
Abstract
Background:
Tumor enucleation technique in robot-assisted partial nephrectomy (RAPN) reportedly contributes to renal function preservation. Which tumors and which part to utilize this technique have not been determined.
Patients and Methods:
This multi-institutional retrospective study included patients who underwent RAPN at tertiary surgery centers. Patients were first stratified into High, Intermediate, and Low categories based on renal nephrometry score. Patients were further classified into I/B-enucleation (I/B-E, I + B ≤ 1) and I/B-resection (I/B-R, I + B ≥ 2) groups based on surface-intermediate-base margin score. Perioperative outcomes, including percentile change in estimated glomerular filtration rate (eGFR), new-onset chronic kidney disease, complication rate, surgical margin, and trifecta achievement, were compared between the I/B-E and I/B-R groups in each category. Odds ratios (ORs) and β-coefficients were also compared.
Results:
Overall, 704 patients were included in this study. Relative decrease in eGFR was significantly lower for the I/B-E group in all three categories, with medians of 8.1%, 4.4%, and 3.2% in the High, Intermediate, and Low, respectively. In multivariate analyses, excision technique was independently associated with eGFR change in all three. β-coefficient was higher in the High (5.06) category than in the Low (3.17) or Intermediate (3.33). Across all three categories, significantly more patients attained trifecta with a difference of 34.0%, 18.3%, and 15.1% in the High, Intermediate, and Low categories, respectively (all, p < 0.05), with a higher OR in the High (5.91) category than in the Low (3.20) or Intermediate (2.48). No significant differences were found in operation time, amount of estimated blood loss, rate of positive surgical margin, or complications. Warm ischemic time was significantly longer for the I/B-E group in the Intermediate (18.0 minutes vs 16.0 minutes, p = 0.002) and Low categories (13.0 vs 11.0, p = 0.006), but not significant in High (p = 0.344).
Conclusions:
I/B-enucleation in RAPN contributes to renal function preservation, and the impact was more emphasized in complex tumors.
Introduction
Partial nephrectomy (PN) reportedly provides equivalent oncological control and preserves more renal function compared with radical nephrectomy as a surgical management of small renal tumors. 1 Recently, robot-assisted partial nephrectomy (RAPN) has emerged as a minimally invasive alternative to open PN and has gained popularity for its advantages on enabling easier and more precise dissection and reconstruction. 2 These features allow application of RAPN for treating larger or high-complexity tumors. With aging of the general population, particularly in developed countries, the number of patients with chronic kidney disease (CKD) requiring surgery for renal tumors, is expected to increase, 3 indicating higher chances for the requirement of PN.
Enucleation is defined as dissection along the peritumoral pseudocapsule without additional renal parenchyma. 4,5 Numerous reports support its feasibility and advantages in terms of renal function, but its technique and definition greatly vary. 6,7 Minervini and colleagues proposed surface-intermediate-base (SIB) margin score as a standard reporting system for excision technique. This has been utilized in several studies, including ours, reporting that enucleation, defined as a total SIB margin score ≤2, possibly contributes to the preservation of renal function compared with resection technique. 8 –14 However, which tumors benefit most from enucleation and which part to utilize this technique have not been determined.
Based on our previous reports, we hypothesized that the advantage is maximized in tumors with higher R.E.N.A.L. nephrometry score (RNS). In our hand, the score of surface (S) in the SIB margin score is 1 point in almost all patients. We speculate that the resection manner at the intermediate to base of the tumors, an area with more contact surface with normal renal parenchyma, is more likely to influence the surgical results. 15 This study aimed to compare the benefits of enucleation performed at the intermediate to base of the tumor based on three RNS categories (Low, Intermediate, and High).
Patients and Methods
Study design and patient selection
This retrospective study included 709 consecutive patients who underwent RAPN at 2 tertiary institutions between April 2016 and November 2019. Patients whose estimated glomerular filtration rate (eGFR) was <15 mL/min/1.73 m2 before surgery were excluded.
Data collection
All clinical and laboratory data were obtained from the institutions' electronic databases and patient medical records. The Internal Ethics Review Board of Tokyo Women's Medical University approved this study (Approval ID: 5685), which was performed in accordance with the Declaration of Helsinki. The requirement for formal consent was waived because of the retrospective observational nature of the study.
