
Abstract
Purpose:
To compare the efficacy and safety of plasma kinetic enucleation of the prostate (PKEP) with holmium laser enucleation of the prostate (HoLEP) for treatment of benign prostatic hyperplasia (BPH).
Methods:
A total of 160 patients with indications for the surgical treatment of BPH were randomly assigned to receive either PKEP or HoLEP prospectively. Baseline characteristics, perioperative data, and postoperative outcomes of the patients were recorded. One hundred twenty-six (78.75%) patients (PKEP 64 vs HoLEP 62) completed the 3-year follow-up assessment.
Results:
Patients in both groups had similar baseline characteristics. Compared with PKEP, HoLEP was associated with shorter operative time as well as take-out time, lower perioperative hemoglobin decrease, and shorter bladder irrigation time, catheterization time, and hospital stay time. PKEP was superior to HoLEP in terms of the noise of the machine and hospitalization expenses. There were no significant differences in enucleating time, resected weight, and serum sodium levels. Both groups achieved satisfactory results and maintained improvement from baseline in terms of maximum urinary flow rate (Qmax), International Prostatic Symptomatic Score, quality of life, and postvoid residual at 3-year follow-up, with no significant differences between the two procedures. Except for re-catheterization rate, postoperative data such as transrectal ultrasound volume, International Index of Erectile Function-5, and follow-up scores of the flexible cystourethroscopy results, as well as the acute and mid-to long-term complications after surgery, were statistically similar.
Conclusion:
The 3-year follow-up data of this randomized trial confirmed that both PKEP and HoLEP were effective and safe surgical procedures for the transurethral management of BPH. HoLEP presented certain advantages compared to PKEP, such as reduced operative duration, decreased risk of blood loss, and less bladder irrigation, hospital stay time, and re-catheterization rate, whereas PKEP had lower noise and no additional laser cost. Chinese Clinical Trial Registry (ChiCTR-TRC-13004468).
Introduction
Low urinary tract symptoms (LUTS) secondary to benign prostatic hyperplasia (BPH) have been reported to have a significant negative impact on the quality of life (QoL), with most affected men ultimately opting for minimally invasive therapy or surgical treatment. 1 Since transurethral resection of the prostate (TURP) has been recommended as the gold standard surgical therapy for years, new treatment techniques such as plasma kinetic enucleation of the prostate (PKEP) and holmium laser enucleation of the prostate (HoLEP) showed better results in terms of prostate tissue removal, hemoglobin loss, catheterization time, and shorter length of hospitalization. 2,3 Still, there are not enough studies directly comparing the efficacy and safety of these two techniques. To the best of our knowledge, there has been no randomized study that compared the two procedures with a follow-up period longer than 12 months and that performed cost analysis. 4,5 Therefore, to further demonstrate the medium-term durability of PKEP for the management of BPH in comparison with HoLEP, we conducted this prospective randomized trial.
Methods
Trial design and participants
This study was a prospective, single-blind, randomized, controlled trial of PKEP vs HoLEP. All treatments took place at Shanghai Ninth People's Hospital between May 2014 and April 2016. The patients with LUTS and obstruction because of BPH, who had indications for the surgical treatment, were invited to take part in our study. All participants previously failed conservative medical therapy with α-blockers and 5-reductase inhibitors. The exclusion criteria included patients with severe pulmonary disease or heart disease, bladder calculus, neurogenic bladder dysfunction, bladder cancer, previous prostate surgery, prostate cancer, urethral stricture, or coagulopathy.
Ethical approval was obtained from the Shanghai Ninth People's Hospital IRB. All participants provided informed consent using study-specific forms before any test that went beyond standard care. Figure 1 shows a timeline of the study.
