
Abstract
Background:
Some reports in the literature describe lymphocele formation in as much as half of patients after pelvic lymph node dissection (PLND) in robot-assisted radical prostatectomy (RARP), with 1%–2% requiring intervention. Several treatment modalities for symptomatic lymphoceles are available, including percutaneous drainage, sclerosing agents, and surgical marsupialization, typically performed by laparoscopy or with a multiport robotic platform. The advantage of surgical approach is permanent excision of the lymphocele capsule and fewer days with pelvic drains compared to percutaneous drainage. This study aims to describe and illustrate, for the first time, the step-by-step surgical management of symptomatic lymphoceles using a less invasive robotic platform, the da Vinci
Materials and Methods:
We describe the outcomes of three patients who underwent lymphocelectomy and marsupialization with the da Vinci SP for symptomatic lymphoceles after RARP and PLND with the da Vinci Xi.
Results:
Operative time for cases 1, 2, and 3 was 84, 80, and 79 minutes. The blood loss for each surgery was 25 mL. Patient 2 was discharged in 3 days, whereas patients 1 and 3 were discharged in 4 days. No intraoperative or postoperative complications were reported. All patients had their drain removed in under 24 hours after surgery. The mean follow-up period was 7.7 months (3.5–15.8). No patients were readmitted or had lymphocele recurrence.
Conclusion:
Da Vinci SP lymphocelectomy is safe and feasible with satisfactory outcomes. The SP enables definitive treatment of the lymphocele sac, reducing the number of days with abdominal drains, and allows further decrease in surgical invasiveness with fewer incisions and better cosmesis.
Introduction
Pelvic lymph node dissection (PLND) is the most effective modality to detect nodal metastasis in men with prostate cancer. The American Urologic Association (AUA) and the European Association of Urology (EAU) recommend PLND in intermediate- and high-risk patients with prostate cancer, who undergo radical prostatectomy. 1,2 Previous studies have demonstrated an increase in biochemical relapse, symptomatic disease progression, and overall cancer-specific mortality corresponding with the number of positive nodes at the time of lymphadenectomy. 3,4 However, literature regarding the extent of PLND and long-term therapeutic benefit of PLND is still limited.
Despite the AUA and EAU considerations, PLND is not devoid of complications. The lymphocele rates after PLND can range from 9% to 54% depending on the surgical modality and number of lymph nodes removed. 5,6 Most lymphoceles are asymptomatic without clinical consequence and do not require treatment. 7 Seetharam and colleagues, assessing over 5000 patients treated with robot-assisted radical prostatectomy (RARP) and PLND, described 2% of patients with symptomatic lymphocele requiring intervention. 8 There are several treatment modalities for symptomatic lymphoceles, including aspiration, percutaneous drainage, and sclerosing agents, and in refractory cases, surgical marsupialization may be performed. 8 However, the literature still lacks well-designed studies describing the optimal treatment for this complication.
Percutaneous drainage is the most common treatment for infected lymphoceles. However, with increased recurrence rates proportional to lymphocele size and the need for prolonged use of pelvic drains, this modality has its limitations.
9
–11
On the other hand, minimally invasive marsupialization is associated with a permanent treatment of the lymphocele cystic capsule and higher postoperative quality of life for patients because of fewer days with surgical drains.
12
–14
Currently, the minimally invasive lymphocele treatment is performed by laparoscopy or with the multiport da Vinci
In this scenario, the recently introduced da Vinci Single Port (SP) has some potential advantages over the conventional multiport robotic approach attributable to less invasive access. 15 Therefore, instead of multiple incisions to place the trocars for the multiport console, the lymphocele is treated with only one or two incisions. 16 This study aims to illustrate, for the first time in the literature, the step-by-step surgical management of symptomatic lymphoceles using the da Vinci SP.