SIB margin score was recorded by the operating surgeon prospectively in each patient immediately after surgery, according to the original report. 4 Patients were first stratified by tumor complexity according to three RNS categories and then classified within each category into two groups: I/B-enucleation group (I/B-E, I + B ≤ 1) and I/B-resection (I/B-R) group (I + B ≥ 2). For each RNS category, changes in percentage eGFR (%eGFR), preservation of 90% eGFR, new onset of CKDG3 (eGFR <60 mL/min/1.73 m2), new onset of CKDG3b (eGFR <45 mL/min/1.73 m2), positive surgical margin status, perioperative complications, warm ischemic time, and trifecta (90% eGFR preservation, negative surgical margin, and no perioperative complications) were compared between the I/B-E and I/B-R groups. The results were compared across the RNS cohorts by β-coefficient or odds ratios (ORs) to assess surgical outcomes.
Surgical procedures and perioperative care
Four distinguished laparoscopic surgeons performed all RAPN surgeries. In the earlier study period, resection with 3 to 5 mm of normal renal parenchyma margin was intended, whereas enucleation technique was considered in the more recent cases. The indication to utilize enucleation was based on factors such as tumor configuration (smooth and spherical tumors), estimated large contact surface area on preoperative enhanced CT scan, and pseudocapsule evident on preoperative CT imaging. The final decision to perform enucleation or resection was decided by the operating surgical team. Decision to choose transperitoneal or retroperitoneal approach was made by considering tumor location.
The procedures have been previously detailed. 9 All preoperatively recognized arteries were clamped under warm ischemia. Enucleation was performed by dissecting the tumor along the peritumoral capsule, whereas resection was carried out by removing the tumor with a substantial renal parenchyma margin. After tumor excision, an inner running suture was placed using a barbed suture (15 cm 3-0V-Loc® 180 with a half-circle 17-mm needle; Covidien, New Haven, CT), and the renal artery was unclamped to confirm arterial hemostasis. Renorrhaphy was then performed with a barbed suture (30 cm 2-0 V-Loc 180 with a half-circle 37 mm needle; Covidien). In cases with large parenchymal defect, TachoSil® bolster was used to fill the gap. All surgeries, both enucleation and resection, were performed under the same reconstruction technique (inner suture and renorrhaphy). Postoperative management was generally performed according to the enhanced recovery after surgery protocol. 16,17
Evaluation of renal function
Preoperative and postoperative renal functions were evaluated within 2 months before surgery and 3 to 6 months after surgery, respectively. eGFR values were estimated using the modification of diet in renal disease equation modified for Japanese patients proposed by the Japanese Society of Nephrology (eGFR = 194 × SCr−1.094 × Age−0.287 × 0.739 [if female]). 18
Perioperative complications
All surgery-related complications within 3 months after surgery were recorded and graded using the Clavien-Dindo classification. 19 Prevalence of any and high-grade (3 or higher) complications was analyzed.
Statistical analysis
Continuous variables were analyzed using the Mann–Whitney U-test and expressed as median and interquartile range. β-Coefficient was calculated using linear regression models. Categorical variables were analyzed using the χ 2 or Fisher's exact tests with OR and 95% confidence intervals (CI). Multivariate linear regression models were used to adjust the β-coefficient for excision technique using the following variates: age at surgery, body mass index, year of surgery (2016–2017 or 2018–2019), Charlson comorbidity index score (≥3), American Society of Anesthesiologists (ASA) score, and tumor size. Multivariate logistic regression was performed to adjust OR using the same variates. All analyses were carried out using JMP software (version 14.0; SAS Institute, Cary, NC). Differences were considered statistically significant at p-values <0.05.
Results
Patient characteristics
After excluding 5 patients, 704 patients were finally enrolled. Patients were stratified into 3 RNS categories (Low: 256, Intermediate: 359, and High: 89) based on their characteristics (Table 1). For the SIB surface (S) score, except for three patients with S = 0 in the I/B-E (1.0%) and I/B-R groups (0.8%), all others had an S score of 1. Overall, percentage of patients receiving enucleation increased from 32.5% in 2016 to 46.2% in 2017 and 53.0% in 2018, finally falling to 36.9% in 2019.
Baseline Patient Characteristics
ASA = American Society of Anesthesiologists; BMI = body mass index; I/B-E = intermediate-base enucleation; I/B-R = intermediate-base resection; IQR = interquartile range; N/A = not applicable; RCC = renal-cell carcinoma; SIB = surface-intermediate-base.
