
Abstract
Purpose:
Although single-port robot-assisted radical prostatectomy (SP-RARP) is considered a safe and feasible approach for radical prostatectomy, the comparative performance of the SP robot with earlier models, including da Vinci Xi or Si, is elusive. This systematic review summarizes the current evidence on SP-RARP and compares its perioperative, functional, and oncologic outcomes to multiport robot-assisted radical prostatectomy (MP-RARP).
Methods:
We performed a systematic search in PubMed, Embase, Web of Science, and Cochrane Library database for randomized control trials (RCTs) and non-RCTs that compare SP-RARP to MP-RARP. The primary outcomes included perioperative, functional, oncologic, and painful outcomes. The odds ratio (OR) and weighted mean difference (WMD) were applied for the comparison of dichotomous and continuous variables with 95% confidence intervals (CIs).
Results:
Seven studies, including 1239 patients, were enrolled in the meta-analysis. We reported similar results for SP-RARP and MP-RARP in terms of the operative time, blood loss, continence and potency rates, complication rate, positive surgical margin, and biochemical recurrence. However, hospital stay (WMD −17.86 hours, 95% CI −27.80 to −7.92; p = 0.0004), catheterization time (WMD −1.51 days, 95% CI −2.60 to −0.41; p = 0.007), and the rate of opioid use (OR 0.26, 95% CI 0.13 to 0.53; p = 0.0002) were less with SP-RARP. In addition, more patients did not require any pain medication during the hospital stay with SP-RARP (OR 14.41, 95% CI 5.22 to 39.76; p < 0.00001).
Conclusions:
SP-RARP is associated with a shorter hospital stay and catheterization time, and the need for postoperative pain medication is lower compared to MP-RARP, with comparable perioperative, functional, and oncologic outcomes.
Introduction
Prostate cancer is the most prevalent cancer in men in the United States and the second highest cause of cancer-related deaths. 1 Radical prostatectomy is the most common management approach for clinically localized intermediate- and high-risk prostate cancer. 2 Because of the noticeable merits of postoperative recovery and better ergonomics provided by the robotic platform, the application of robot-assisted radical prostatectomy (RARP) in the surgical treatment of clinically localized prostate cancer is rising. 2,3 Currently, the multiport da Vinci platform is the most largely adopted robotic approach to radical prostatectomy. 4
Laparoendoscopic single-site surgery (LESS) was developed as an alternative to traditional laparoscopic surgery to minimize the morbidity of the surgical procedure and offer faster recovery and improved cosmetic results. 5 Previously, the LESS approach proved to be an effective conventional laparoscopic surgery without influencing surgical and postoperative results. Despite attempts using robotics, the clash between steep learning curves and continuous instrument clashes limits the adoption of the LESS method. 6,7 A dedicated single-port (SP) robotic platform for the da Vinci surgical system was recently developed by Intuitive Surgical. The single-port da Vinci SP robot improves robotic access to the abdominal cavity, and it lets to a resurgence of LESS because of its innovativeness. The da Vinci SP system has some novel functions in the facilitation of single-site surgery, aided by its single multichannel laparoscopic trocar, improved guidance, and articulating camera. Of note, the SP system potentially offers better ease of use, cosmesis, and improved convalescence. Several SP-RARP technology-based case series through different surgical approaches have since been shown to be feasible and safe. 8 –10 A recent systematic review and single-arm analysis of SP-RARP 11 could not clarify the difference between SP-RARP and multiport (MP)-RARP in terms of perioperative, functional, and oncologic outcomes; this warrants further exploration.
In this systematic review, we summarize the current evidence on SP-RARP and compare its reported results to those of the MP-RARP technique.
Methods
This systematic review and meta-analysis were conducted as per the PRISMA statement. 12
Literature search strategy, study selection, and data collection
We conducted a systematic electronic literature search in February 2021 in PubMed, Embase, Web of Science, and Cochrane Library database. Intervention and patient-related search terms were combined to build the following search string: ((Prostatectomy OR Prostatic Neoplasms) AND (Robotic Surgical Procedures OR Robotics OR Robot-assisted) AND (single-port OR multiport)). The search was limited to English.
