
Abstract
Purpose:
Calcium oxalate (CaOx) stone formation is influenced by urinary oxalate excretion. Stone formers with elevated urinary oxalate are commonly prescribed a low-oxalate diet or oral supplementation with vitamin B6 and magnesium to reduce urinary oxalate excretion. This study aims to compare the effects of dietary modification vs supplementation vs a combination of both on urinary oxalate.
Materials and Methods:
We enrolled patients with a documented history of CaOx stones and newly diagnosed idiopathic hyperoxaluria. Patients were randomized into three treatment groups: low oxalate diet (D), supplementation with 25 mg vitamin B6 and 400 mg magnesium oxide (S), or both low oxalate diet and B6/magnesium supplementation (DS). Baseline and 3-month postintervention 24-hour urine tests were obtained. The primary endpoint was change in 24-hour urinary oxalate (Ox24) at 12 weeks. Secondary endpoints included changes in other 24-hour urine parameters, compliance rates, and adverse effect rates.
Results:
In total, 164 patients were recruited and 62, 47, and 55 were enrolled into the D, S, and DS groups, respectively. Of these, 99 patients completed the study (56.5% of the D, 72.3% of the S, and 54.6% of the DS groups, respectively). Significant differences were noted in median percent reduction in Ox24 values (−31.1% vs −16.0% vs −23.9%, p = 0.007) in the D, S, and DS groups, respectively. Furthermore, the percentages of patients within each treatment arm who realized a decrease in Ox24 were also found to be significantly different: D = 91.4% vs. S = 67.6% vs DS = 86.7%, p = 0.027. No significant adverse events were observed in any of the study arms.
Conclusion:
Low oxalate diet is more effective than B6/magnesium supplementation at lowering urinary oxalate in idiopathic hyperoxaluric stone formers. Combination therapy did not produce greater reductions in urinary oxalate than either of the monotherapy arms suggesting it is of little clinical utility. Further study with long-term longitudinal follow-up is required to determine if these treatment strategies reduce recurrent stone events in this population.
Introduction
Nephrolithiasis is a common and burdensome illness with an incidence of 8.8% in the United States. 1 Kidney stones recur in ∼50% of patients 1 making recurrence prevention crucial to management strategy. The most common kidney stone type by composition is calcium oxalate (CaOx). 2 Although the pathophysiology of nephrolithiasis is poorly understood, 24-hour urine abnormalities such as hypercalciuria, hypocitraturia, and hyperoxaluria have been strongly associated with an increased risk of CaOx nephrolithiasis. 3 Accordingly, treatments aimed at normalizing these urinary parameters are a cornerstone of the medical management of kidney stones.
Indeed, options for CaOx stone prevention include thiazide diuretics for hypercalciuria, potassium citrate supplementation for hypocitraturia and low urinary pH, and a low oxalate diet for hyperoxaluria. 3 However, there is debate surrounding the impact of dietary oxalate on urinary oxalate excretion, 3 and given the wide variety of oxalate containing foods, compliance with a low oxalate diet may be challenging. Two potential pharmacologic interventions that have shown promise for the treatment of hyperoxaluria are pyridoxine (also known as vitamin B6 [B6]) and magnesium supplementation. Nondietary oxalate derives from the conversion of glyoxylate to oxalate by lactate dehydrogenase in the liver. B6 targets this pathway by serving as a cofactor for the enzyme alanine:glyoxylate aminotransferase that converts glyoxylate to glycine, reducing the amount of glyoxylate substrate available to be converted to oxalate. 4 Magnesium is believed to target oxalate absorption by binding oxalate in the intestine. 5 A combination of B6 and magnesium can, therefore, target the pathways of oxalate production and absorption, respectively.
