
Abstract
Objective:
To investigate the efficiency of three advanced lithotripters during the treatment of artificial stones (hard and soft) in an experimental in vitro and in vivo setting.
Materials and Methods:
An experimental configuration was created to treat artificial stones, made from BegoStone Plus in a weight ratio of 15:3 or 15:6 powder to water, replicating hard and soft urinary stones, respectively. Experimental data of three lithotripters, the Lithoclast Master, the Lithoclast Trilogy, and the ShockPulse-SE, were assessed. Experiments aimed at comparing the stone clearance times (SCTs) of the devices as well as different probe diameters, probe disposability, and hardness of the stones. The in vivo experiment was performed in a porcine model after the approval from the State Services. Before in vivo lithotripsy, stones had been placed through percutaneous access established by using the Bull's eye technique. The SCT between the Lithoclast Trilogy and the ShockPulse-SE was compared.
Results:
All the devices were statistically more efficient in the treatment of soft stones in both in vitro (p < 0.001) and in vivo settings (p < 0.008). The use of larger-diameter probes resulted in shorter SCT (p < 0.007). The disposable probes of the ShockPulse-SE showed higher performance than the multiple-use probes (p < 0.05). In the direct comparison between the devices, the Lithoclast Trilogy was found to be the fastest during all the in vitro (p < 0.001) and in vivo (p < 0.008) trials.
Conclusion:
Modern dual
Introduction
Percutaneous nephrolithotomy (PCNL) is the preferred choice of treatment for renal stones ≥2 cm. Technological advancements provided the urologists with a variety of lithotripters with improved efficacy and safety along with faster stone clearance and lower complication rates. 1,2
Recently, the ultrasonic lithotripter such as the Lithoclast® Master (EMS Medical, Nyon, Switzerland) has gained popularity for easier stone fragmentation. Two new-generation lithotripters, available in the market, are the Lithoclast Trilogy (EMS Medical) and the ShockPulse-SE™ (Olympus, Tokyo, Japan) single-probe, dual-energy devices that combine ballistic and ultrasonic energy with integrated suction. This combination provides better evacuation of the generated fragments and limits their further spillage. 3,4
Despite the wide acceptance and use of these devices in urological practice, there is a lack of comparative evidence in the literature. 5 Therefore, the aim of the current study was to investigate the efficiency of three advanced lithotripters (the Lithoclast Master, the Lithoclast Trilogy, and the ShockPulse-SE) for the treatment of artificial stones of two compositions, using different diameters of probes, in an experimental in vitro and in vivo setting.
Materials and Methods
Artificial stones were made from BegoStone Plus (Bremen, Germany) in a weight ratio of 15:3 or 15:6 powder to water, resembling the physical properties of hard and soft stones, respectively. 6 To minimize any discrepancy, all stones were made in a standardized manner, possessing the same 1.9 cm size, 0.7 cm3 volume, and 1500 or 1000 mg weight for hard and soft stones, respectively.
In vitro experiment
An experimental configuration was created by using a clear polyvinyl chloride (PVC) tube 30 cm long, closed on one end and fixed on a solid wooden base, 20°angled, inside a box filled with 0.9% saline solution.
Each stone, soaked for 30 minutes before each trial, was placed inside the PVC tube. The experiment was performed by using one lithotripter at a time (the Lithoclast Master, the Lithoclast Trilogy, or the ShockPulse-SE) inserted through an 18F nephroscope in the PVC tube. The test was over when complete stone clearance was achieved (Fig. 1). The suction was kept constant for all trials: Each lithotripter was pretested and set to a suction power of 800 cc/minute. To achieve the best efficiency, for each device, the most powerful setting in terms of energy was used. Several probes with different diameters were tested: 9.9F (3.3 mm) and 11.4F (3.8 mm) multiple-use probes for the Lithoclast Master; 3.4 and 3.9 mm disposable probes for the Lithoclast Trilogy; and 3.4 and 3.76 mm, both disposable and of multiple use, for the ShockPulse-SE. The probe, handpiece, and suction tubing were cleared of fragments between each trial to avoid obstruction.

Artificial setting and devices:
Stone clearance time (SCT), defined as the time until complete fragmentation and evacuation of the stone, was recorded. Each device was used to treat 20 stones (10 soft and 10 hard stones).
Evaluated parameters
- SCT for each lithotripter,
- Comparison in the SCT for each device according to:
diameter of the probes (small/big),
composition of the stones (hard/soft),
disposability of the probes (single/multiple-use probes, available only for the Olympus ShockPulse-SE)
- Comparison in the SCT between the three devices according to:
diameter of the probe,
composition of the stones,
For a better comparison between devices, we compared only single-use probes.