Materials and Methods
Data acquisition
We collected data prospectively from June 2019 to December 2019, at our center (Advent Health Celebration, FL), on patients who underwent six-port transperitoneal RARP and PLND with the da Vinci Xi (Institutional Review Board approval number 237998-40), with our previously described surgical technique. 17 Perioperative complications were evaluated using the Clavien-Dindo grading score. 18 Three patients were diagnosed with symptomatic lymphoceles after RARP and PLND and were subsequently treated with lymphocelectomy and marsupialization with the da Vinci SP system. All surgeries were performed by a single experienced surgeon (V.P.).
PLND technique
PLND was performed in all intermediate- and high-risk patients based on D'Amico score.
19
The primary template boundary of PLND was the external iliac vein laterally, bladder medially, obturator nerve posteriorly and proximal extension to the common iliac artery, and its bifurcation. Hem-o-lock
Patient presentation and case scenarios
The first patient went to the emergency department 4 months after his initial RARP with fever of 106°F and elevated white blood cell (WBC) count. Computed tomography (CT) revealed a 9.3 × 7.1 cm lymphocele on the left pelvic sidewall (Fig. 1).
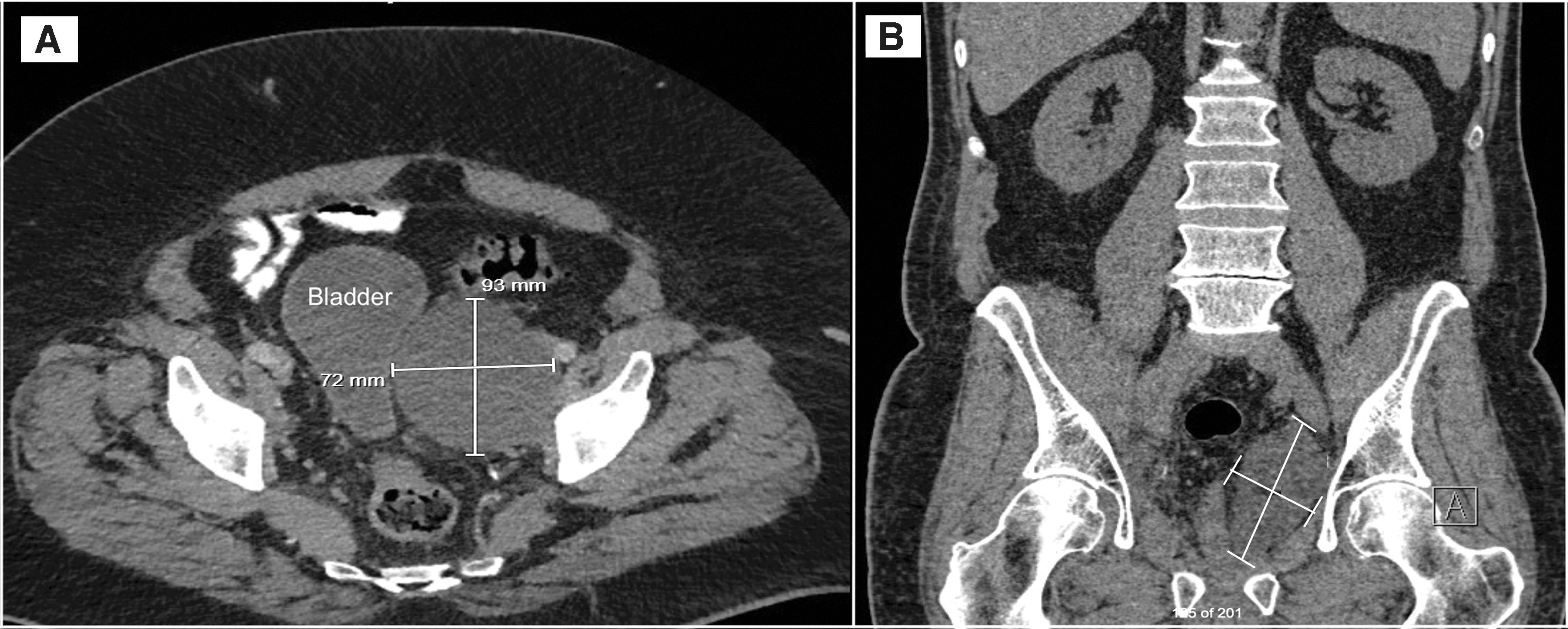
Abdominal and pelvic CT describing the 9.3 × 7.1 cm pelvic lymphocele in
The second patient presented to our institution 1 month after his initial RARP in a similar clinical scenario with fever of 104°F and CT revealing bilateral lymphoceles measuring 6.1 × 4.0 cm on the right and 5.8 × 3.8 cm on the left pelvic sidewall compressing the urinary bladder (Fig. 2).