To our knowledge, a limited number of studies have prospectively evaluated the effect of a low oxalate diet on oxalate excretion, 6,7 and only one randomized controlled trial (RCT) has been performed in hyperoxaluric CaOx stone formers (and the study was limited by a small sample size of only 41 patients). 6 In addition, there are no RCTs on the use of B6 and magnesium supplementation in hyperoxaluric stone formers. In light of these gaps in the existing literature, in this study, we seek to conduct an RCT comparing the use of B6/magnesium supplementation with low oxalate diet in hyperoxaluric CaOx stone formers.
Materials and Methods
Patient cohort
After Institutional Review Board approval (HS# 15-00873), patients were recruited from a high-volume outpatient kidney stone center of a major tertiary referral center from December 2015 to February 2019. Study inclusion criteria were as follows: documented history of CaOx stone formation (defined as stone composition >50% CaOx on infrared spectroscopy stone analysis), newly diagnosed and untreated idiopathic hyperoxaluria (defined as 24-hour urinary oxalate [Ox24] ≥40 mg/day with no evidence of primary or enteric hyperoxaluria), age ≥18 years, and ability to provide informed consent. Baseline 24-hour urine studies were conducted within 30 days before enrollment. Exclusion criteria were as follows: documented history of gastric or intestinal bypass, liver disease, history of gastrointestinal malabsorptive disease (i.e., Crohn's disease, ulcerative colitis, and short-gut syndrome), use of B6 or magnesium supplements at time of initial diagnosis/recruitment, documented history of peripheral neuropathy, and acute or chronic renal insufficiency (defined as creatinine [Cr] >1.4 at the time of diagnosis/recruitment).
Study interventions
Patients were randomized into one of three 12-week therapeutic groups: dietary modification (D), vitamin supplementation (S), or combination therapy (DS). Simple randomization was utilized to make group assignments using
The relationship between diet and urinary oxalate excretion is complex and multifactorial. Although modulating calcium intake has been shown to impact urinary oxalate, 3 our study aim was to evaluate the low oxalate diet. Accordingly, instructions regarding dietary modifications focused on oxalate restriction and no recommendations were made regarding other vitamins and minerals. One notable exception is vitamin C intake, as vitamin C is a commonly used supplement and oxalate is a direct metabolic by-product of vitamin C. 3 We advised patients not to exceed >100 mg/day of vitamin C supplementation (no recommendations were made regarding dietary vitamin C).
All patients underwent initial 24-hour urine studies before initiating therapy (Litholink® Corporation, Chicago, Illinois, USA). Twenty-four-hour urine studies contained the following parameters: volume, supersaturation of calcium oxalate (SSCaOX), calcium (Ca24), oxalate (Ox24), citrate (Cit24), supersaturation of calcium phosphate, pH, supersaturation of uric acid, uric acid (UA24), sodium (Na24), potassium (K24), magnesium (Mg24), phosphorus (P24), ammonium, chloride (Cl24), sulfate (S24), urea nitrogen (UUN24), protein catabolic rate, and Cr.
At 6 weeks after enrollment, all patients were contacted by a member of the research team through telephone to assess for self-reported treatment compliance and any adverse effects of therapy. In addition, all patients receiving vitamin supplementation underwent basic metabolic panel testing to assess for the interval development of any electrolyte abnormalities or changes to renal function. Any such changes or abnormalities would prompt cessation of vitamin supplementation and exclusion from the study. At 12 weeks, all patients were instructed to complete a follow-up 24-hour urine study. Patients were then evaluated by the treating physician in clinic to again assess for compliance and any adverse effects, and to review the follow-up 24-hour urine study findings with the patient. Compliance status was determined by patient self-reporting and was evaluated at both 6 weeks (through phone call check-in by our research team) and 12 weeks (through follow-up appointment with the treating physician). If the patient reported noncompliance at either of these two time points, they were categorized as noncompliant. Patients who self-reported noncompliance with study protocol had treatment stopped because of adverse effect or did not complete follow-up 24-hour urine testing were excluded from final analysis. In addition, any patient who had a Cr24/kg value outside the following range, men 18–24 mg/[kg·day] and women 15–20 mg/[kg·day], was deemed an over- or under-collection and subsequently asked to repeat a 24-hour urine. These ranges were selected as they are the reference range utilized by the laboratory performing the 24-hour urine analysis. 10
Outcome measures/statistical analysis
The primary endpoint of the study was change in Ox24 at 12 weeks compared with baseline between the three groups. Secondary endpoints included changes in other 24-hour urine parameters, evaluation of compliance rates, and adverse effect rates between the three groups over the 12-week study period. Before enrollment a power analysis was conducted to determine the minimum number of patients in each treatment arm to achieve a Cohen's d ≥ 0.8 that revealed an n ≥ 45 patients per group was required.