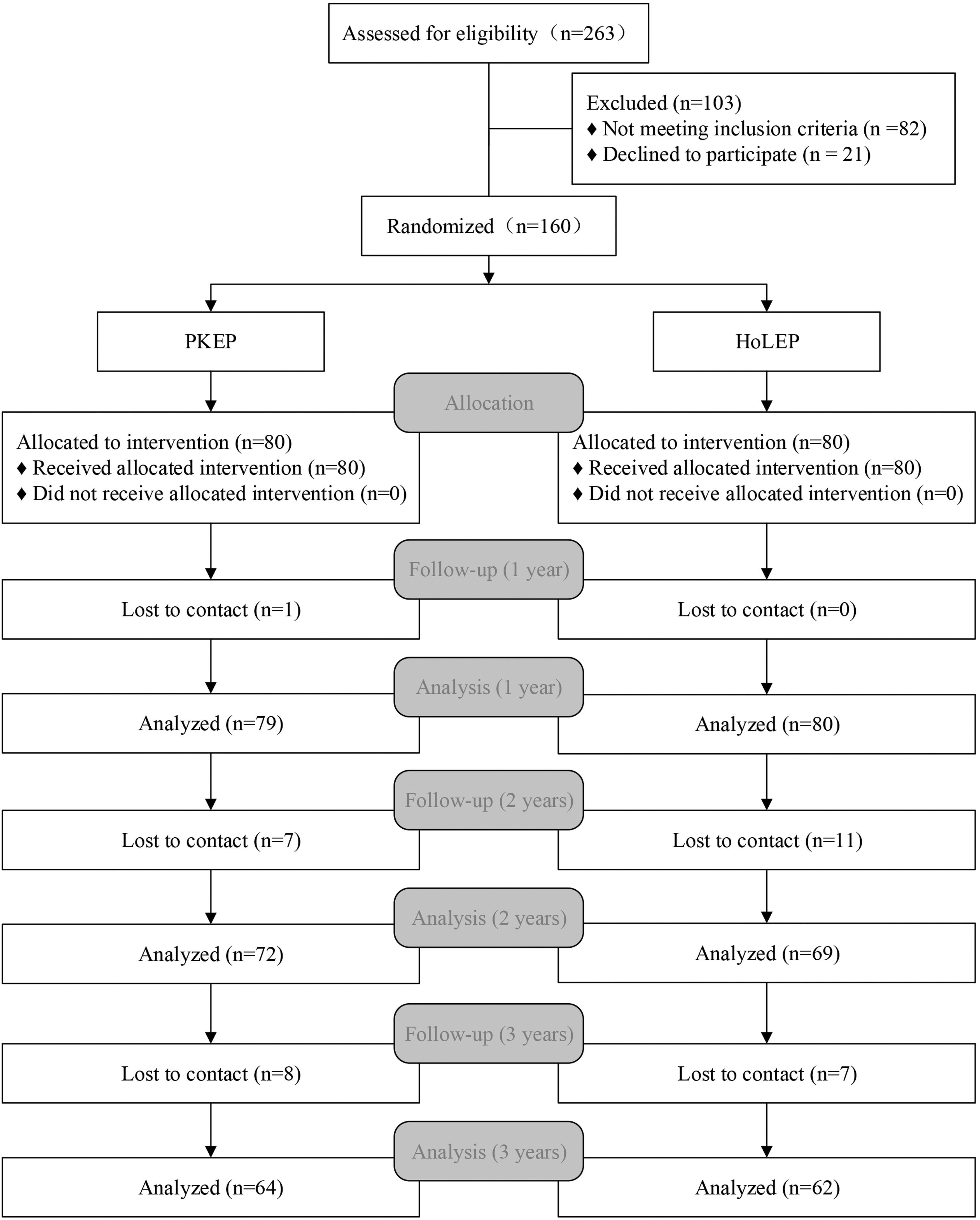
CONSORT flowchart for study participants. CONSORT = consolidated standards of reporting trials; HoLEP = holmium laser enucleation of the prostate; PKEP = plasma kinetic enucleation of the prostate.
Randomization and intervention
In total, 160 patients were randomized to PKEP (80) or HoLEP (80) after ethical approval, and the written informed consent was obtained from all patients. Allocation concealment was done using sequentially numbered and sealed envelopes. Each patient was assigned with an envelope through the computerized random number generator. One week before surgery, all patients stopped using 5-reductase inhibitors, α-blockers, anticholinergics, and anticoagulants.
PKEP was conducted using the ScanMed Plasmakinetic Super Pulse System (ScanMed, Zhuhai, China). The generator for PKEP was set at 80 W for coagulation and 160 W for cutting; there was no need for additional morcellation devices. HoLEP was performed using a 550 μm end-firing laser fiber and a 100 W VersaPulse® holmium laser with power settings at 80–100 W. Transurethral morcellation was performed using a mechanical morcellator (VersaCut™).
All the operations were performed by one surgeon (Z.W.), who was quite skilled in both technologies. All patients received general anesthesia and were in the lithotomy position during surgery. Normal saline (0.9%) was used as the irrigation fluid, and all irrigation bags were hung 60 cm above the operating table. After surgery, an irrigating catheter was inserted. The bladder irrigation was used as necessary, and when the hematuria sufficiently settled, the catheter was removed.