Abdominal and pelvic CT describing 6.1 × 4.0 cm and 5.8 × 3.8 cm bilateral pelvic lymphoceles in
The third patient went to the emergency department 2 months after his initial RARP with fever of 104°F, abdominal pain, and elevated WBC count. The CT revealed a 12.7 × 8.0 cm lymphocele on the right pelvic sidewall compressing the bladder (Fig. 3).
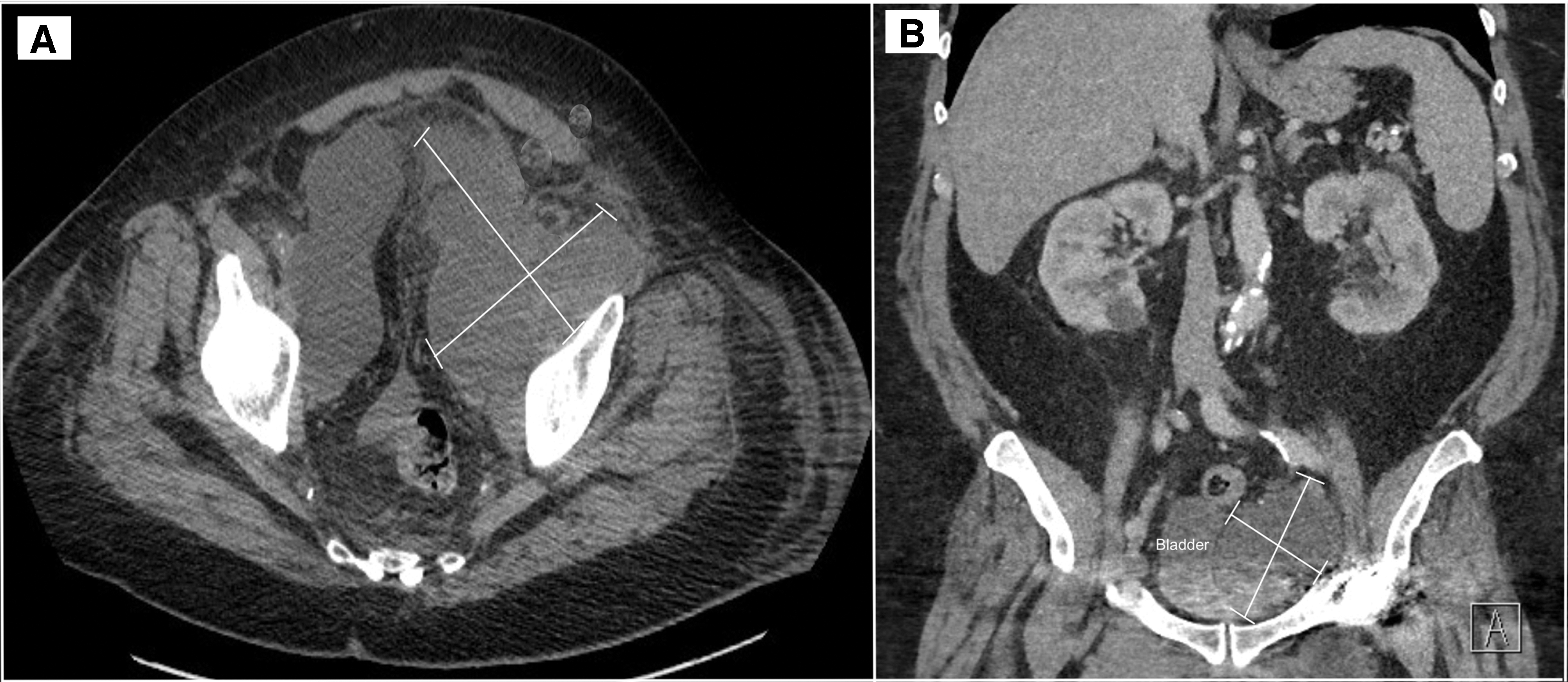
Abdominal and pelvic CT describing the 12.7 × 8.0 cm pelvic lymphocele in
All patients were admitted for intravenous (IV) antibiotics and treatment. The patients were given the options of radiologic drainage vs robotic marsupialization of the lymphocele cavity in the operating room. All patients understood the potential complications and consented for robot-assisted SP drainage.