Inclusion criteria were defined using the PICOS approach. P (patients): All the patients were found to have prostate cancer; I (intervention): undergoing SP-RARP; C (comparator): MP-RARP was performed as a comparator; O (outcome): one or more of the following outcomes: perioperative outcomes, functional outcomes, oncologic outcomes; S (study type): prospective comparative, retrospective studies or randomized control trials. Exclusion criteria: (1) noncomparative studies; (2) editorial comments, meeting abstracts, case reports, book chapters, or studies reporting experimental; (3) none of the defined outcome measure analysis.
Two reviewers individually extracted data from the included studies. Data extracted for individual study included: (1) general information related to the article: first author, country, year of publication; (2) population characteristics: sample size, age, prostate-specific antigen (PSA), body mass index (BMI), prostate volume, pathologic grade group; (3) perioperative outcomes: operative time, blood loss, hospital stay, catheterization time, perioperative pain; (4) overall complications (defined as Clavien grade ≥1), major complications (defined as Clavien grade ≥3) 13 ; (5) functional outcomes: continence recovery (defined as the use of 0–1 pad/day), potency recovery (defined as the ability to achieve and maintain erections sufficient for sexual intercourse without PDE5 inhibitors, intracavernous injections, and intraurethral alprostadil use); and (6) oncologic outcomes: Positive surgical margins (PSMs), biochemical recurrence (BCR). Any dispute was resolved by consensus or consultation with a third reviewer.
Assessment of risk of bias
Among the studies, ROBINS-I was applied to determine 14 bias due to (1) confounding, (2) selection of participants, (3) classification of exposures, (4) departures from intended exposures, (5) missing data, (6) measurement of outcomes, and (7) selection of the reported result.
Statistical analysis
Meta-analyses were performed using odds ratios (ORs) for dichotomous outcomes, while weighted mean differences (WMDs) were used for continuous outcomes. The results were reported with 95% confidence intervals (CIs). Meta-analyses of dichotomous variables were pooled using the Mantel–Haenszel method, and continuous variables were performed using the inverse variance method. Taking account of predictable substantial between-trial heterogeneity, a random-effects model was used to combine all summary data. Review Manager V5.4 software (Cochrane Collaboration, Oxford, United Kingdom) was used for result synthesis. Heterogeneity across the included studies was assessed using the I 2 statistic. 15 p-Values of <0.05 were regarded as statistically significant. Data that could not be measured by meta-analysis were presented narratively.
Subgroup analysis
We performed a subgroup analysis based on the different surgical approaches for SP: transperitoneal, extraperitoneal, and perineal approach.
Sensitivity analysis
We performed sensitivity analyses to assess the robustness of the estimates according to the size of the study cohort (excluding studies with <150 patients) and applied the leave-one-out method to exclude studies one at a time from the pooled effect. However, sensitivity analyses were not performed when comparing three or fewer studies.
Publication bias
Because the test power was lacking when 10 or fewer studies were included, we could not evaluate the publication bias. 16,17
Results
Study characteristics
After preliminary screening and full-text review, we included 1239 patients in 7 studies for meta-analysis (Fig. 1). 18 –24 All the multiport platforms are da Vinci Si or Xi systems. SP-RARP was used as single-port da Vinci SP robotic platform. Table 1 summarizes the number and baseline demographics of the included patients having each intervention and their associated preoperative variables (age, BMI, PSA, prostate volume, International Society of Urological Pathology [ISUP] grade group, and pathologic stage). The baseline characteristics of the prostate volume were not relatively equal in one study (the mean volume for the SP-RARP group and the MP-RARP group was 30 and 48 mL, respectively). 24 However, the preoperative demographics were comparable in other studies, with similar age, BMI, baseline PSA, prostate volume, ISUP grade group, and pathologic stage observed in each of the included studies. The median follow-up time of the studies ranged between 3 and 13 months.

