
Abstract
Background:
The surgical techniques and devices used to perform radical cystectomy have evolved significantly with the advent of laparoscopic and robotic methods. The da Vinci® Single-Port (SP) platform (Intuitive Surgical, Inc., Sunnyvale, CA) is an innovation that allows a surgeon to perform robot-assisted radical cystectomy (RARC) through a single incision. To determine if this new tool is comparable to its multiport (MP) predecessors, we reviewed a single-surgeon experience of SP RARC.
Materials and Methods:
We identified patients at our institution who underwent RARC between August 2017 and June 2020 by one surgeon at our institution (n = 64). Using propensity scoring analysis, patients whose procedure were performed with the SP platform (n = 12) were matched 1:2 to patients whose procedure was performed with the MP platform (n = 24). Univariable analysis was performed to identify differences in any perioperative outcome, including operative time, estimated blood loss (EBL), lymph node yield, 90-day complication/readmission rates, and positive surgical margin (PSM) rates.
Results:
Patients who had an SP RARC on average had a lower lymph node yield than those who had an MP RARC (11.9 vs 17.1, p = 0.0347). All other perioperative outcomes, including operative time, EBL, 90-day complication rates, 90-day readmission rates, and PSM rates, were not significantly different between the SP and MP RARC groups.
Conclusions:
Based on their perioperative outcomes, the SP platform is a feasible alternative to the MP platform when performing RARC. The SP's perioperative outcomes should continue to be evaluated as more SP RARCs are performed.
Introduction
Robot-assisted radical cystectomy (RARC) has been shown to provide perioperative benefits typically associated with minimally invasive surgery. These benefits include reduced incisional pain, blood loss, and length of stay when compared to open approaches. 1 Furthermore, RARC is associated with noninferior oncologic outcomes with regard to progression-free survival rates at 3 years. 2 These studies have been based on multiport (MP) platforms where each robotic arm and camera requires its own surgical incision and port.
The da Vinci® Single-Port (SP) platform (Intuitive Surgical, Inc., Sunnyvale, CA) allows RARC to be even less invasive than the conventional MP approach. The SP platform provides the surgeon access to three multijointed robotic arms and a multijointed camera, all of which fit through a single 25 mm channel. The feasibility of performing both RARC and urinary diversions with this system has been previously described. 3,4
Although it shares goals and design choices with its predecessors, the SP platform is not a direct translation of the MP platforms. The addition of joints to the bodies of laparoscopic instruments allows surgeons to operate through a single port, although minimizing instrument clashing. However, the lack of a second joint directly at the wrists of these instruments requires additional working space for some motions. 5 We hypothesize that the use of an SP platform during RARC may impact perioperative outcomes when compared to conventional MP RARC because of differences in each platform's design and functionality.
A comparative cohort between MP RARC and SP RARC is necessary to evaluate the perioperative outcomes of this new surgical tool. To evaluate these outcomes, we reviewed 12 consecutive SP RARCs within a single-surgeon series and compared their perioperative outcomes to a propensity-matched cohort of patients who underwent MP RARC.
Materials and Methods
Subjects
After Institutional Review Board approval was granted, we reviewed the medical records of patients who underwent RARC with an ileal conduit or neobladder diversion from August 2017 to June 2020 performed by a single surgeon, who has 3 years of post-training experience with the da Vinci MP platform and a caseload of over 90 RARCs. We identified 12 patients who underwent SP RARC and 52 patients who underwent MP RARC.
Propensity matching
To reduce the impact of known clinical predictors of perioperative outcomes, we used nearest neighbor (1:2) propensity score matching to pair those who underwent SP RARC with patients who underwent MP RARC. Matching was based on the patient's age, sex, body mass index (BMI), T stage after transurethral resection of bladder tumor (TURBT), prior history of pelvic surgery, prior history of radiation, use of neoadjuvant chemotherapy, and type of urinary diversion. 6 –9 The final cohorts included 12 patients who underwent SP RARC and 24 patients who underwent MP RARC.