The da Vinci SP system
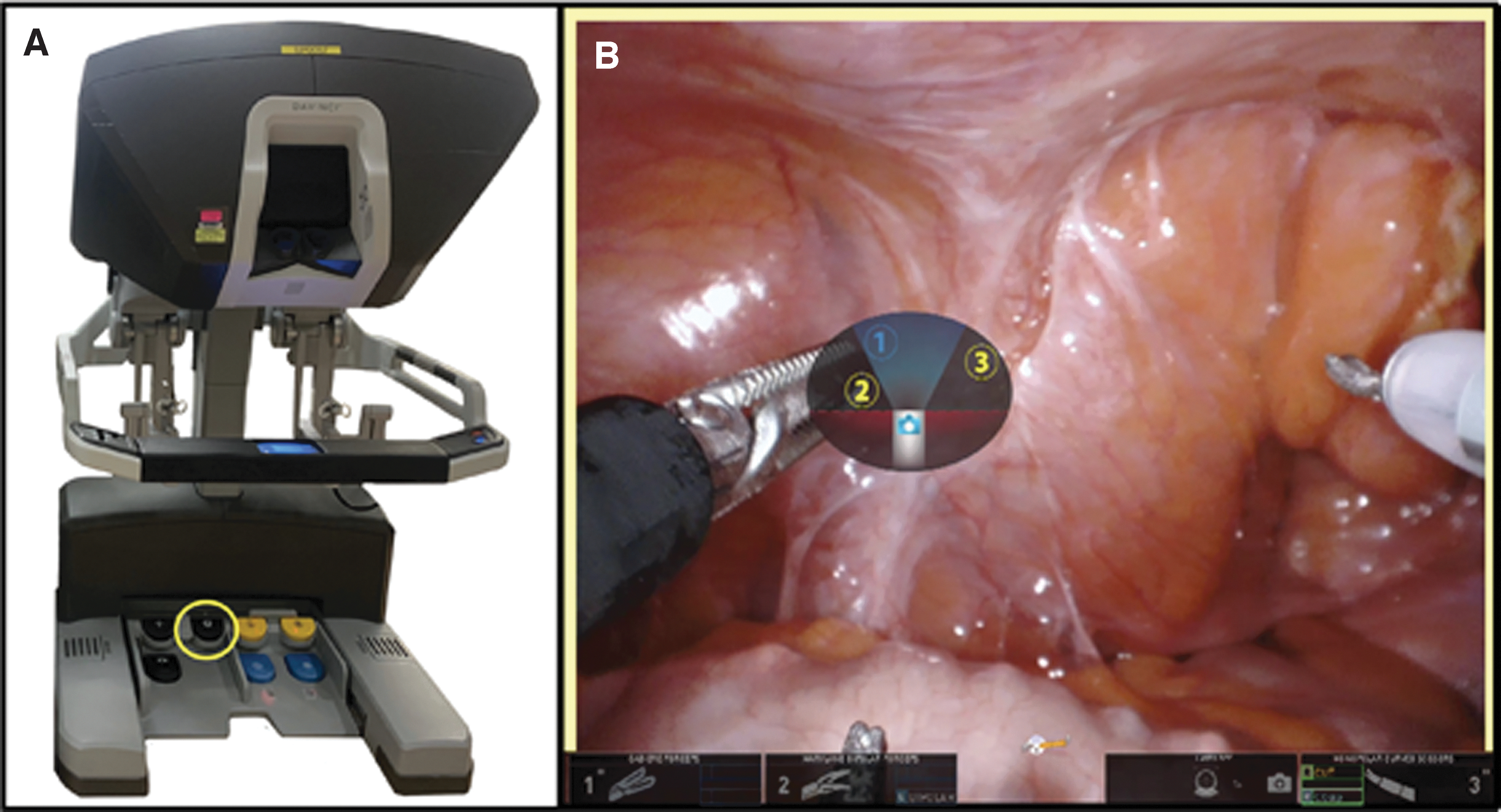
The da Vinci SP was approved by the Food and Drug Administration (FDA) in 2018 and has already demonstrated a significant advancement in minimally invasive surgery, especially within urology. 15,20,21 This innovative technology utilizes a single 25 mm multichannel port to accommodate three independent working arms and one scope. All arms are 6 mm in diameter with two points of articulation to allow the instrument triangulation without clashing. A high-definition 10 × 12 mm scope with several angles of deflection enables exceptional visualization. In addition, the advent of the relocation pedal allows the robot to work in multiple quadrants without redocking or new port placement (Fig. 4).