More patients in the Low category underwent resection (71.1%), whereas more in the High (69.7%) category underwent surgery with enucleation. The distribution of ASA score was significantly different between I/B-E and I/B-R in Low and Intermediate categories (both p < 0.05), but not in High (nonspecific). Moreover, tumor size was larger with significance for I/B-E compared with I/B-R in Low (p < 0.001) and Intermediate (p < 0.001), but without significance in High (p = 0.235).
Comparison of renal function outcomes within each RNS category according to I/B excision technique
When analyzed by subgroups of three RNS categories, %eGFR loss was significantly smaller for the I/B-E group than I/B-R group in all three. The difference in %eGFR loss (median) was 3.2%, 4.4%, and 8.1% in the Low, Intermediate, and High categories, respectively (Fig. 1), with significantly more patients in I/B-E group maintaining 90% of preoperative eGFR (all, p < 0.05) and attaining trifecta (all, p < 0.05) across all categories. The difference in 90% eGFR achievement rates between I/B-E and I/B-R groups were 13.7%, 24.5%, and 32.8% in the Low, Intermediate, and High categories, respectively. The difference in trifecta attainment rate was 15.1%, 18.3%, and 34.0% in the Low, Intermediate, and High categories, respectively (Fig. 2 and Table 2).
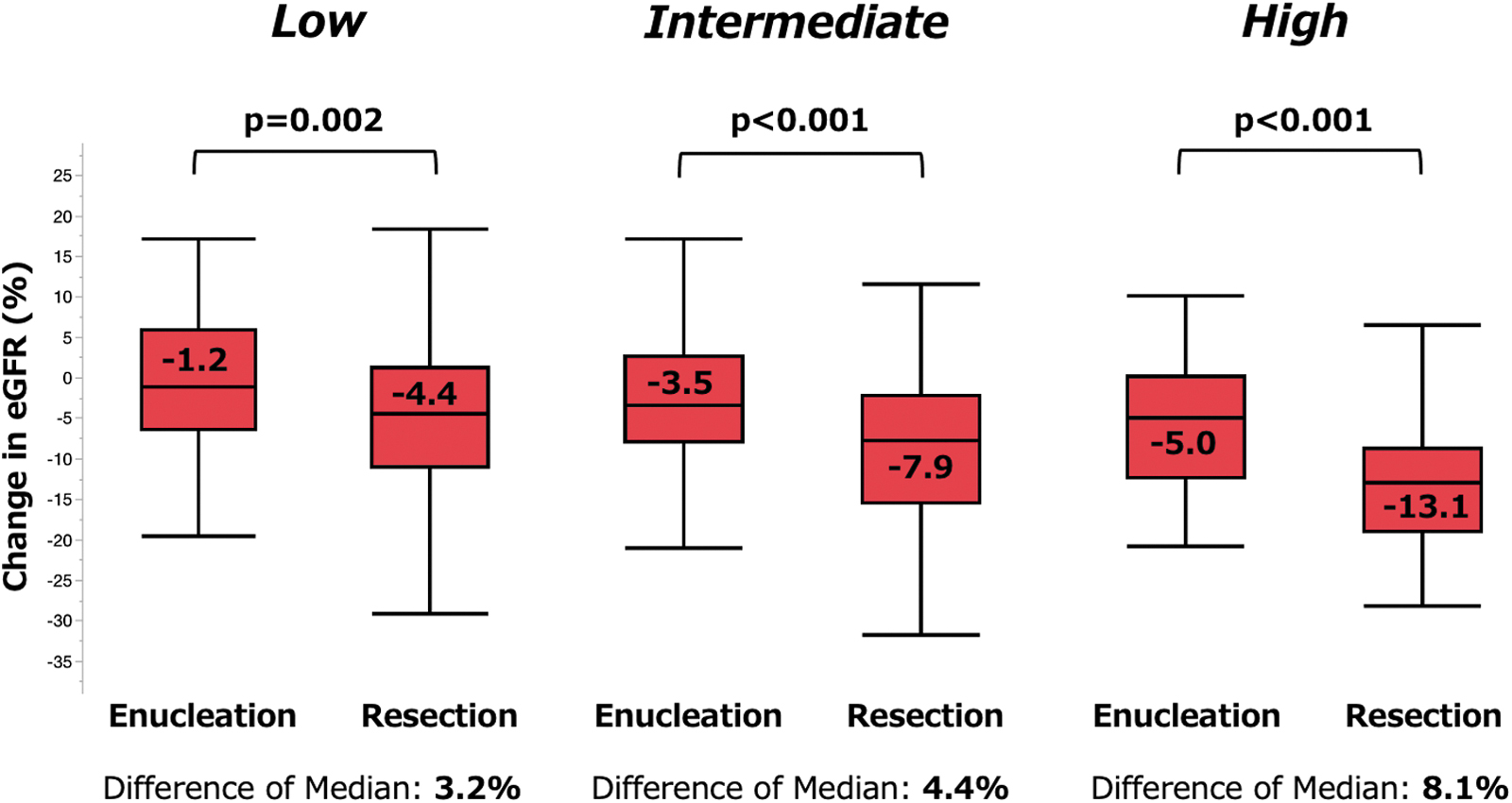
Comparison of relative eGFR change by three RNS categories. eGFR = estimated glomerular filtration rate; RNS = R.E.N.A.L. nephrometry score.