SP RARC surgical technique
Port placement and docking
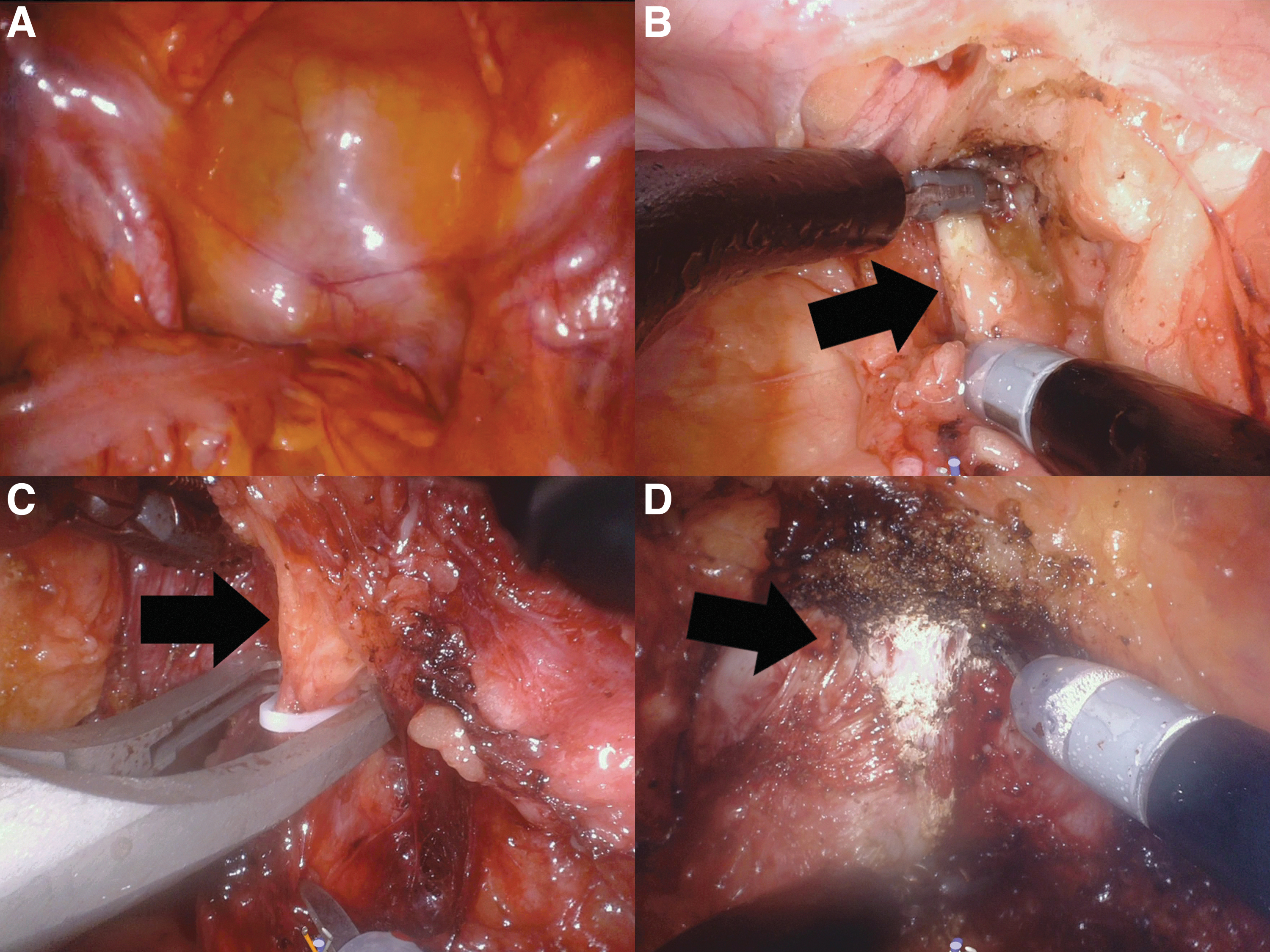
The initial straight in placement of a midline SP trocar is accomplished with an open Hasson technique. 10 A 12 mm AirSeal® assistant port is placed in the left lower quadrant. The da Vinci SP robot is docked (Fig. 1A) and loaded with fenestrated bipolar forceps in channel 1, Cadiere forceps in channel 2, and monopolar curved scissors in channel 3. These instruments are used until the creation of the ureteral-bowel anastomoses.