PRISMA flow diagram for the systematic review.
Main Baseline Patient for the Studies Included
Mean (SD).
ASA = American Society of Anesthesiologists classification; AUASS = American Urological Association symptom score; BMI = body mass index; ISUP = International Society of Urological Pathology; MP = multiport; PSA = prostate-specific antigen; SD = standard deviation; SP = single-port.
Perioperative outcomes are summarized in Table 2. The transperitoneal approach was adopted for MP-RARP. Six studies used SP-RARP through the transperitoneal or extraperitoneal approach. 18 –23 In four studies, patients underwent SP-RARP performed with the SP console by one surgeon. 18,20,23,24 Besides, the patients in the other two studies underwent SP-RARP performed by two and three experienced robotic surgeons using the SP console, respectively. 21,22 Patients enrolled in one of the studies treated with the SP platform; patients underwent perineal radical prostatectomy. 24 Notably, most patients that managed with the perineal approach underwent complex abdominal surgery. Furthermore, we often encountered the complex anatomy and narrow and deep surgical field with perineal radical prostatectomy. To avoid the huge heterogeneity and bias, the operative time, blood loss, and complications during perineal radical prostatectomy were excluded in the analysis. Functional oncologic outcomes and complications are summarized in Table 3.
Perioperative Outcomes
Mean (SD).
Complication and Functional and Oncologic Outcomes
Mean (SD).
Assessment of quality
No prospective studies on SP-RARP vs MP-RARP were available, except for retrospective comparative studies. Because all the studies conducted retrospective comparative analysis and published between 2020 and 2021, the level of evidence was intermediate. Overall, the risk of bias was considered moderate in seven studies (Table 4; the details are in the Supplementary Data).
The Risk of Bias (Nonrandomized Control Trials)-ROBINS-I
Outcome analysis
Perioperative outcomes and complications
Meta-analysis of operative time revealed no significant difference between SP-RARP and MP-RARP (six studies pooled; p = 0.38). 18 –23 Similarly, there is no statistical significance in the blood loss between SP-RARP and MP-RARP (four studies; p = 0.32). 19 –22 When we pooled the results from three studies, the SP-RARP group demonstrated less catheterization time compared to MP-RARP (WMD −1.51 days, 95% CI −2.60 to −0.41; p = 0.007). 20,22,24 Furthermore, there was no statistical significance in the hospital stay which had taken “days” as the unit between SP-RARP and MP-RARP (three studies; p = 0.17). 19,21,22 However, the pooled estimates of hospital stay which had taken “hour” as the unit were less in SP-RARP compared to MP-RARP (three studies; WMD −17.86 hours, 95% CI −27.80 to −7.92; p = 0.0004). 20,23,24 After we eliminated studies with <150 patients and performed the leave-one-out test, the statistical significance did not change in terms of operative time and blood loss (Fig. 2).