Blinding and follow-up
The study was a single-blinded trial in which only the patients were blinded to the treatments, whereas the surgeons and supervisors were not. A team coordinator and physician performed the follow-up visits. Some items that did not require a hospital examination were completed after telephone consultation.
Outcomes and endpoints
Primary
The primary outcome was the change in micturition function from baseline to the 36th month, measured by the change in maximum urinary flow rate (Qmax).
Secondary
The change from baseline in Qmax at 1, 6, 12, and 24 months was assessed as a secondary endpoint. Additional secondary endpoints included International Prostatic Symptomatic Score (IPSS), QoL, postvoid residual (PVR) volume, and PSA. Furthermore, we recorded the hospitalization expenses, International Index of Erectile Function-5 (IIEF-5), and flexible cystourethroscopy results 6 to evaluate the economic loss, sexual function, and recurrence. Safety evaluations included intraoperative and postoperative adverse events. In addition, a sound-level meter (Control Company, Friendswood, TX, USA) was used for decibel measurements. 7
Sample size
Based on our previous publication, the sample size was determined as mean ± standard deviation (SD) Qmax of 27.3 ± 6.8 for enucleation procedure at the 36-month follow-up. 8 Noninferiority margin δ was defined as 1/2 SD, which means we considered Qmax ≤3.4 mL/s as a predefined accepted equivalence margin. Respective type 1 and 2 statistical errors <5% and <20% accounted for potential 20% dropout rate; therefore, 80 patients were set in each arm.
Statistical analysis
Data were statistically analyzed using the SPSS 21.0 software (Chicago, IL, USA). All measurement data were presented as mean ± SD and statistically analyzed with a two-tailed Student's t-test. Descriptive statistics were reported and analyzed with a Mann–Whitney U-test. The significance threshold for all bivariate analyses was set at a two-sided alpha = 0.05.
Results
Table 1 shows perioperative characteristics of patients, as well as the cost of hospitalization consisting of direct costs (treatment costs, including surgery and anesthesia costs, disposable products costs, and products sterilization costs, drugs, and blood product costs), indirect costs (hospital stay service costs and diagnostics costs), and other costs related to hospitalization. Baseline characteristics showed no significant difference between the PKEP and HoLEP groups in relation to age, PSA, and preoperative prostate volume. Although enucleation time and resected weight were similar between the groups, take-out tissue time and total operative time were significantly shorter in the HoLEP group (p < 0.01, p < 0.001). Compared to plasma kinetic, holmium had less hemoglobin decrease (p = 0.03), bladder irrigation time (p = 0.02), catheterization time (p = 0.01), and hospital stay time (p < 0.001). Serum sodium decrease and indirect costs were comparable between the two groups. However, as shown in Table 1, PKEP showed more favorable results in terms of the noise of the machine, total hospitalization costs, and direct costs (all p < 0.001).
Perioperative Characteristics of Patients
We take that 1 United States dollar equals 7 Chinese yuan as the exchange rate for conversion.
HoLEP = holmium laser enucleation of the prostate; k¥ = thousand-Chinese yuan; k$ = thousand-United States dollar; PKEP = plasma kinetic enucleation of the prostate; PSA = prostate-specific antigen; SD = standard deviation.
The preoperative and 1-, 6-, 12-, 24-, and 36-month postoperative data for the Qmax, IPSS, QoL, PVR, and PSA are shown in Table 2. Compared to baseline levels, both groups showed marked improvements at each interval from 1 month after surgery. However, no significant differences were found in these parameters between the two energy source groups.
Follow-Up Data for Maximum Urinary Flow Rate, International Prostatic Symptomatic Score, Quality of Life, Postvoid Residual Urine, and Prostate-Specific Antigen
PVR = postvoid residual urine; Qmax = maximum urinary flow rate; QoL = quality-of-life score.
We evaluated transrectal ultrasound (TRUS) volume of the prostate and yearly IIEF-5, observing no statistical significance between them. At 3 years after surgery, 47 patients (PKEP 22 and HoLEP 25) volunteered to undergo flexible cystoscopy during a follow-up visit. One of the left or right prostatic cavity walls that were not recovering well (after removal of the prostate gland) were found in two cases in the PKEP group and one case in the HoLEP group, thus suggesting the elasticity or smoothness was not restored, whereas in one case in each group, good prostatic cavity wall recovery and bladder neck construction were absent, which mean these two patients only gained three points. In total, the wounds in most patients recovered well, and there was no noteworthy observation found between the two groups, as shown in Table 3.