In vivo experiment on porcine model
Animals and surgical technique
Aiming at testing the reliability of the in vitro findings, experiments in an in vivo porcine model were performed. Female pigs, weighing more than 30 kg, were involved after the approval from the Veterinary State Services.
Anesthesia
The procedure was performed under general anesthesia. Premedication using a combination of Ketamine (5 mg/kg) and Xylazine (1 mg/kg) was injected intramuscularly. The pig was placed in a supine position, simulating a lithotomy position. Auricular venous access was preferred for the induction and maintenance of the anesthesia with Propofol. Mechanical ventilation through an endotracheal tube was available throughout the whole procedure.
Placement of ureteral catheter
In the lithotomy position, a ureteral catheter (Occlusion Balloon Catheter by Boston Scientific) was placed endoscopically in each kidney, with the balloon occluding the ureteropelvic junction to prevent fragments from migrating down the ureter during lithotripsy (Fig. 2A, B).
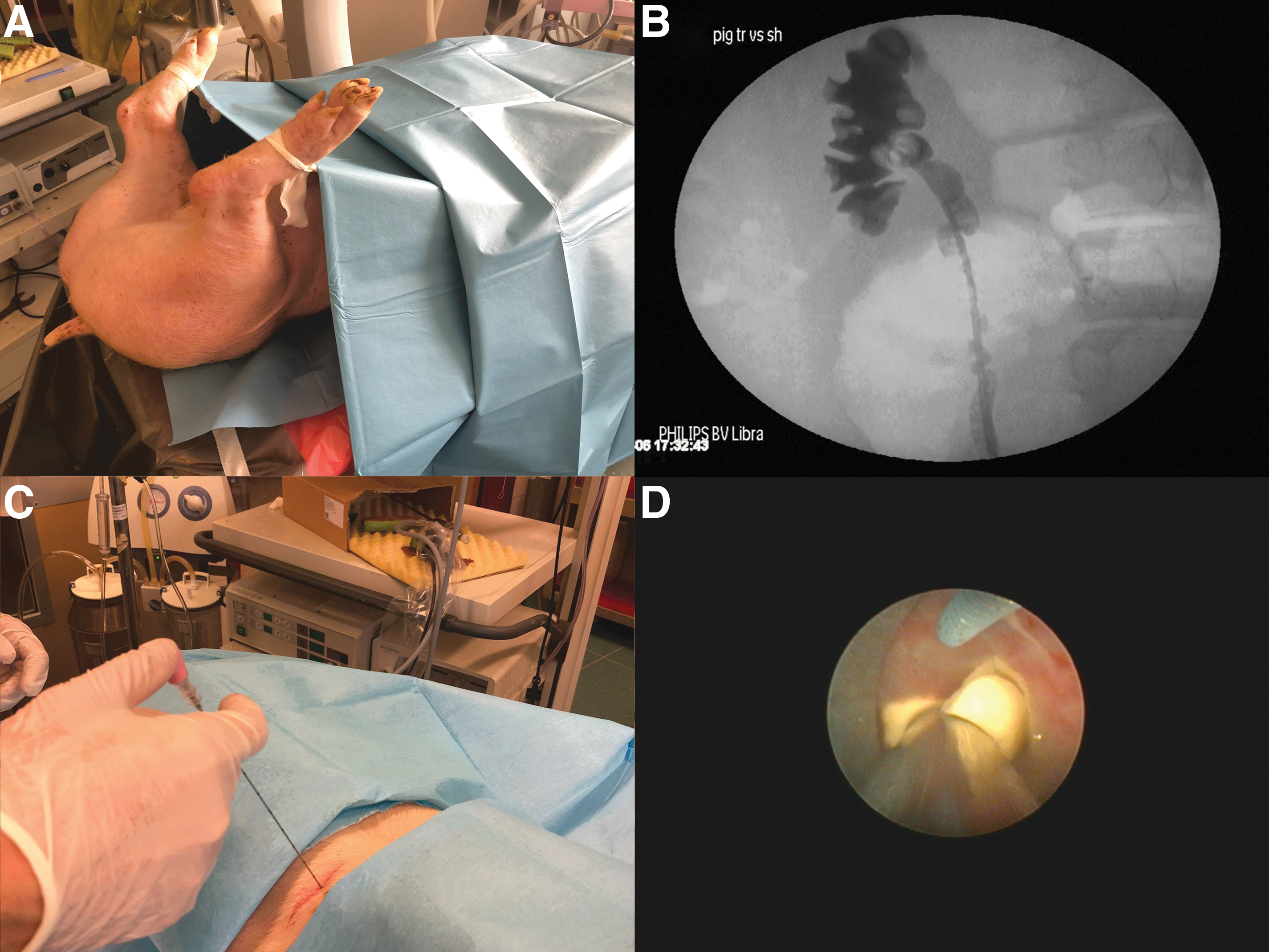
Positions of the pig and percutaneous puncture.