Extirpative RARC steps.
Extirpative portion of RARC
The extirpative portion of SP RARC is performed as previously described for MP RARC. 11 Briefly, the left ureter is identified at the confluence of the bifurcation of the common iliac and the vas deferens. The ureter is dissected free caudad to the level of the bladder. Weck® Hem-o-lok® clips are applied to the distal ureter, which is then divided (Fig. 1B). This is repeated for the right ureter.
For female patients, the gonadal vessels are controlled with Weck Hem-o-lok clips and the broad and round ligament are controlled with bipolar electrocautery and subsequently divided. Utilizing a ringed forceps with a sponge in the vagina, an incision is made over the posterior peritoneum at the level of the cervix. Once the sponge is visualized after entry into the vaginal canal, the bladder pedicles are taken with a combination of Weck Hem-o-lok clips and bipolar electrocautery. The endocervical fascia is dissected laterally and the space of Retzius is developed. The anterior vagina and urethra are dissected free using electrocautery dissection.
For male patients, the posterior reflection of the peritoneum is divided to expose the seminal vesicles and the distal vas deferens. Denonvilliers' fascia is identified and bluntly dissected posteriorly. The medial umbilical ligaments are ligated with Weck Hem-o-lok clips and divided. The pedicles of the bladder are controlled with sequential Weck Hem-o-lok clips and electrocautery dissection (Fig. 1C). Once the endopelvic fascia is encountered, the space of Retzius is developed. A nerve-sparing procedure with minimal opening of the endopelvic fascia is performed for low-risk patients who desire retained erectile function. The dorsal venous complex is then controlled with electrocautery dissection (Fig. 1D). The posterior plane of the dissection is bluntly retracted from Denonvilliers fascia until the urethra is isolated. The urethra is divided sharply. The Foley catheter is brought to the midline, ligated with Weck Hem-o-lok clips and divided, and the rectourethralis muscle is divided. Retraction during the preceding steps is challenging owing to the seemingly reduced grip strength and unique arm constraints on the SP platform.
Pelvic lymph node dissection
The bilateral pelvic lymph node dissection is performed using the genitofemoral nerve, Cooper's ligament, the obturator nerve, and the common iliac artery as boundaries of dissection.
Intracorporeal ileal conduit creation
Ten patients received an ileal conduit through the following steps: a 20 cm segment of distal ileum is isolated 20 cm from the ileocolic junction with two 60 mm tan loads of an Endo-GIA stapler (Medtronic, Minneapolis, MN) through the assistant port (Fig. 2A). The bowel-to-bowel anastomosis is performed in a side-to-side functional end-to-end manner with two 60 mm tan loads performing the side-to-side anastomosis and another 60 mm tan load performing the closure of the segment (Fig. 2B–D).