Baseline patient characteristics were compared between the three groups using a Kruskal–Wallis test for continuous variables and chi-square analysis for categorical variables. As not all 24-hour urine data were normally distributed, nonparametric tests were utilized. A Kruskal–Wallis test was used to compare differences in baseline, endpoint, and change (endpoint minus baseline) in 24-hour urine parameters between the three groups. Significant differences (p < 0.05) in univariate testing were evaluated further in post hoc testing using pairwise comparisons with a Bonferroni corrected p-value.
Group compliance was assessed using Pearson's chi-square test. To assess potential interactions between age and gender with compliance, a Kruskal–Wallis test and Pearson's chi-square test were used, respectively, across patients who completed the study vs those who did not. A multivariate regression was used to determine if treatment group independently predicted change in oxalate when controlling for urinary magnesium. All statistical analyses were two-tailed and performed using SPSS v.24 (SPSS, Inc., Chicago, IL, USA); graphs were generated with GraphPad prism v.7 (GraphPad Software, San Diego, CA, USA).
Results
Demographic data
Among the 3251 patients screened for enrollment, 640 (19.7%) met inclusion criteria and 164 (5.0%) consented to participate and were enrolled. The D group included 62 patients, the S group had 47 patients, and DS group included 55 patients. There were no significant differences in age, body mass index, or gender distribution between the three groups (Table 1).
Demographic Data Across Individual Study Cohorts
Median (interquartile range).
Kruskal–Wallis test.
Chi-square test.
BMI, body mass index.
24-Hour urinalysis
Univariate analysis of 24-hour urinary lithogenic profile stratified by treatment arm are reported in Table 2. At baseline, the median Ox24 values across the D, S, and DS groups were 49.6, 49.7, and 53.6 mg/day, respectively (p = 0.2). No significant difference was noted between final median Ox24 values (D = 37.0 mg/day vs S = 40.7 mg/day vs DS = 38.9 mg/day); however, absolute change in median Ox24 from baseline to 12 weeks was found to be significant (D = −15.6 mg/day vs S = −7.3 mg/day vs DS = −12.7 mg/day, p = 0.017). These data are visually represented in Figure 2. Similarly, significant differences were noted in median percent reduction in Ox24 values (−31.1% vs −16.0% vs −23.9%, p = 0.007) in the D, S, and DS groups, respectively (Fig. 3). Furthermore, the percentages of patients within each treatment arm who realized a decrease in Ox24 were also found to be significantly different: D = 91.4% vs S = 67.6% vs DS = 86.7%, p = 0.027. Bonferroni post hoc analysis was used to determine individual associations and revealed a significant difference between the D and S group only (Bonferroni corrected p-value <0.017).