Patient positioning, port placement, and docking
All patients were placed in a supine position and a bilateral transverse abdominis plane block was performed after the intubation.
22
Afterward, a 3 cm supraumbilical midline incision was made to place the 25 mm port.
16
An additional 5 mm AirSeal
Surgical technique
Pneumoperitoneum was established using the AirSeal as much as 12 mm Hg. The lymphocele was identified, and the peritoneum was separated from the lymphocele sac (Fig. 5). The sac was dissected circumferentially until adequate exposure was achieved. Care was taken to identify the correct anatomic planes owing to the intense pelvic inflammation avoiding injury to the ureter, which was displaced by the lymphocele in all cases. The lymphocele sac was punctured, and its fluid was suctioned and sent for culture and cytological examination (Fig. 5). Afterward, the anterior wall of the sac was resected using the monopolar scissors and bipolar forceps, and the interior of the sac was cleaned with saline (Fig. 6). The remaining interior sac wall was cauterized using monopolar energy and the pelvis was thoroughly inspected to ensure adequate hemostasis. A Jackson-Pratt
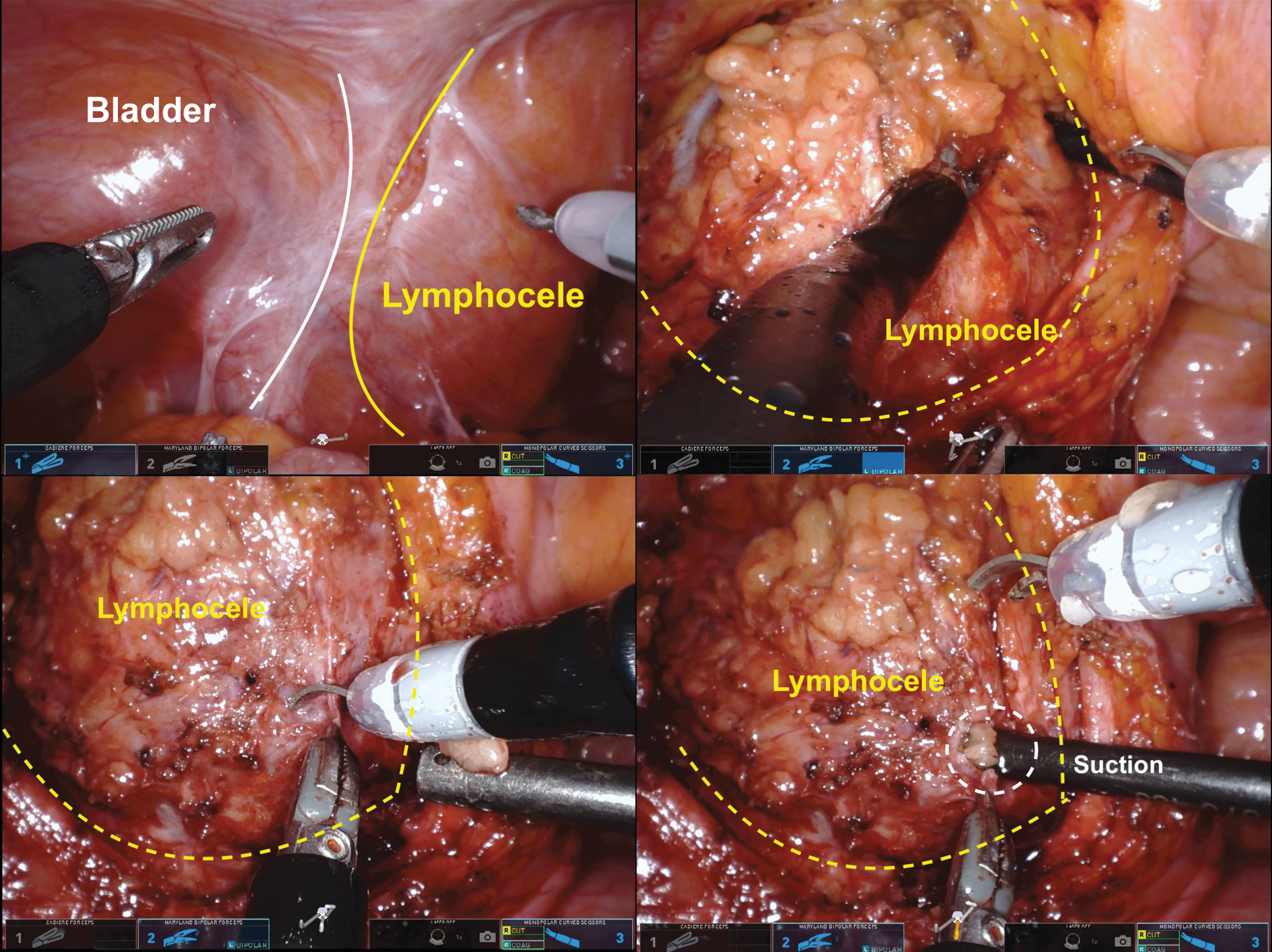
Different steps during the intraoperative lymphocele dissection and fluid aspiration with the suction device. Color images are available online.