Postoperative Data for Transrectal Ultrasound Volume, International Index of Erectile Function-5, and Flexible Cystourethroscopy Results
FC = follow-up scores of the flexible cystourethroscopy results; IIEF5 = International Index of Erectile Function-5; TRUS vol = transrectal ultrasound volume.
Adverse events are listed in Table 4. Six patients from the PKEP group experienced bladder spasm characterized by spastic abdominal pain and urine leakage from around the catheter, compared to one patient in the HoLEP group (p = 0.05). Four patients in the PKEP group required re-catheterization owing to urine retention, whereas there were no cases with urine retention in the HoLEP group (p = 0.04). After catheter removal, 13 patients (PKEP 7 and HoLEP 6) complained of some degree of incontinence, 8 patients (PKEP 5 and HoLEP 3) recovered continence within 1 month, and in the remaining patients, it resolved within 6 months. During the follow-up period, no patient had urethral stricture; however, one patient experienced BNCs at 9 weeks after surgery in the PKEP group and one patient at 8 weeks in the HoLEP group. Retrograde ejaculation occurred in 31.25% of patients in the PKEP group and in 37.10% of patients in the HoLEP group. No reoperation was performed because of recurrence.
Total Adverse Events at 36 Months
Discussion
BPH is a prevalent health condition in elderly men, which has a tremendous impact on patients' QoL. This condition cannot be completely cured by medications; thus, surgical resection is the only potentially curative therapy. 9,10 Although TURP has remained the cornerstone of BPH surgical treatment for more than nine decades, it has some inescapable shortcomings. Consequently, identifying new approaches for replacing TURP is of great importance. Over recent years, relevant research has mainly focused on different energy technology, such as plasma kinetic, holmium laser, green laser, and similar, or on the improvement of surgical procedure, such as the proposal of enucleation. 11 In these methods, PKEP and HoLEP, both suitable for medium and large prostate sizes, are emerging as commonly used techniques and the potential new gold standard that could replace TURP. 12 –16 However, comparisons of mid-term and long-term outcomes achieved by these two techniques are lacking. Thus, we designed this prospective randomized trial to compare PKEP with HoLEP in terms of efficacy and safety.
Our findings indicated that both the PKEP and HoLEP were efficient techniques, and HoLEP was not inferior to PKEP in terms of Qmax within 36 months. To the best of our knowledge, this is the first 3-year follow-up randomized controlled trial with the largest sample size up to now.
As PKEP and HoLEP are both enucleation procedures, no significant difference was observed in LUTS outcomes between the two groups, including PSA. Moreover, LUTS results were durable during the following period, as was expected. No noteworthy difference could be seen in the TRUS volume of prostate follow-up, and the increase in the changing trends of the TRUS data was similar in the two groups. To intuitively evaluate the prostatic cavity's recovery condition after surgery, a scoring system that was previously designed by our team and that ranged from 0 to 5 (higher numbers indicated better recovery) was used. No residual and recurrent adenomas were found in any of the patients, and the general statistical difference between the two techniques was not significant. In short, regardless of the subjective LUTS score or objective auxiliary examination, these two surgical methods were both effective and lasting, generating satisfactory effects.
Surgical efficiency is one of the common concerns of urologists. Our findings revealed that more than 70% of the prostate tissue was enucleated by both techniques. Yet, a significant difference in operative time was noted, with the HoLEP technique achieving better time, regardless of the prostate size. 4,5 In this study, there was no significant difference in enucleation time, and both average enucleation speeds were about 1 g/min. Therefore, the statistical difference in total operation time was mainly attributable to take-out tissue time. Our improved morcellation procedure can address various situations, providing a more fluent process and better efficiency. 17 On the contrary, the suction of the enucleation tissue with Ellik was inferior in the PKEP group.