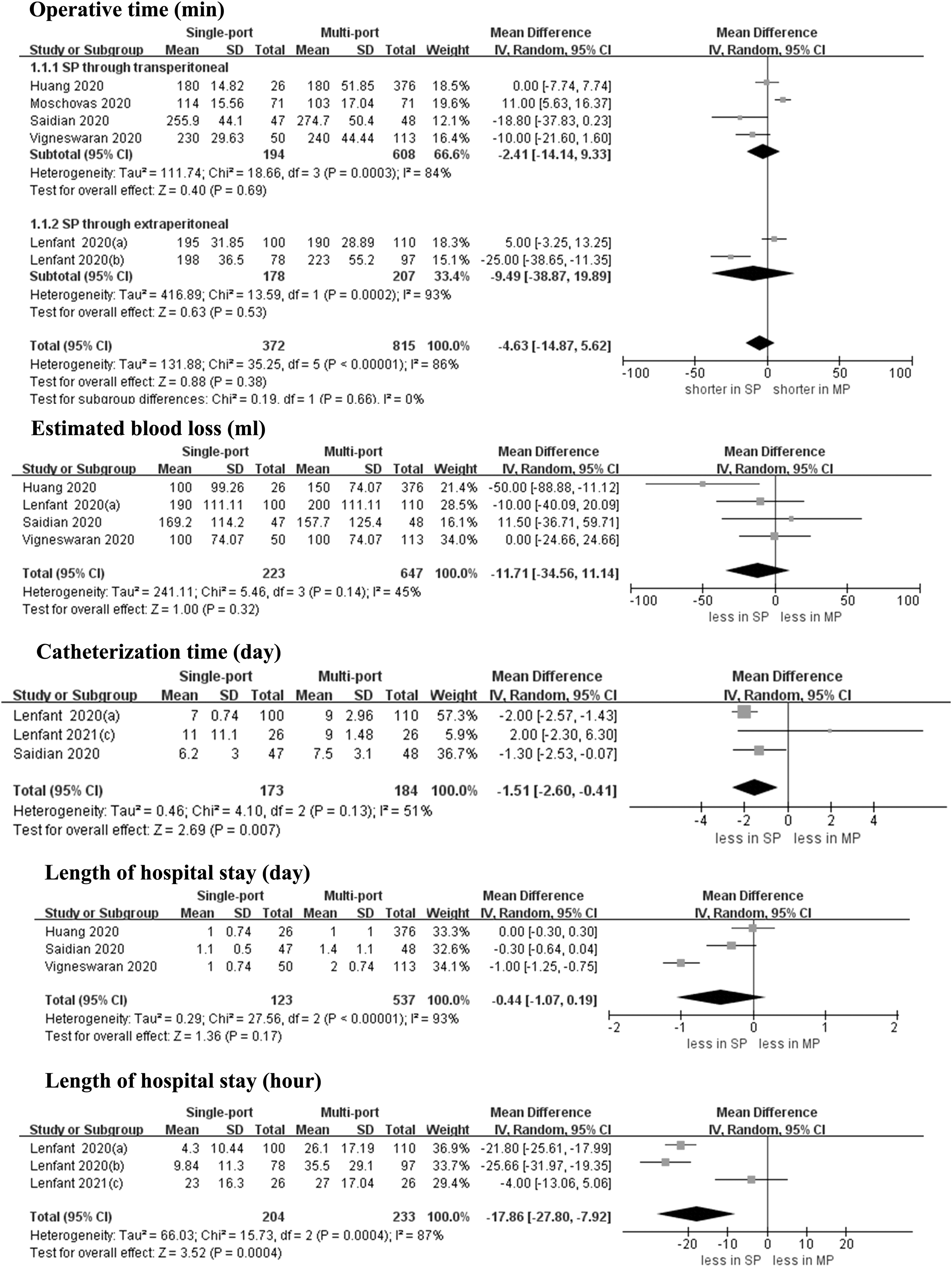
Forest plots of perioperative outcomes for SP-RARP vs MP-RARP (operative time, blood loss, catheterization time, and hospital stay). CI = confidence interval; DF = degrees of freedom; IV = inverse variance; MP-RARP = multiport robot-assisted radical prostatectomy; SD = standard deviation; SP-RARP = single-port robot-assisted radical prostatectomy.