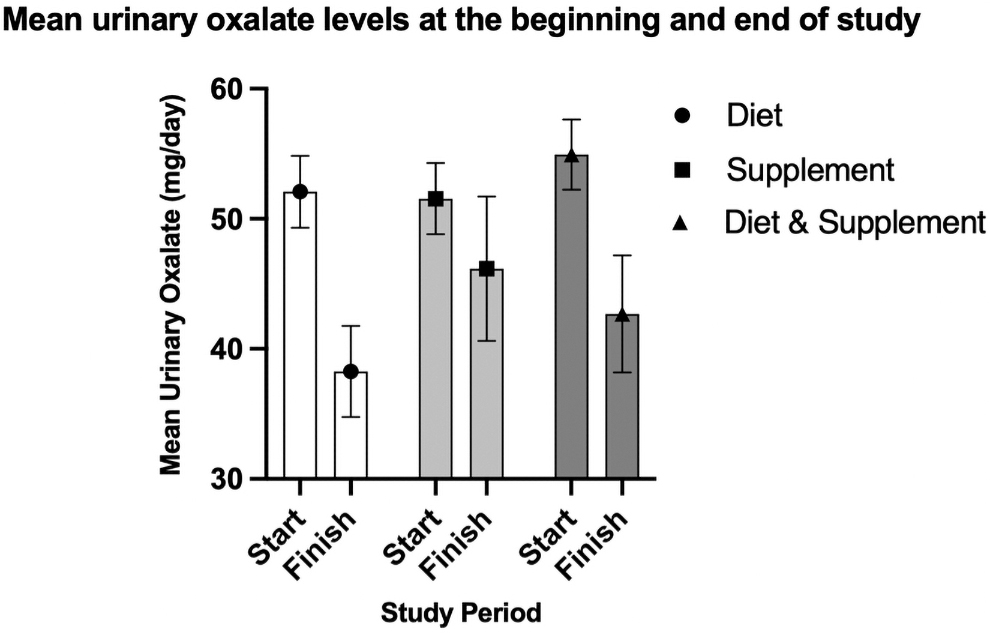
Urinary oxalate levels at the beginning and end of the study.
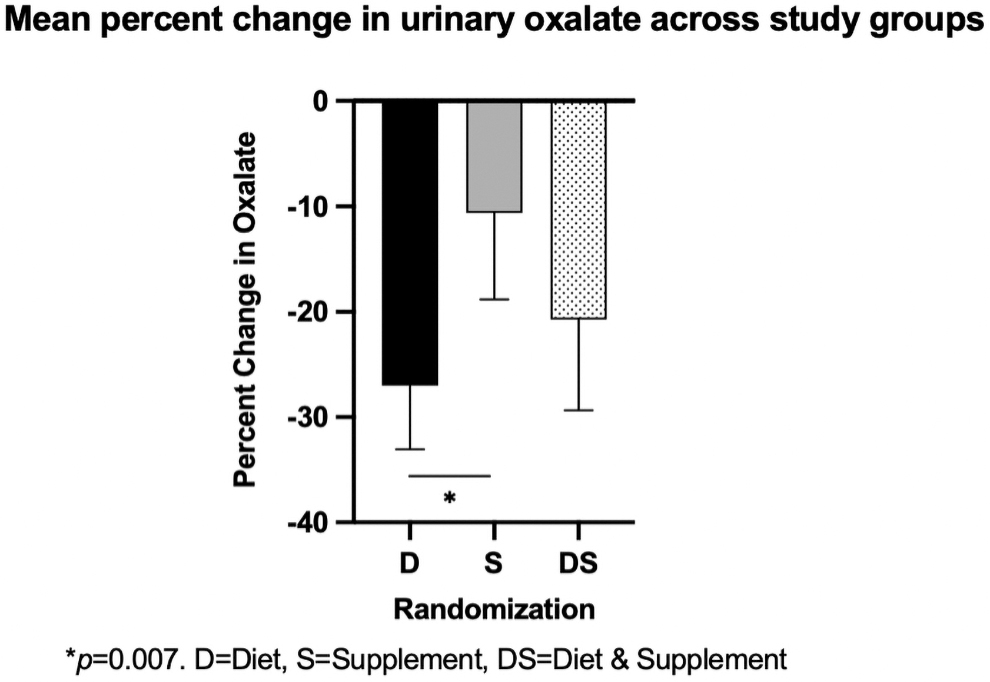
Median percent change in oxalate during study for each group.
Univariate Analysis of 24-Hour Urinary Lithogenic Profile Stratified by Treatment Arm
Bold values denote significance.