Puncture
In a prone position, a fully fluoroscopic bi-planer puncture technique (Bull's eye technique) was performed. The puncture site was identified under fluoroscopic guidance, placing the C-arm perpendicular to the long axis of the pig, at 20°. Through a specific rotational movement typical of the Bull's eye technique, an 18-gauge trocar needle was introduced and advanced parallel to the C-arm to get closer to the target (Fig. 2C). The depth of the penetration was controlled with the C-arm set at 0°. 7 A 0.035″ hydrophilic guidewire was then introduced and directed down into the ureter.
Tract dilation
The hydrophilic guidewire was exchanged for a stiff guidewire, utilizing an 8F dilator. Tract dilation was performed in two steps by utilizing 16F and 24F Amplatz dilators. Thereafter, a 24F Amplatz sheath was introduced over the last dilator under fluoroscopic guidance. 7
Artificial stone placement and lithotripsy
Artificial stones were introduced in the renal pelvis through the same access sheath. As an inclusion objective for the in vivo part, the two fastest lithotripters according to the results of in vitro experiment were selected: the Lithoclast Trilogy or the ShockPulse-SE.
One by one, stones were introduced through an 18F nephroscope, and they were treated interchangeably by using one lithotripter at a time (Fig. 2D). To minimize the discrepancies, the 3.4 mm disposable probes (small probes) were used for both devices.
To keep the pig alive after the experiment, only one kidney was used with a maximum of five stones treated during each experimental session.
The SCT were recorded. Each device was used to treat 10 stones (5 soft and 5 hard stones).
Evaluated parameters
SCT for each lithotripter,
Comparison in SCT between hard and soft stones for each device,
Comparison in SCT between the two devices.
Data analysis
The statistical evaluation was performed by using the software IBM SPSS version20 (IBM Corp., Armonk, NY). Continuous variables were described by using medians and interquartile ranges (IQRs). The values for SCT were compared with the Mann–Whitney U test. A p-value <0.05 was considered statistically significant for all the comparisons.
Results
In vitro experiment
A total number of 160 experiments were performed, including 80 hard and 80 soft stones.
Clearance time for each device
The median SCT with the small diameter probe (9.9F–3.3 mm) of the Lithoclast Master was 48.2 seconds (IQR 44.8–52.9) for hard stones and 26.1 seconds (IQR 23.5–27.0) for soft stones. The respective numbers for the large diameter probe (11.4F–3.8 mm) were 46.1 seconds (IQR 44.2–47.4) for hard stones and 21.1 seconds (IQR 20.5–21.1) for soft stones.
Using the Lithoclast Trilogy, the SCT with the small diameter probe (3.4 mm) was 34.9 seconds (IQR 30.8–38.7) for hard stones and 12.2 seconds (IQR 10.9–13.6) for soft stones. A faster median SCT for both hard (17.5 seconds [IQR 15.8–18.3]) and soft (7.4 seconds [IQR 6.3–8.6]) stones was observed with the big diameter probe (3.9 mm) of the same device.
Only for the ShockPulse-SE single and multiple-use probes were additionally compared. With single-use small probe (3.4 mm), the SCT (median) was 42.4 seconds (IQR 39.9–45.2) for hard stones and 18.2 seconds (IQR 17.2–19.1) for soft stones. However, using multiple-use small probes, SCTs of 45.2 seconds (IQR 43.7–46.7) for hard stones and 22.0 seconds (IQR 20.6–23.0) for soft stones were observed.
Similar superiority of single-use probes was described in terms of the bigger diameters. With the single-use big probe (3.76 mm), the median was 35.2 seconds (IQR 34.2–36.0) for hard stones and 17.0 (IQR 16.6–17.8) for soft stones. However, with the multiple-use big probe, it was 40.5 (IQR 38.9–42.7) for hard stones and 19.1 seconds (IQR 18.5–21.7) for soft stones. These data are summarized in Table 1.