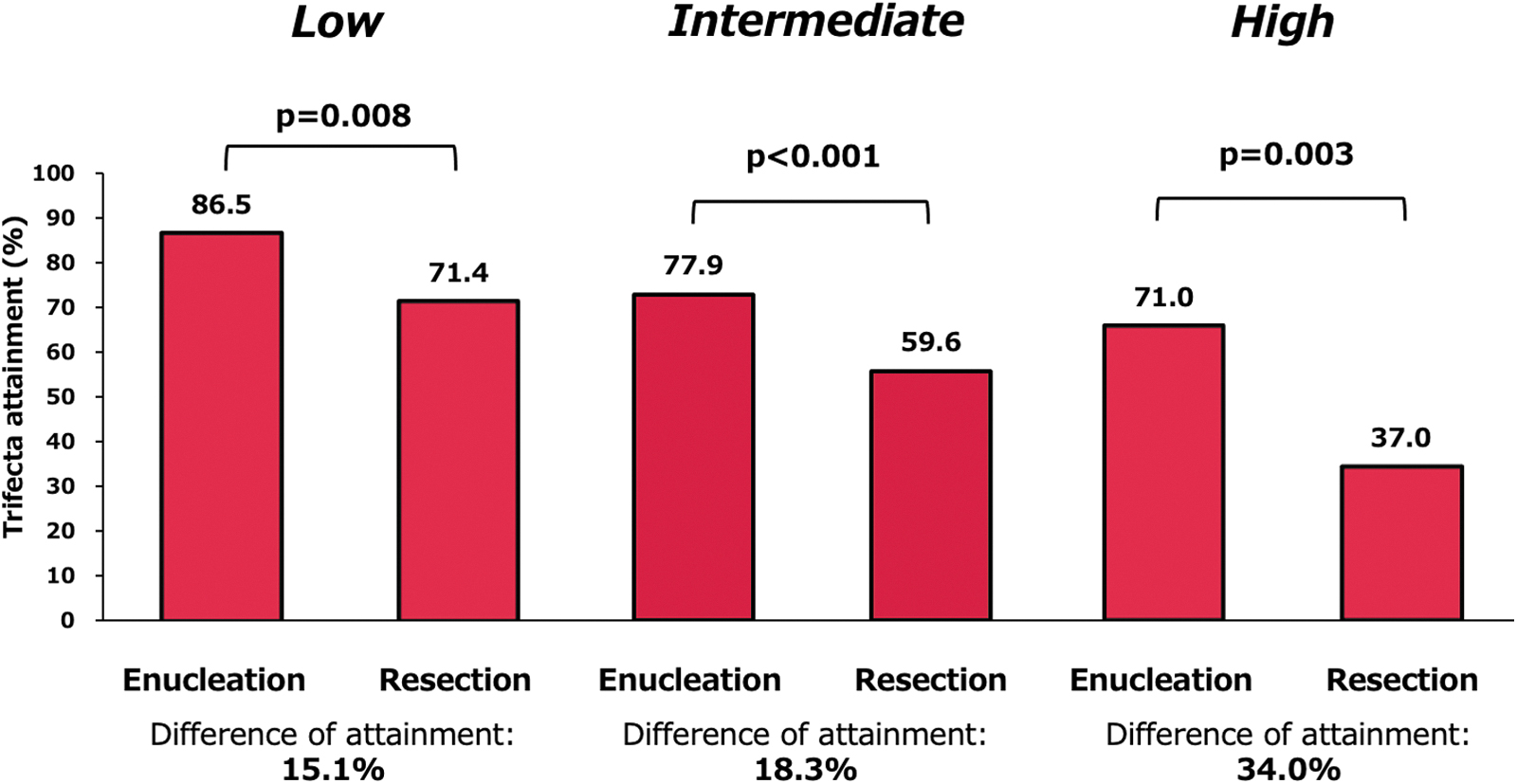
Comparison of trifecta attainment by three RNS categories.