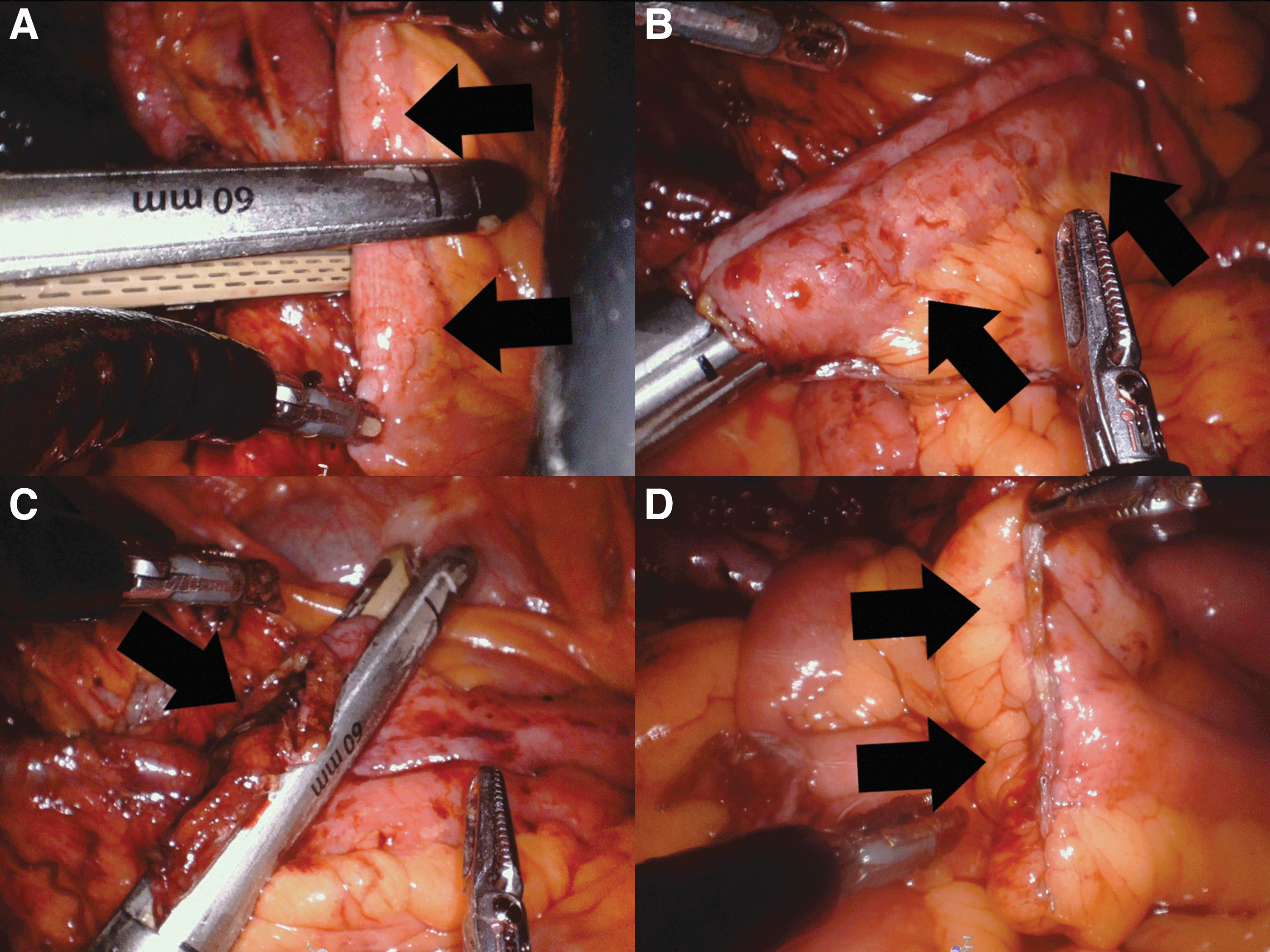
Creation of the ileal conduit and bowel-to-bowel anastomosis. Obtaining the angles necessary to perform this portion of the procedure can be difficult. The images in this study demonstrate the best approach for accomplishing the anastomosis.
The left ureter is tunneled under the sigmoid mesentery and both ureters are widely spatulated (Fig. 3A). An enterotomy is created in the ileal conduit with the monopolar curved scissors. The monopolar curved scissors are removed from channel 3 and replaced with a needle driver. A Bricker ileal ureteral anastomosis is performed with 4-0 Monocryl suture in a running manner (Fig. 3B). A single J stent is placed in the ureter as much as the level of the kidney before completion of the anastomosis (Fig. 3C, D). The needle driver is removed from channel 3 and replaced with the monopolar curved scissors to repeat the creation of an ileal ureteral anastomosis for the remaining ureter. The pelvis is then irrigated with antibiotic solution and the distal end of the conduit is marked with a 2-0 Vicryl suture.