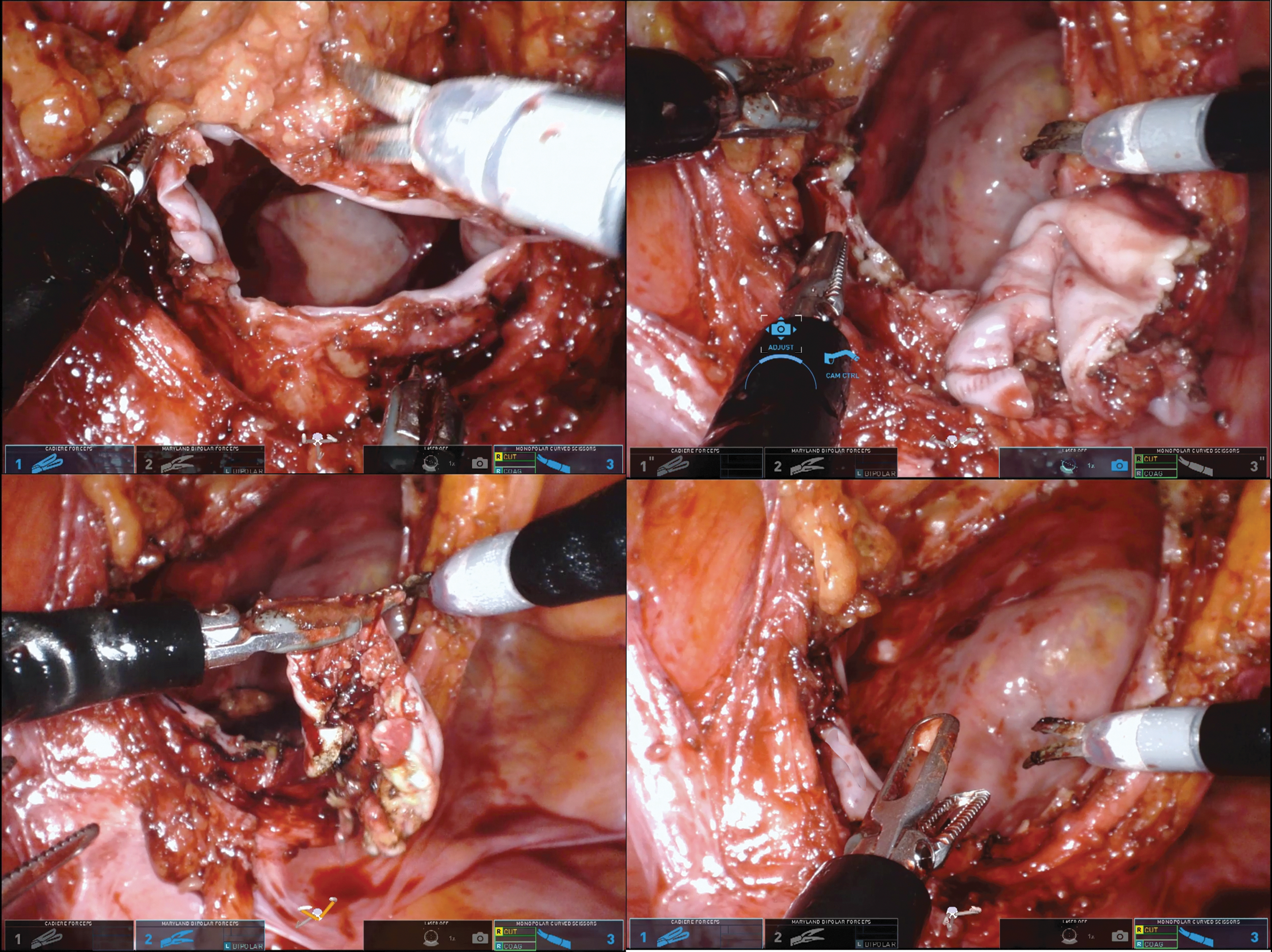
Different steps during the lymphocele sac opening and marsupialization. Color images are available online.
Antibiotic management and postoperative follow-up
The Infectious Disease team performed antibiotic therapy management in all cases. The patients underwent blood culture examinations in the admission and then received empiric IV Tazobactam + Piperacillin attributable to the high fever and clinical scenario. Afterward, antibiotic therapy was guided by blood culture and lymphocele fluid culture (drained during the surgery). For discharge, we usually select an oral antibiotic sensitive to the cultures.
After surgery, the patients had deep vein thrombosis (DVT) prophylaxis with heparin and compressive socks until appropriate ambulation and mobilization. All patients underwent abdominal and pelvic ultrasound after 3 months of surgical drainage to screen lymphocele recurrence.
Results
The mean follow-up period was 7.7 months (3.5–15.8). Patient demographics and preoperative characteristics are demonstrated in Table 1. Median age was 67 and median time to presentation after RARP was 60 days. Table 2 describes the perioperative outcomes. The operative time for case 1, 2, and 3 was 84, 80, and 79 minutes. Estimated blood loss for all cases was 25 mL. No intraoperative or postoperative complications were reported. The patients were discharged at least 3 days after surgery owing to the elevated WBC count and IV antibiotic use. All patients had the abdominal drain removed <24 hours after surgery. No patients were readmitted or had lymphocele recurrence after discharge.
Patient Demographics and Outcomes of Robot-Assisted Radical Prostatectomy
BMI = body mass index; EPE = extraprostatic extension; GrGP = Grade Group; ISUP = International Society of Urological Pathology; LN = lymph node; PSA = prostate-specific antigen.
Perioperative Outcomes of Lymphocele Drainage and Marsupialization Using the da Vinci Single-Port Console
CT = computed tomography; EBL = estimated blood loss.
Discussion
The advent of a pure SP robotic platform, the da Vinci SP system, has the potential to advance robotic surgery by building upon the minimally invasive approach of performing challenging surgery within confined spaces with fewer incisions. Since its recent approval by the FDA in 2018, the feasibility of the SP system has been described by different authors in various urologic approaches for kidney, bladder, and prostate surgery. 20 Despite the multiple series of surgeries performed with this console in the literature, this is the first study to describe minimally invasive lymphocele drainage and marsupialization utilizing the da Vinci SP system.