.aKruskal–Wallis test.
Significant difference between diet and supplement groups.
Significant difference between diet group and diet and supplement group (Bonferroni corrected p < 0.017).
Significant difference between supplement group and diet and supplement group (Bonferroni corrected p < 0.017).
Ca = calcium; CaOx = calcium oxalate; Cit = citrate; Cr = creatinine; Mg = magnesium; NA = sodium; Ox = oxalate; SS CaOx = supersaturation of calcium oxalate; SS CaP = supersaturation of calcium phosphate; SSUA = supersaturation of uric acid; UA = uric acid.
In addition, in a multivariate analysis of change in Ox24 between treatment arms controlling for urinary magnesium, a significant mean difference was noted between D and S groups (b = 9.37; 95% confidence interval: 2.6–16.1, p = 0.007) with diet held as a referent. Neither DS nor change in Mg24 were found to independently predict change in Ox24, p = 0.447 and p = 0.773, respectively.
Treatment compliance and adverse events
Of the 164 patients, 99 completed the study, 6 withdrew, and the remaining 59 failed to complete the second 24-hour urine test, failed to follow-up, or were noncompliant with the prescribed regimen (Fig. 1). In a comparison of study completion across individual groups, 56.5% of the D, 72.3% of the S, and 54.6% of the DS groups completed the study. Noncompliance was highest in the DS group (20.0%), the D group (16.1%), and the S group (10.6%). Lost to follow-up rate was highest in the D group (25.8%), followed by the DS group (20.0%), and the S group (12.8%). In contrast, study withdrawal rates were higher in the combination group at 5.5% compared with 1.6% in the diet group and 4.3% in the supplement group. In the DS group, two patients withdrew because of gastrointestinal discomfort (diarrhea), and one patient withdrew because of headaches. In the S group two patients also withdrew because of gastrointestinal discomfort, and in the D group one patient withdrew because of unintended weight loss. No significant difference in compliance data was found between groups (p = 0.371; Table 3 and Fig. 4).
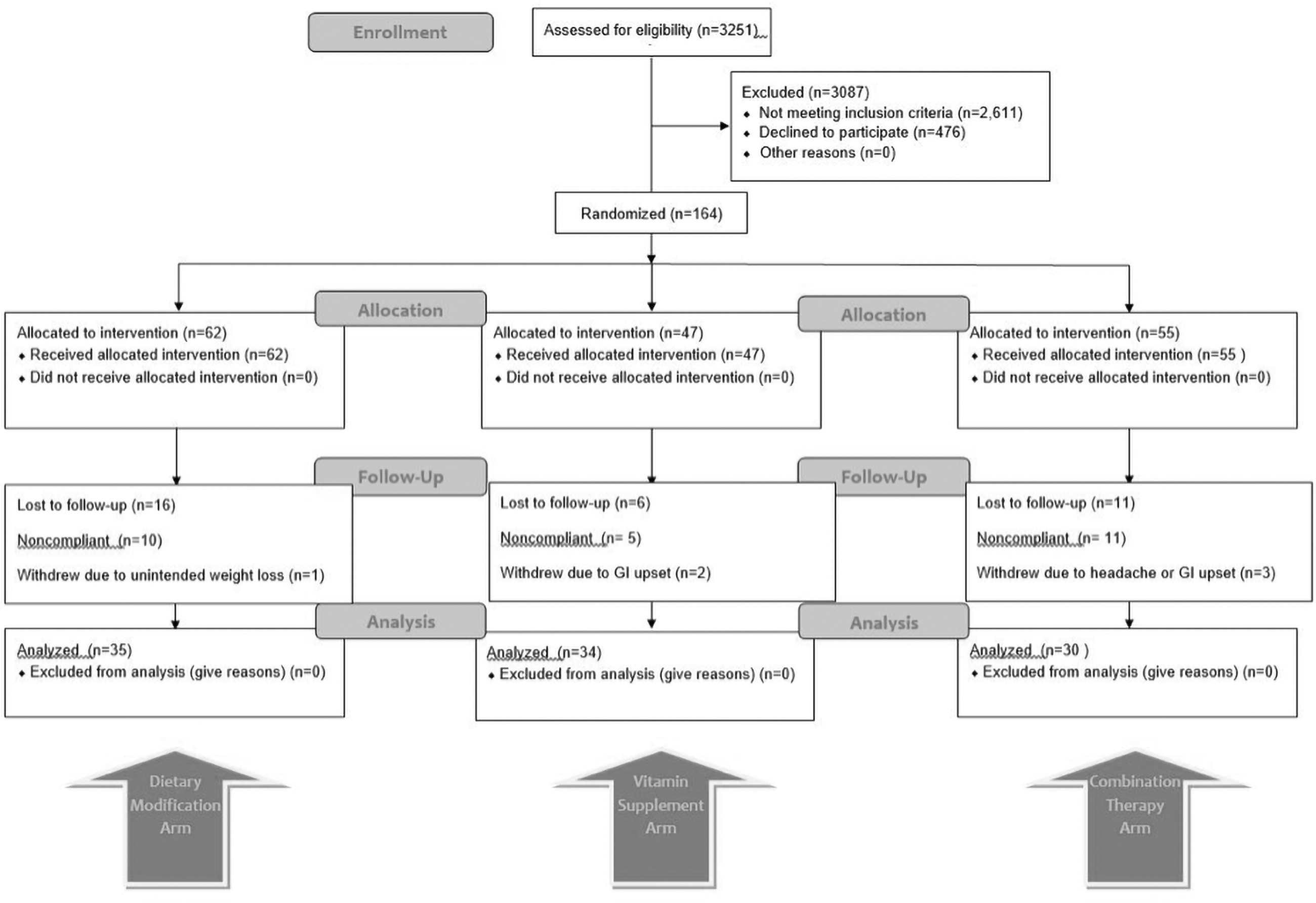
CONSORT flow diagram. CONSORT, Consolidated Standards of Reporting Trials.
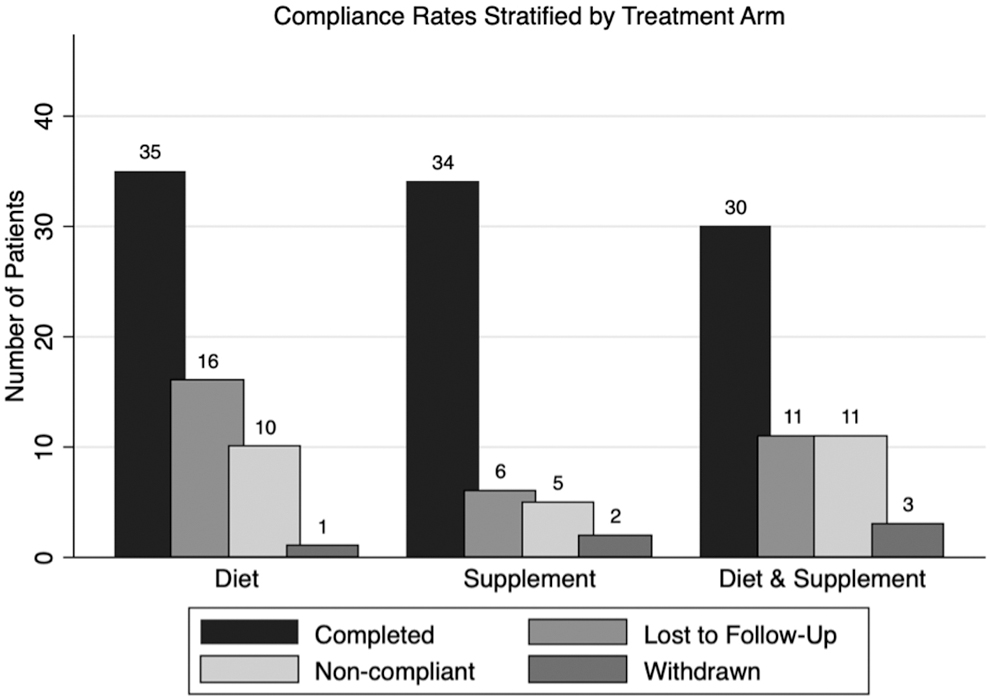
Compliance rates stratified by treatment arm.