The overall complication rates were 10.2% (20 out of 197 cases) for SP-RARP and 13.5% (75 of 557 cases) for MP-RARP, respectively. 18,20,21 Meta-analysis of overall complication rates showed no significant difference between SP-RARP and MP-RARP (three studies; p = 0.38). Similarly, there is also no statistical significance in the major complication and Clavien grade ≥2 between SP-RARP and MP-RARP (two studies; p = 0.83 and three studies; p = 0.32). Pooled analysis for four studies showed the MP-RARP group had less readmission rate compared with SP-RARP (OR 2.80, 95% CI 1.19 to 6.59; p = 0.02) (Fig. 3). 18,20,23,24
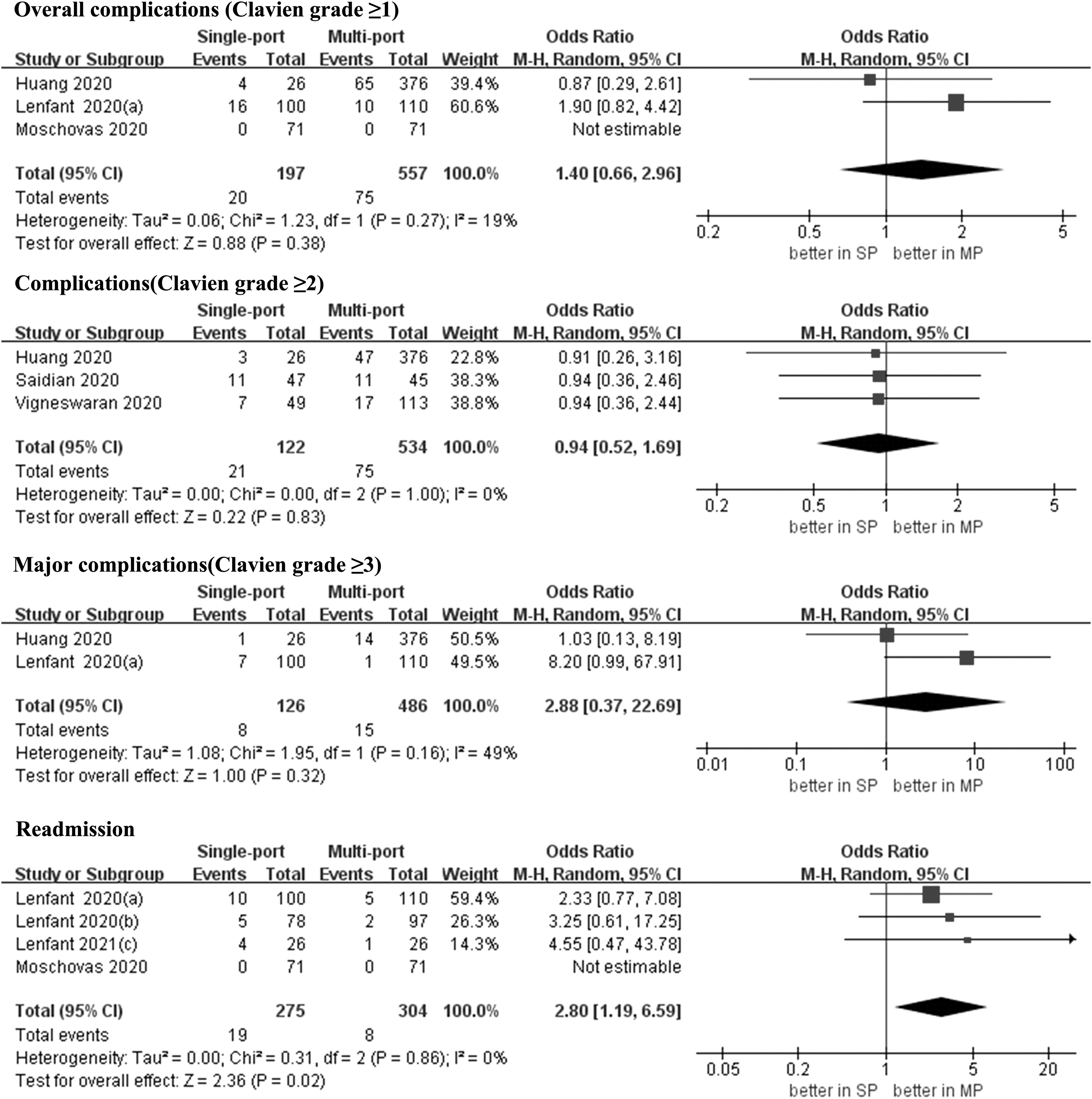
Forest plots of complication and readmission for SP-RARP vs MP-RARP (overall complications, major complications, and readmission rate).