In Vitro and In Vivo Stone Clearance Times for Each Device
IQR = interquartile range.
Comparison in SCT between composition of stones and diameter of probes for each device
All the devices were statistically faster in the treatment of soft stones than hard stones (p < 0.001).
No significant difference was observed between big- and small-diameter probes of Lithoclast Master when hard stones were treated (p < 0.131). In contrast, using the Lithoclast Master on soft stones or the Olympus ShockPulse-SE and the Lithoclast Trilogy on both hard and soft stones, statistically significant shorter SCTs were reported for bigger probes (p < 0.007 for all the experiments as shown in Table 2).
In Vitro Comparison in Stone Clearance Time Between Composition of Stones (Soft vs Hard), Diameter of Probes (Big vs Small Diameter), and Number of Use of the Probes for Each Device Used
Comparison in SCT between single- and multiple-use probes for the Olympus ShockPulse-SE
Regardless of size of the probe and composition of the stone, the use of disposable probe resulted in statistically significant faster outcomes (p < 0.05) (Table 2).
Comparison in SCT between the three lithotripters
Comparing the devices directly, the results showed that the Lithoclast Master had a longer clearance time compared with the other two devices. On the other hand, the Lithoclast Trilogy was found to be the fastest in the comparison with both Lithoclast Master and the Olympus ShockPulse-SE. Detailed data are reported in Table 3.
In Vitro Comparison in Stone Clearance Time Between the Three Lithotripters
In vivo experiment—porcine model
For the in vivo experiment, 4 pigs were included to accomplish treatment of 20 (10 hard and 10 soft) stones.
SCT for each device
In vivo, the SCT using the Lithoclast Trilogy was 69.2 seconds (IQR 66.3–70.1) for hard stones and 35.6 seconds (IQR 31.6–36.9) for soft stones. Using the Olympus ShockPulse-SE, the same treatment required longer time: The SCT was 130.2 seconds (IQR 128.6–131.5) for hard stones and 59.4 seconds (IQR 58.9–61.2) for soft stones (Table 1).
Comparison in SCT between soft and hard stones for each device
As well as in the first part of the experiment, hard stones were associated with significantly worse outcomes (p < 0.008) (Table 4).
In Vivo Comparison in Clearance Time Between Soft and Hard Stones for Each Device
Comparison in SCT between two lithotripters
Regardless of the composition of stones, Lithoclast Trilogy was found to be statistically more efficient in terms of SCT than the ShockPulse-SE (p < 0.008), as reported in Table 4.
Discussion
The development of ultrasonic lithotripters with combined suction led to notable improvements in the stone-free rate, clearance time, and safety for the patients undergoing PCNL. 2,8 Pneumatic lithotripsy was also considered as a highly effective instrument for the fragmentation of all types of stones, but it was associated with longer operative time. This was due to the lack of an integrated suction that dictated the need for the use of retrieval systems for fragment extraction (e.g., grasper). 9,10
Consequently, modern dual-energy lithotripters were designed to combine the advantages of the two energy sources (ultrasonic and pneumatic probes) in a single instrument, as it happens with the Lithoclast Master (dual-probe lithotripter).
9
The new generation devices even work with a dual-energy system in a single probe: - ShockPulse-SE by Olympus is a dual-action lithotripter simultaneously producing constant ultrasonic vibration and intermittent shockwave (ballistic) energy at a high rate. - Lithoclast Trilogy by EMS uses the same hollow probe ultrasonic vibration with an electromagnetic impactor.
9
Several studies have demonstrated the efficiency of these single devices. 3,4,11 –13 Better performance of the ShockPulse-SE was shown in the clinical evaluation of Chew and colleagues, describing the effectiveness of this single-probe dual-energy lithotripter compared with three ultrasonic devices (LUS-2, CyberWand by Olympus and Lithoclast by EMS). The outcomes of fragmentation of artificial hard and soft stones in a simulated kidney model were reported. 3 Sabnis and coworkers described the advantages of the Lithoclast Trilogy in terms of speed, ease of use, high tissue safety, and optimized suction during mini and standard PCNL. 4 However, to our knowledge, none of the studies performed so far has investigated and compared the outcomes of all modern duel-energy lithotripters.
The current study was the first to directly compare these three lithotripters focusing on the features of the probes (diameter and number of uses) and composition of stones by using a large number of experiments.