Perioperative Outcomes by R.E.N.A.L. Nephrometry Score Classification
Complications defined as per Clavien-Dindo classification.
CKD = chronic kidney disease; eGFR = estimated glomerular filtration rate; WIT = warm ischemic time.
Other outcomes and perioperative complications according to I/B excision technique within each RNS categories
Operation time, amount of estimated blood loss, and rate of positive surgical margin were comparable between the I/B-E and I/B-R groups across all three categories (all, nonspecific). The incidence of perioperative complications of any grade or grade ≥3 was not significantly different between the two groups for all three categories (all, nonspecific) (Table 2). Warm ischemic time was significantly longer for the I/B-E group in the Intermediate (p = 0.002) and Low (p = 0.006) categories, but not significant in the High (p = 0.344) category.
Impact of excision technique in percentile change in eGFR and trifecta attainment: comparison between three RNS categories
We performed multivariate analyses to assess the impact of the excision technique on eGFR change and trifecta attainment, adjusting for possible independent variables. The results are summarized in Tables 3 and 4. The excision technique (I/B-E vs I/B-R) was significantly and independently associated with percentile change in eGFR across all categories (Low: β-coefficient 3.17 [SE 0.74], p < 0.001; Intermediate: 3.33 [0.63], p < 0.001; and High: 5.06 [1.36], p < 0.001), and β-coefficient was higher in the High category than in the Low or Intermediate. It was also a significant and independent factor for trifecta attainment in all three categories, with OR higher in the High (OR 5.91 [95% CI 1.94–18.06], p = 0.002) than in the Intermediate (OR 2.48 [95% CI 1.50–4.11], p < 0.001) or Low (OR 3.20 [95% CI 1.44–7.14], p = 0.005) category.
Multivariate Linear Regression for Change in Estimated Glomerular Filtration Rate (%)
SE = standard error.
Multivariate Logistic Regression for Trifecta Attainment
CI = confidence interval; OR = odds ratio.
Discussion
Enucleation during RAPN at the intermediate to base portion of renal tumors significantly contributed to the preservation of renal function, regardless of tumor complexity; this was more emphasized in complex tumors. No significant differences were found regarding surgical margin or complications.
The optimal margin of normal or healthy renal parenchyma has been debated for decades. Enucleation aims to minimize normal or healthy renal parenchyma by excising the tumor along the pseudocapsule. Enucleation may preserve normal parenchymal mass and renal function compared with resection technique. 8,20 –22 A universal reporting system for excision technique had been lacking. After the introduction of SIB margin score, many studies based on this score have been reported, showing its versatility. 10 –14 We also utilized this score, presuming that it is the optimal assessment tool to enable standardized reporting of specific tumor contact surface.
Meanwhile, reports focusing on which tumor surface lesions to preserve are limited. Theoretically, the original idea of enucleation is to dissect “along” the pseudocapsule; therefore, performing enucleation in the surface area when no or minimal pseudocapsule can be visualized is hypothesized to be technically challenging. In the early external validation of SIB margin score, 30% of the originally resection-intended procedure eventually turned into enucleation in the later part of dissection. 10 The reason why enucleation evaluated only by intermediate and base portion is optimal requires further validation. Some possible explanations may be preservation of the renal pelvis and prevention of damage to segmental arteries, in addition to saving normal renal tissues. Nevertheless, this does not necessarily mean that parenchymal preservation at the surface portion can be omitted. As such, we aim to limit the surgical margin to 3 to 5 mm even in cases when the surface score is evaluated as 1.