Perioperative pain
The cumulative analysis showed no significant difference between SP-RARP and MP-RARP in terms of pain score ≤3 (two studies; p = 0.42). 20,24 However, with SP-RARP, more patients did not use pain medication during hospital and before discharge (OR 14.41, 95% CI 5.22 to 39.76; p < 0.00001 and OR 5.10, 95% CI 1.81 to 14.37; p = 0.002). Similarly, the number of patients who used opioid was less for the SP-RARP group during hospital and before discharge (OR 0.26, 95% CI 0.13 to 0.53; p = 0.0002 and OR 0.08, 95% CI 0.04 to 0.15; p < 0.00001). 20,24 In one study, fewer patients were pain free on postoperative day 1 in the SP-RARP group (p < 0.05). 19 However, a study found no significant differences in pain score at 6, 12, and 18 hours (p < 0.05). 18 Similarly, in one study, no significant differences were found in maximum patient-reported pain at 6 and 24 hours before discharge (p < 0.05) (Fig. 4). 21

Forest plots of perioperative pain for SP-RARP vs MP-RARP (pain score and pain medication).
Functional outcomes
The absolute risk of urinary continence was 69.8% (171 of 245 cases) and 70.1% (224 of 317 cases) at 12 weeks after SP-RARP and MP-RARP, respectively. And the meta-analysis showed no significant difference between two robotic platforms (five studies; p = 0.52). 18 –20,22,24 The leave-one-out sensitivity analysis and excluding smaller studies also showed no significant differences between SP-RARP and MP-RARP at 12 weeks. Similarly, there is also no statistical significance in the urinary continence at 24 and 48 weeks (p = 0.33; p = 0.33). 20,24 In terms of potency recovery, there is also no statistical significance between SP-RARP and MP-RARP (p = 0.25) (Fig. 5). 18,22
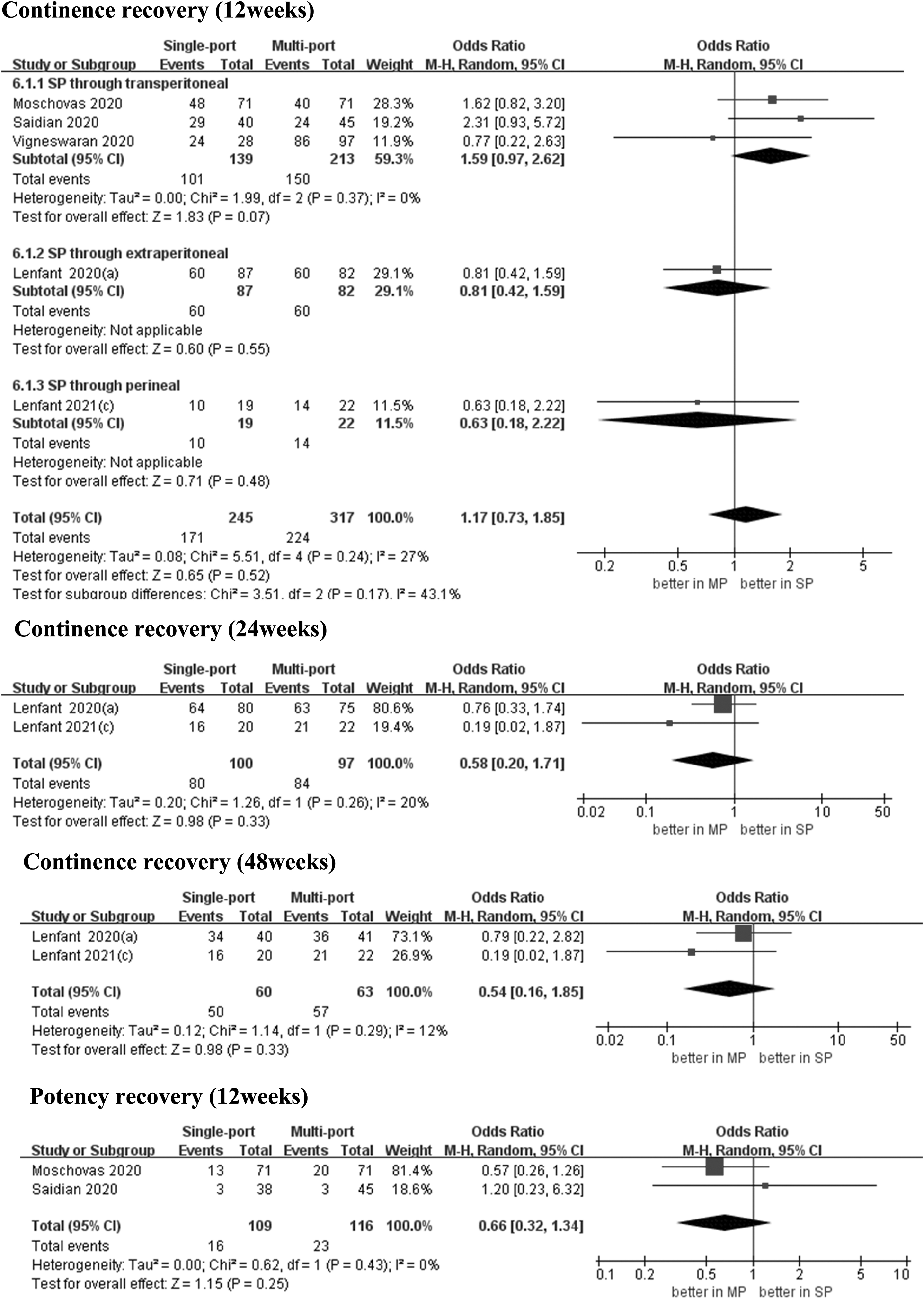