To better standardize the protocol, artificial stones were made with equal properties. They were prepared with two powder-to-water ratios (15:3 and 15:6), chosen to resemble two groups of stones, hard and soft, comparable to calcium oxalate monohydrate (COM) and magnesium ammonium phosphate hydrogen (MAPH) stones, respectively. 6
The first conclusion of the study is that all the devices work more efficiently on soft stones than on hard stones, in both in vitro and in vivo porcine models. This reflects what, most of the time, the endourologists perceive in their daily practice where MAPH stones are more easily manageable compared with COM stones. 14,15
In vitro, the median treatment time of these stones was never longer than 1 minute for all the devices, even when hard stones were treated. In vivo, the overall clearance time was slightly longer, but still around 2 minutes. Time is a key issue, especially for endourological procedures. Although PCNL is a less invasive procedure as opposed to pyelolithotomy, it is still associated with a risk of complications (blood loss requiring transfusion, fever up to urosepsis, steinstrasse, embolism), which tend to increase with the longer operative time. Thus, keeping the procedure short could probably increase the safety and lead to a decreased rate of complications. 16,17
Stone treatment with smaller-diameter probes resulted in significantly slower SCTs than working with bigger-diameter probes of the same devices. The only exception was related to the Lithoclast Master: Although the bigger probe was faster during the trials, the outcome was not statistically significant, underlining a potential small difficulty of this device to treat hard stones regardless of the diameter of the probes.
The ShockPulse-SE was tested with disposable and multi-use probes: The former presented a significantly higher efficiency than the latter. In addition, a higher frequency of obstruction of the probe by fragments during the lithotripsy with multi-use probes was observed.
Focusing on direct comparisons, the Lithoclast Master with longer clearance times was the least efficient compared with the other two lithotripters, regardless of the hardness of stones and the diameter of probes.
Carlos and associates analyzed the performance of these two devices in an in vitro setting and the Trilogy (3.9 mm probe) was significantly superior on clearance test than the ShockPulse (3.76 mm probe). 5 Unlike our study, they evaluated the data of bigger probes for both of the devices, the diameter of which was apparently smaller for the ShockPulse. This could introduce a bias to correctly interpret the gained outcomes.
Bader and colleagues conducted a similar in vitro experiment. Trials were performed by five operators only on hard stones. The Trilogy was again found to be the fastest in both clearance and drilling tests. 18 The results of our study are concurring with the aforementioned results.
In a prospective randomized clinical trial evaluating the ablation rate and type of complications (Giusti et al.), the ShockPulse-SE had a significant higher speed than the one of the Lithoclast Master. 19
Our final comparison was conducted in vivo, on a porcine model, between the two best devices proven in the first part of the experiment (the Lithoclast Trilogy and the ShockPulse-SE), using exclusively single-use probes with identical diameter (3.4 mm).
Even in these circumstances, the Lithoclast Trilogy showed better clearance times for hard and soft stones than the opponent device with a notable statistical significance (p < 0.008). No similar in vivo studies are still available. Considering that the observed trends in the in vitro and in vivo experiments were similar for both devices, with Lithoclast Trilogy being superior, we think that our in vitro data are realistic and can be used as a reference.
A recent review about advances in PCNL supports our results: The Lithoclast, Trilogy, thanks to its better suction properties, high mean stone volume clearance, and low complication rate, is included among the new technologies that significantly improve the procedure, even with a miniaturized instrument in the mini-PCNL (sheath size: 14–22F). 20
Our study has some limitations. Although the anatomy of the porcine kidney has similarities to the human one, it is not exactly the same. Pig kidneys are tilted inward 20° from the sagittal plane (instead of the 30° of the human), so their working orientation is marginally different. The pyelocaliceal system shows less compliance with a large number of small calyces. Two different consistencies of artificial stones were selected. These stones were made according to a previous study to replicate the properties of COM and MAPH stones, which represent two of the most common types of urinary stones. 6 The efficacy of the lithotripter on stones of other compositions was not investigated in this study, but it can represent a starting point for possible future investigations.
Despite the aforementioned limitations, the current study shows how new-generation lithotripters are designed to make the procedures simpler and faster. They all provide high performance with short clearance times in the treatment of stones. These data, along with the spreading of standardized techniques for percutaneous access (e.g., Bull's eye technique), consolidate the idea that PCNL is not anymore a procedure restricted to a small group of selected urologists.
The performances result faster in the treatment of soft stones and using larger or disposable probes. The Lithoclast Trilogy, a dual-energy single-probe lithotripter, appeared the most efficient in terms of clearance time according to our results.
Further clinical investigations (prospective randomized studies) will help endourologists to better understand the reliability and safety of these devices, with regard to intra- and postoperative complications.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This study received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.