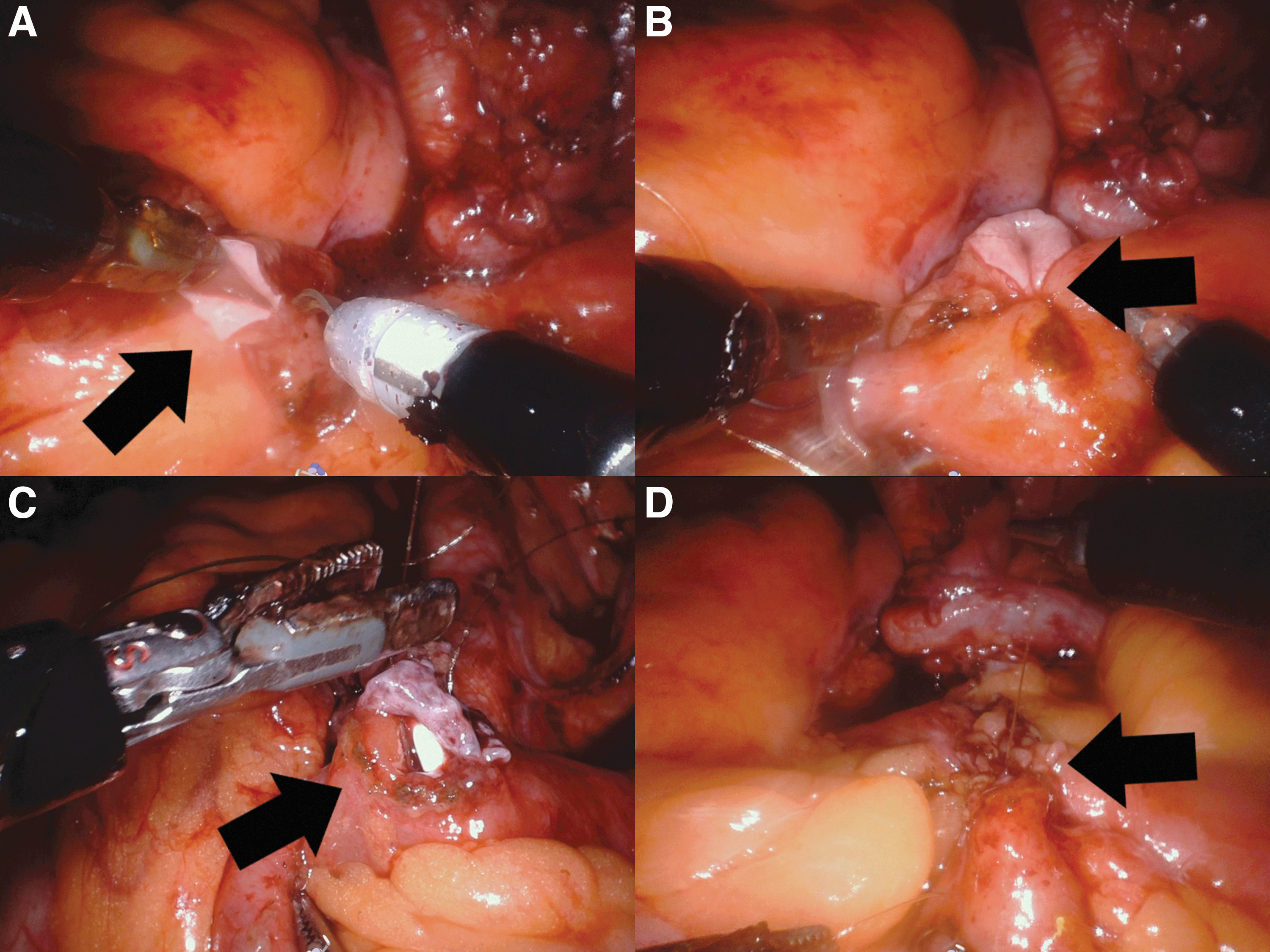
Creation of the ileal ureteral anastomosis.