Forest plots of functional outcomes for SP-RARP vs MP-RARP (continence recovery and potency recovery).
Oncologic outcomes
The overall PSM rates were 27.4% (109 out of 398 cases) for SP-RARP and 29.5% (248 of 841 cases) for MP-RARP. The meta-analysis showed no statistically significant difference between two robotic platforms in overall PSM rates (seven studies; p = 0.72). 18 –24 Following the analysis of PSM rates in <PT3 and ≥PT3 tumors, two studies reported no significant differences between SP-RARP and MP-RARP (p = 0.40; 0.36). 18,22 In terms of BCR, two studies used PSA >0.1 ng/mL as BCR, one study applied PSA >0.2, and the other study applied PSA >0.03. When detecting BCR, the time point of two studies was 12 months, 20,24 whereas that for other studies 18,22 was 4 months. Four studies reported no significant differences between SP-RARP and MP-RARP (p = 0.48). When we eliminated studies with <150 patients and performed the leave-one-out test, no statistically significant change in the difference between PSMs and BCR was reported (Fig. 6). 18,20,22,24

Forest plots of oncologic outcomes for SP-RARP vs MP-RARP (positive surgical margins and biochemical recurrence).
Heterogeneity
Most of the outcomes exhibited moderate to high heterogeneity. Low heterogeneity was found for perioperative pain, overall complications, major complications, and functional outcomes. However, it may be misleading to assume that the heterogeneity of these results was low because the I 2 has a substantial bias when the number of studies is small. 25
Discussion
This is the first systematic review and meta-analysis that compares the outcomes of SP-RARP to MP-RARP. Some important findings in this analysis warrant in-depth discussion.