Comparison of Compliance Between Individual Study Cohorts
Two subset analyses were performed to determine interactions between demographic data and group compliance. For compliant subjects median ages were 62, 61.5, and 56.5 years in the D, S, and DS groups, respectively, and men accounted for 71.4%, 76.4% and 70% of patients in these groups, respectively. For patients who did not complete the study, median ages were 53, 57, and 55 years, and men accounted for 81.5%, 76.9%, and 76% of patients, respectively. Neither age nor gender were found to be significantly different across any group.
Discussion
To our knowledge, this is the first RCT comparing the effects of a low oxalate diet with B6/magnesium supplementation on 24-hour urine parameters in hyperoxaluric CaOx stone formers. We found restricting dietary oxalate to be more effective than B6/magnesium supplementation in reducing Ox24 in hyperoxaluric CaOx stone formers. Although all three study groups saw a decrease in Ox24, the diet group saw the greatest decrease. In post hoc testing, the decrease in Ox24 in the D group was significantly larger than of the S group. Furthermore, a decrease in SSCaOx was observed in both the D and DS groups, but not the S group.
Prior studies on the use of a low oxalate diet for idiopathic hyperoxaluria have brought mixed results. One study demonstrated that the contribution of dietary oxalate to urinary oxalate excretion is significant, ranging from 24% to 52%, and that dietary oxalate restriction may play an important role in the prevention of CaOx stones. 11 Contrarily, a separate study found that participants in the highest quartile of dietary oxalate consumption only excreted 1.7 mg more urinary oxalate per day compared with those in the lowest quartile of oxalate consumption, suggesting that dietary oxalate is a minor contributor to urinary oxalate. 12 In an RCT examining the effect of probiotic use on urinary oxalate excretion, Lieske et al. indirectly found that a low oxalate diet decreased urinary oxalate. All participants were placed on a low oxalate diet for a 1 week run-in period and found to have a decrease in Ox24 and SSCaOx before subsequent intervention. 7 The only RCT on dietary oxalate restriction for hyperoxaluria compared a low oxalate diet to a Dietary Approaches to Stop Hypertension (DASH) diet and found that whereas the low oxalate group had lower urinary oxalate, the DASH group had lower SSCaOx. 6 Notably, as in our study, the authors found that the low oxalate diet group did have a decrease in SSCaOx, although not as large in magnitude as in the DASH diet group (−0.90 vs −2.14, respectively). 6
Regarding B6 and magnesium supplementation, prior studies have suggested that these supplements may help reduce urinary oxalate. Indeed, two small single cohort studies found that the use of B6 supplementation reduced Ox24. 13,14 Furthermore, a retrospective analysis found that treatment with combined dietary modification and B6 supplementation for idiopathic hyperoxaluria in patients with nephrolithiasis was associated with a decreased Ox24 in 75% of patients. 4 Furthermore, a study of six healthy volunteers found that magnesium supplementation within 12 hours of an oxalate load decreased intestinal absorption of oxalate. 15 Similarly, another study of 24 healthy subjects found that magnesium supplementation at the time of oral oxalate load decreased oxalate absorption. 5 Indeed, a study of 16 recurrent stone formers found significantly lower urinary oxalate levels after 60 days of combined B6/magnesium supplementation, 16 and a study of 265 idiopathic calcium stone-forming patients reported that supplementation with B6 and magnesium reduced the recurrence rates of CaOx kidney stones. 17 Notably, none of these studies on B6 and magnesium were prospective controlled studies.