Symptomatic lymphoceles are associated with increased morbidity, hospitalization, and health care costs. Musch and colleagues performed a study of 1380 patients who underwent radical prostatectomy and demonstrated that patients with lymphocele had an 8% rate of DVT and a 3% rate of pulmonary embolism. 23 Therefore, high clinical suspicion for venous thromboembolism and further radiologic testing are warranted before the lymphocele surgical management.
The incidence of lymphoceles requiring drainage ranges from 0.4% to 16%. Some require multiple drainage attempts, use of sclerosing agents, and occasionally, surgical management, especially in larger, multiseptated lymphoceles or those that fail previous percutaneous drainage. 18 Some studies reported that the rate of formation is decreased with minimally invasive surgery compared to open and in transperitoneal vs extraperitoneal approaches. 19,20 In addition, previous studies have determined that the increased rate of lymphoceles can be associated with a lack of clips, use of anticoagulation, and increased use of postoperative imaging. 21 In our experience, ∼2% of lymphoceles require intervention, and on multivariable analysis, we described that the number of nodes removed increases the likelihood of postoperative drainage. 9
The challenges associated with lymphocelectomy using the da Vinci SP system are similar to the multiport robot. Care must be taken to avoid injuries to surrounding organs and vessels when resecting the lymphocele sac, as increased inflammation disrupts normal anatomic planes and increases the chance of complications. Despite the reduced capacity of traction provided by the SP robot compared with the multiport, this console's biarticulated tools allow meticulous dissection of the target anatomy. The relocation pedal is essential when moving from one quadrant to another in cases of bilateral lymphoceles. It is crucial to keep all instruments in the middle of the screen under direct visualization to avoid potential injury to surrounding tissues when using this pedal and relocating the instruments.
Furthermore, the minimally invasive SP access enables surgical drainage with one or two small incisions performed on the same scars of the previous surgery, providing a permanent treatment (marsupialization) with low recurrence rates. In terms of quality of life, the patient typically has an abdominal drain for <24 hours after surgery. In contrast, with percutaneous drainage, the patient remains with an abdominal drain for an extended period of time and another percutaneous procedure to sclerose the lymphocele is usually required before drain removal. Moreover, the percutaneous drainage of bilateral lymphoceles often requires more than one puncture and the placement of more than one drain. Finally, the thick purulent content of some infected lymphoceles can be entirely removed and cleared with surgery, unlike with small percutaneous drains that have inherent limitations draining this type of fluid.
Our study is not devoid of limitations. First, because of its retrospective design and all the inherent limitations associated. Second, the small number of patients and short-term follow-up are also considered limitations. However, this is the first report of SP lymphocele drainage in the literature. Previous studies described the SP application in urologic procedures as safe and feasible. We believe that this new console could also be used in urology as a less invasive alternative for surgical candidates of lymphocele drainage.
Conclusion
Lymphocele drainage with the da Vinci SP robot is safe and feasible with satisfactory outcomes. The SP system enables definitive treatment of the lymphocele sac, reducing the number of days with abdominal drains, and allows a further decrease in surgical invasiveness with fewer incisions and better cosmesis.
Footnotes
Author Contributions
All authors contributed to the study conception and design, material preparation, and data collection and analysis. The first draft of the article was written by Dr. M.C.M. and T.H., and all authors commented on subsequent versions of the article. All authors read and approved the final article.
Author Disclosure Statement
According to the International committee of medical journal editors' (ICMJE) conflict of interest, the authors Dr. M.C.M., T.H., Dr. S.R., Dr. S.B., Dr. T.R., M.S., J.N., and Dr. V.P. declare that they have no conflict of interest or competing financial interests related to the article. Dr. V.P. is consultant for Exact Sciences/Genomic Health, Decipher/Genomic DX, Active Surgical, and AVRA.
Funding Information
No funding was received for this article.