews of population databases also indicate that transperineal biopsy patients experience substantially fewer cases of sepsis than TR-Bx patients. 11,12
However, because there was one case of a Bacteroides fragilis perianal abscess in our fTP-Bx series, we must consider whether systemic prophylaxis for anaerobic bowel flora is indicated for fTP-Bx. Although, to the best of our knowledge, no other cases of perianal abscess after fTP-Bx have been published to date, 13 several cases of perineal abscesses have been reported after transperineal injection of the SpaceOAR™ Hydrogel System. 14 It is therefore likely that either a puncture of the rectal wall or contamination of the perineum by rectal bacteria was responsible for this complication. More studies with larger case series are required to determine if the benefit of administering antibiotic prophylaxis to try to prevent a rare, nonlife-threatening complication (perianal abscess) outweighs the risk of an allergic reaction to prophylactic antibiotics since the latter complication is much more common 15 and can be more dangerous. 16 Nevertheless, the virtual elimination of life-threatening postbiopsy sepsis, 11,17 with or without the use of prophylactic antibiotics, is a significant advantage of the transperineal approach.
Limitations of our study
This study is a retrospective review of the experience of a single surgeon in a single institution. The sample size was relatively small and the indications for prostate biopsy were mixed. The cohort contained patients with elevated PSA's who were referred for their second and third biopsy due to prior negative prostate biopsies. These patients often had large prostates and low PSA densities, likely diminishing the CDR for csPCA compared to other studies in the literature. Finally, comparing immediate post-fTP-BX pain ratings to pain ratings based on memories of pain experienced during prior TR-Bx's may invoke recall bias.
Conclusion
This retrospective study contains a large number of cases of fTP-Bx with PPTAS under LA without sedation, in which antimicrobial prophylaxis was not administered. Yet, despite the avoidance of prophylaxis in 212 of 242 cases, postbiopsy sepsis did not occur, attesting to the safety of the transperineal approach when compared to TR-Bx. However, the one case of delayed perianal abscess (the first time this complication has been reported in the literature for fTP-Bx) highlights the need for careful attention to the rectal wall during the fTP-Bx procedure as well as the need to avoid fecal contamination of the perineum during the procedure. Given the rarity of perianal abscess after fTP-Bx and the localized nature of this infectious complication, it is not yet known if the merits of prophylactic antibiotics outweigh their disadvantages when considering the transperineal approach.
Footnotes
Acknowledgments
Ingrid Rosenthal developed the clarity report spreadsheets from the HealthConnect™ database, and Jiaxiao M Shi, PhD provided statistical analysis advice.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
Southern California Kaiser Permanente provided database service and statistical advice.
Supplementary Material
Supplementary File A
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.