In this study, although not as efficacious as the D or DS groups, the supplement group did see a median decrease of 7.3 mg/day in Ox24, and approximately two-thirds of the patients in the supplement group realized a decrease in Ox24 (67.6%). Thus, B6/magnesium supplementation may help lower urinary oxalate, although not as efficaciously as a low oxalate diet. However, compliance with a low oxalate diet may be challenging and may conflict with other health-related dietary goals, as a low oxalate diet restricts many heart-healthy foods. Indeed, the D and DS groups had high rates of study noncompliance. Challenges with compliance are expected as dietary and lifestyle prevention regimens may result in noncompliance rates as high as 70%. 18 Accordingly, our study findings suggest that a sound strategy for reducing urinary oxalate in hyperoxaluric CaOx stone formers is to offer a low oxalate diet as a first-line treatment with magnesium/B6 supplementation as a second-line therapy for those with poor compliance with the low oxalate diet. Importantly, combination therapy was not superior to diet or supplementation alone for lowering urinary oxalate, and thus there is little clinical utility to combining the two treatment strategies.
In addition, it is important to note that the intestinal microbiome of stone formers adds to the complexity of analyzing urinary oxalate excretion. Oxalobacter formigenes, an oxalate degrading intestinal bacterium, has been shown to be a modulator of intestinal oxalate levels. 19,20 When compared with non-stone-forming control subjects, stone formers were found to have reduced or absent levels of O. formigenes, and higher urinary oxalate levels. 19,20 Furthermore, antibiotic use may reduce colonization of O. formigenes and other oxalate degrading bacteria in the gut, leading to increased stone formation. 21 In our study, three subjects were taking antibiotics during the study period in the setting of recurrent urinary tract infections (two in the supplement group and one in the combination group), which could influence the observed urinary oxalate levels in those patients.
Our study had several notable limitations. First, we conducted an “as-treated” analysis, as there was a high noncompletion rate, potentially adding a source of bias. In addition, we conducted a single 24-hour urine collection, rather than multiple 24-hour urine collections at each time point. Given that there is significant variability in 24-hour urine samples, this is a notable limitation of our study. Furthermore, our study lacked a true control group because of the ethical concerns associated with not treating a high-risk hyperoxaluric CaOx stone-forming patient. Finally, our findings may be underpowered, as power analysis determined that n > 45 was needed each group. However, because of noncompliance, only 35, 34, and 30 subjects in the D, S, and DS groups, respectively, completed the study and were included in the final analysis. Despite these limitations, we believe our study provides important data regarding the efficacy of a low oxalate diet and magnesium/B6 supplementation on the treatment of idiopathic hyperoxaluria. Ultimately, the most clinically relevant outcome for stone formers is recurrent stone episodes, and thus we recommend future long-term longitudinal studies to determine relationship between these prevention strategies and stone recurrence.
Conclusions
In the first prospective RCT comparing a low oxalate diet vs B6/magnesium supplementation vs a combination of both for the treatment of idiopathic hyperoxaluria in CaOX stone formers, we found that a low oxalate diet is most effective and should be considered for first-line therapy. However, approximately two-thirds of patients in the B6/magnesium supplementation group did experience a decrease in urinary oxalate, suggesting that B6/magnesium supplementation may be a good second-line therapy for those with poor compliance with low oxalate diet. Notably, combination therapy did not produce greater reductions in urinary oxalate than either of the monotherapy arms suggesting that combination therapy is of little clinical utility. Further study with long-term longitudinal follow-up is recommended to determine if these treatment strategies reduce recurrent stone events in idiopathic hyperoxaluric CaOx stone formers.
Footnotes
Author Disclosure Statement
Dr. Mantu Gupta is compensated for educational training for Cook Urological Inc., Boston Scientific Inc., Olympus Inc., Lumenis Inc., and Retrophin Inc. Additionally, Dr. Gupta is the Editor in Chief for Video Urology. No other authors have any relevant conflicts of interest to disclose.
Funding Information
There is no funding for this research study.