The distal end of the conduit is brought as much as the right upper quadrant (Fig. 4A). The trocars are removed. After excision of the skin, the ostomy is matured using 2-0 and 3-0 chromic suture in a Bricker manner (Fig. 4B–D). 12

Intracorporeal neobladder creation
Two patients received orthotopic neobladders. Neobladder creation was performed as previously described for MP RARC. 11 Briefly, a 60 cm segment of distal ileum is isolated 20 cm from the ileocolic junction with two 60 mm tan loads. The bowel-to-bowel anastomosis is performed in a side-to-side functional end-to-end manner with three 60 mm tan loads. The bowel segment is sewn to the urethral stump with 3-0 V-Loc suture in running manner. The bowel segment is then opened along the antimesenteric border. The back wall of the bowel segment is sewn together with a 2-0 V-Loc suture in running manner. The ureteral-to-neobladder anastomoses are created with a 4-0 Monocryl suture placed in running manner. Single J ureteral stents are placed in both ureters. The ureters are brought to the lower left quadrant. A 4-0 chromic suture is used to purse string the neobladder around the stents. The anterior neobladder is closed with 2-0 V-Loc suture in a running manner. The final Foley catheter is placed through the urethra, and the balloon is inflated to 7 mL. The neobladder is irrigated with 120 mL of normal saline to detect leaks.
Closure and postoperative management of stents and drains
The fascia of the assistant and camera port is closed with 0 Vicryl suture. The skin of the port sites is closed with 4-0 Monocryl suture and reapproximated with Steri-Strip dressings.
Each patient is managed on an Enhanced Recovery After Surgery (ERAS) pathway, which includes an epidural for pain control, minimizes narcotic use, and emphasizes early activity postoperatively. Any drain is monitored and removed on postoperative day 3. Ureteral stents are removed on postoperative day 7 to 10. Patients with neobladders have a cystogram on postoperative day 21 and their Foley catheter is removed if no leak is present.
Perioperative outcome measures
Assessed perioperative outcomes included the following: hospital length of stay, 90-day readmission rate, 90-day complication rate, estimated blood loss (EBL), operative time, lymph node yield, and rate of positive surgical margins (PSMs). Readmissions were defined as having any readmission within 90 days to the operating facility or any associated hospital. Complications were defined as having any Clavien-Dindo Grade II complication or greater within 90 days of surgery. 13
Statistical analysis
Comparisons were made using the chi-square test of independence and Wilcoxon rank-sum test for categorical and continuous variables, respectively, to assess for differences between those who underwent MP vs SP RARC. Statistical significance was defined by a p-value of <0.05. All propensity matching and statistical analysis were done in R, Version 3.6.2.
Results
The baseline clinical characteristics for the patients in this study are summarized in Table 1. No baseline characteristic was significantly different between the two groups after propensity matching, including age, BMI, sex, type of urinary diversion, or T stage after TURBT. There were also no differences in their past medical history for rates of pelvic radiation, pelvic surgery, or neoadjuvant chemotherapy.
Clinical Characteristics and Patient Demographics
BMI = body mass index; MP = multiport; SD = standard deviation; SP = single port; TURBT = transurethral resection of bladder tumor.
Perioperative outcomes are summarized and compared in Table 2. Patients who underwent SP RARC on average had a lower lymph node yield during surgery than MP RARC patients with an average of 11.9 and 17.1 (p = 0.034) lymph nodes, respectively. Length of stay (5.4 vs 5.9 days, p = 0.945), EBL (117 vs 148 mL, p = 0.080), operative time (387 vs 418 minutes, p = 0.247), and rate of PSMs (8.3 vs 4.2%, p = 0.607) were not statistically different between patients who had SP or MP RARC, respectively.
Comparison of Perioperative Outcomes Between Patients Receiving Single-Port Vs Multiport Robot-Assisted Radical Cystectomy
EBL = estimated blood loss.
Discussion
Our single-surgeon propensity-matched cohorts suggest that patients undergoing RARC experience similar perioperative outcomes when the SP or MP robotic platform is used to perform the procedure. Uniquely, lymph node yield is found to be lower for cases with the SP platform. These findings indicate that the SP platform is a comparable and feasible alternative to the MP platform when performing an RARC.