According to existing literature, patients can benefit from both PKEP and HoLEP compared to those undergoing open prostatectomy (OP) or TURP. 8,14,18,19 In this trial, HoLEP was even superior to PKEP in terms of hemoglobin decrease and bladder irrigation time. Based on our experience, multiple factors lead to less blood loss, such as laser's physical characteristics, clearer operation field, and less bladder spasm. 20 In addition to lower late bleeding after the laser surgery, the shorter bladder irrigation time in the HoLEP group may be related to bladder spasm reduction. However, it is also possible that the usage of a different technique did not cause the occurrence of bladder spasm. There may be some bias here because we did not record preoperative bladder status. As reported, preoperative detrusor functional status was certainly related to bladder spasm in BPH patients after surgery, and patients with detrusor instability were more likely to suffer from bladder spasm, which also tended to be more serious. 21 The longer catheterization time and hospital stay found in the PKEP group might be related to more hemoglobin decrease and bladder irrigation time.
No capsular perforation and mucosal bladder injury were reported. However, it is necessary to further investigate why the PKEP group had a higher re-catheterization rate. Sample size may be one of the reasons. Urinary incontinence is a concerning matter. In this study, a total of 13 patients experienced transitory urge incontinence, whereas no stress incontinence appeared 6 months later. Considering these issues, the rich surgical experience of operating doctors and postoperative pelvic floor muscle exercise might have equal importance.
Sexual dysfunction mainly includes erectile dysfunction and retrograde ejaculation. We indicated that both techniques had no significant impact on IIEF-5 scores. Holmium laser energy has a narrow optical penetration depth, and PKEP has no electric current passing through the body; therefore, both techniques are unlikely to damage nerves traveling just beneath the prostatic capsule. 22 –24 Retrograde ejaculation is another main adverse event that has been reported to occur in as much as 86.2% of patients after HoLEP and in about a half of patients after PKEP. 25,26 In this study, we also observed high retrograde ejaculation rates; however, these were lower than those reported in previous studies. It is possible that inconsistencies in low rates were attributable to the fact that patients without sexual life were regarded as having no retrograde ejaculation during the follow-up period.
Despite no obvious advantage for PKEP in clinical results, the initial outlay for plasma kinetic was cheaper in PKEP. According to previous reports, both PKEP and HoLEP may be cheaper than OP and TURP regarding the length of hospital stay. 27 Still, in China, no significant correlation was reported between the length of hospital stay and costs, revealing no obvious higher indirect cost with a longer hospital stay in the PKEP group. As far as the two techniques are concerned, the main difference in cost was related to the direct cost, that is, ¥2000 (about 285 dollars) of laser costs. Nevertheless, considering other soft tissue applications and the multiuse nature stones, HoLEP also seems to be cost-effective for hospitals and BPH patients with bladder stones. 28 Another advantage was the lower noise of the machine. Noise has been reported to affect both patients and doctors; thus, diminution of intraoperative noise significantly contributed to lowering complications in patients and improving intrateam communication, as well as the well-being of the surgeons in a prospective controlled clinical trial. 29 Although no hearing hazard was observed during HoLEP and hearing protection was not considered mandatory according to Occupational Safety and Health Administration (OSHA) standards, we think that all involved parties could greatly benefit from a quieter environment.
Compared with previous randomized clinical trials (RCTs), our study had a larger sample size and the ability to retain patients for longer follow-up time, as shown in Table 5. The reason why our patients had longer catheterization time was partly attributable to Chinese people's conservative thinking and the fact that the Chinese prefer to remove the catheter as soon as the urine clears, which may explain why the re-catheterization rate was obviously lower in our study. 4 This study has some limitations. First, we did not consider the recovery room time. With reference to blood loss, although Habib et al. 5 found no statistical significance between groups, our results showed a statistical difference. Consequently, future studies with a larger sample size and extended follow-up RCTs are needed to further verify reported findings.
Characteristics and Significant Differences Between Plasma Kinetic Enucleation of the Prostate and holmium Laser Enucleation of the Prostate in Randomized Clinical Trial Studies Up To Now
— = Not available.
Conclusions
Both PKEP and HoLEP resulted as effective and safe procedures for treating patients with BPH at 3-year follow-up. Compared with PKEP, HoLEP presented certain advantages such as reduced operative duration, decreased risk of blood loss, less bladder irrigation and catheterization time, shorter hospital stay, and lower re-catheterization rate, whereas PKEP had a quieter operating environment and no additional laser cost.
Footnotes
Acknowledgments
The authors would like to thank all participants for volunteering to take part in this study.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This work was supported by grants from the Multi-center clinical research project of Shanghai JiaoTong University School of Medicine (DLY201809), Shanghai Huangpu District Industry Support Fund (XK2020011), and National Natural Science Foundation of China (81970656). They did not contribute to the study design, data collection, data analysis, article preparation, and/or publication decisions.