Similarly, profile of tumor in which enucleation advantage can be maximized has not been clearly elucidated. Our results showed that enucleation helped preserve renal function, particularly in complex tumors, and consequently served to improve trifecta attainment. This is partly in line with a previous report by Lu and colleagues, which showed inverse relationship between preoperative aspects and dimensions used for an anatomical score and trifecta achievement rate. 23 We previously reported that larger tumor contact surface area is associated with more parenchymal volume loss in RAPN. 15 As more vascularized renal parenchyma is likely to be included in tumors with high RNS (large diameter, hilar, and median polar location), a running suture for kidney reconstruction owes unavoidable risk of compromising intrarenal vascular anatomy. 24,25 Thus, it is reasonable to presume that efforts to preserve any little volume of parenchyma for these tumors are crucial to prevent acute kidney injury or CKD. However, the impact of the dissecting technique seemed relatively small in patients with low complexity tumors, but the difference was statistically significant (−1.1% vs −4.4%, p = 0.005). Whether the patients in this group truly enjoy the clinical benefit needs further consideration.
For negative surgical margin, data imply that it can be limited to as small as 5 to 10 mm or even <1 mm5. In this study, positive margin was observed only in 10 (3.2%) of the entire I/B-E cohort and 6 (1.6%) of the I/B-R cohort, with no significant difference observed. This finding is comparable to previous reports, adding new data to the oncological safety of enucleation. 7,21 Enucleation can be performed without compromising recurrence or long-term survival. 1 Taken together, oncological control does not seem to be harmed by the I/B-E technique.
Regarding surgical complication rate, no difference was observed between the groups in all RNS category subgroups. Whether dissection strategy has any effect on this important outcome remains controversial. Some studies, including ours, reported lower incidence of complications in the enucleation group. 8,9 At any rate, the complication rate itself was low (any grade: 2.5%) for enucleation, which is in line with other reports claiming the technique's safety. 6,12,26 We believe that this technique is feasible. 8,9,12 Based on the SIB margin score, 44.4% of our original cohort was identified as I + B total 1 or less, indicating that a very strict enucleation was performed in this section. As mentioned above, this was performed without compromising the surgical margin or increasing the complication rate, consequently contributing to the increase in trifecta attainment rate. These data suggest that performing enucleation at the intermediate to base portion, that is, after visualizing the pseudocapsule, is practical, at least by experts' hands.
Several factors affected our decision to perform enucleation in this study. Tumors with relatively smooth configuration were considered to be good candidates. A large mass with evident pseudocapsule was another criterion. Large tumors tend to have larger contact surfaces on excision, which is associated with renal mass loss. 15 Moreover, according to our previous study, larger-diameter tumors (i.e., ≥30 mm) are highly likely to be surrounded by pseudocapsules. 27 In such tumors, enucleation is speculated to be easy and safe. However, pseudocapsules were detected pathologically in only 53% of chromophobe renal cell carcinoma. This indicates that enucleation might be difficult if this pathology is suspected preoperatively. We believe that oncological control should be prioritized in all cases; thus, enucleation should be avoided in this situation. We claim that enucleation at the I/B portion should always be considered and offered as an option in patients with larger or high RNS complexity renal tumors.
Our study has some limitations. First, it is a retrospective study performed at two tertiary institutions, possibly raising concerns for patient selection bias. Second, all surgeries (i.e., RAPN) were performed by highly experienced surgeons, with experience of >100 RAPNs. Whether our results can be applied to other situations, not similar to ours, is unknown. Finally, long-term results, including patient survival, kidney function after several years, and attributing chronic complications, such as cardiovascular disease and hypertension, were not available. Further prospective studies evaluating these outcomes, ideally with long follow-up periods, are warranted to confirm the observed benefits.
Conclusion
Enucleation at the intermediate to base portion in RAPN contributes to the preservation of renal function, with the impact more emphasized in complexed tumors. This was performed without compromising safety. Further studies are required to support our results.
Footnotes
Authors' Contributions
Y.I.: study concepts and designs, acquisition, analysis and interpretation of the data, and article preparation. T.K.: study concepts and design, analysis and interpretation of the data, and article editing. H.T.: article review. K.Y.: article review. T.T.: article editing and review. J.I.: article review. K.T.: article review.
Acknowledgments
The authors thank Ms. Nobuko Hata (Department of Urology, Tokyo Women's Medical University) for her secretarial work.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.