Given that a surgeon is experienced with MP RARC, perioperative outcomes, including PSM, 90-day complication/readmission rate, EBL, operative time, and length of stay during a surgeon's initial experience with the SP platform, have similar outcomes to those patients who undergo MP RARC. Previous studies have shown the learning curve of the MP platform significantly impacts PSM and operative time. 14,15 Although MP cases had a higher average operative time that was not statistically significant, this is likely attributable to the reduced role of surgical trainees during SP cases. Considering this, neither our data nor an investigation into the initial experience of SP robot-assisted laparoscopic prostatectomies (RALP) demonstrated a difference in these perioperative outcomes when comparing cases managed with the SP and MP platforms. 16 This suggests that for surgeons with prior RARC experience, a majority of their perioperative outcomes are not impacted by a learning curve during the initial experience with the SP platform.
When combined with prior reports, our experience suggests that the SP platform is a safe, reasonable alternative to current MP platforms when performing RARC. In a four-patient case series, Kaouk et al. demonstrated the feasibility of the SP platform's use during RARC with no report of Clavien-Dindo Grade II or greater complication within 30 days. 3,4,13 Zhang et al. had similar findings in their four-patient case series, which involved only one Clavien-Dindo Grade II 30-day complication. 13,17 For MP platform-based RARC, previous data indicate that Clavien-Dindo Grade II or greater complication rates at 30 and 90 days can be as high as 50% and 52%, respectively. 1,18 Compared to the MP cohort, the SP platform achieved an overall complication rate of 41.7% at 90 days (p = 1.000), suggesting patients will not likely experience increased rates of complications even during the initial learning period of the SP platform.
Our data suggest that lymph node yield is reduced in RARC where the SP platform is used when compared to the MP platform. RARCs performed with the SP and MP platforms reported average yields of 11.9 and 17.1 lymph nodes, respectively (p = 0.034). Previous literature comparing SP and MP RALPs also revealed a statistically significant difference in lymph node yield of 12 and 14 lymph nodes, respectively (p = 0.012). 16 Further investigation is warranted because lymph node yield is a predictor of disease-free and overall survival. 19,20
It is unclear why lymph node yield is lower in RARCs where the SP platform is used. Both our study and the study examining SP RALP are comparisons between an initial series of SP procedures and a series of MP procedures by a surgeon experienced with the MP platform. 16 This could indicate that a learning curve for pelvic lymph node dissection occurs when surgeons experienced with the MP platform transition to the SP platform for RARC. For a surgeon's initial experience with MP RARC, lymph node yield was shown to increase by sequential case number on average by 4.5 lymph nodes for every 10 patients. 14,15 Our results and published studies on SP RALPs failed to show differences in PSMs and operative times, which are impacted by the learning curve in the initial experience with MP RARC. 16 This suggests that either the reduced lymph node yield is not a learning curve effect or that a learning curve experienced during the MP to SP transition uniquely impacts nodal dissection. A larger series of cases is necessary to determine if this demonstrated difference is reduced through additional SP RARC experience.
Although we believe this is the largest SP RARC series available in the literature, this study is limited by its relatively small sample size and retrospective study design. Specifically, the retrospective design could have introduced bias through the selection of patients for SP RARC, which was at the discretion of the operating surgeon. This source of bias in our study is limited by the propensity matching of subjects that was used to build the comparison MP cohort. Future studies should assess these perioperative outcomes as more SP RARCs are performed.
Conclusions
The SP platform is a comparable and feasible alternative to the MP platform when performing RARC based on their similar perioperative outcomes with the exception of lymph node yield. Further investigation is necessary to determine if these outcomes remain similar and if lymph node yield improves as surgeons perform more SP RARCs.
Footnotes
Author Contribution Statements
J.T.G. and E.H.K. provided substantial contributions to design, data acquisition, data analysis, interpretation of the data, drafting, revising, and final approval of this work and agree to be accountable for all aspects of the work. J.M.V. provided substantial contributions to design, data analysis, drafting, revising, and final approval of this work and agrees to be accountable for all aspects of the work. K.G.S., J.K.P., S.B.B., and R.S.F. provided substantial contributions to design, interpretation of the data, drafting, revising, and final approval of this work and agree to be accountable for all aspects of the work.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This study was supported by an educational grant (P21-04773) from the Midwest Stone Institute (MSI) to James Gross.