Perioperative outcomes
We compared the perioperative, functional, and oncologic outcomes of 398 patients who underwent SP-RARP. Operative time, blood loss, hospital stay, catheterization time, perioperative pain, and complication were the main perioperative parameters of SP-RARP and MP-RARP. Notably, no significant difference was reported between SP-RARP and MP-RARP in operative time. The da Vinci SP surgical system is a novel robot platform; however, the technical steps are for the most part similar to those of MP-RARP, an implication that the transition from multiport to SP may be simple and fast. In addition, we thought that with the increase in the number of operations and experience of each surgeon using the SP platform, the operation time would be shorter.
In terms of hospital stay, no statistical significance was found when the unit was “day”; however, it was significantly shorter for SP-RARP compared to MP-RARP when outcomes were taken using “hour” as the unit. There is no doubt that SP-RARP will not increase the length of stay. In the United States, patients are usually discharged <2 days post-MP-RARP. 26 –28 Adopting a single access port could potentially reduce the invasiveness of the surgery, which consequently reduces the hospital stay and perioperative pain. One study also reported that the same-day discharge SP-RARP was feasible. 29 We noted that studies which used “hour” as the unit for the same-day discharge (discharged <1 day) were more precise. Similarly, in the SP-RARP group, catheterization time was less compared to the MP-RARP group. Most patients undergoing SP-RARP or MP-RARP experience 5 to 7 days catheterization time postoperatively, which is similar to many institutions. 30 Herein, a shorter catheterization time was associated with reduced invasiveness. Although some studies have reported that the early removal of the catheter after RARP does not increase perioperative complications, they failed to establish the optimal duration for catheterization. 31,32 The insufficient literature and larger sample in one study may have caused heterogeneity. As such, more high-level evidence is needed to prove our findings.
Complications
The overall complication rates of SP-RARP and MP-RARP were 10.2% and 13.5%, respectively. The difference in complication rates between the two approaches was not statistically significant. In contrast, the recently published series reported similar results that the incidence of minor complications was 13.3% with RARP. 33 In terms of a major complication, two cases of urinary leakage were recorded in the SP-RARP group.
Perioperative pain
Herein, we reduced the administration of painkillers and opioids during and after hospitalization. Recently, numerous reports have been published on persistent opioid use after surgery and dependence caused by abuse of prescription medications. 34 Therefore, the reduction of opioid intake after surgery is a health concern in clinical practice. In addition, opioids are often associated with inherent side effects, including vomiting and nausea, which may increase postoperative morbidity. 35 We found that reduced invasiveness was associated with a low intake of painkillers and opioids during and after hospitalization. However, such analyses are scanty in literature and were reported from the same institution. More studies from different institutions would be vital to further verify this conclusion.
Functional outcomes
The goal of modern prostate cancer surgery is to maximize oncologic efficacy while minimizing its impact on the patient's quality of life and body functions. 36 The continence recovery was defined as use of 0 to 1 pad per day but found no significant difference for continence between SP-RARP and MP-RARP at 12, 24, and 48 weeks. Similarly, there was no statistical significance in potency recovery at 12 weeks. However, some key issues cannot be ignored when comparing the functional results of SP-RARP with MP-RARP. First, due to the absence of a standard definition for continence and potency, different outcomes can be drawn when using different definitions. In the future, standard definitions (pad diary, ICIQ-SF, and EORTC-PR25) should be applied for continence evaluation to ensure that the conclusions drawn by the study are of clinical importance. 37 Second, surgical experience plays a major role in the functional and oncologic outcomes of RARP. 38,39 Therefore, the individual performance of surgeons may impact the comparison of trials with different surgical techniques. Third, wide excision surgery, nerve-sparing technique, puboprostatic-sparing techniques, and pelvic lymphadenectomy have a potential impact on the recovery of continence and potency. 40 Therefore, we have to be cautious when evaluating the functional outcome after SP-RARP and MP-RARP.
Oncologic outcomes
Our meta-analysis likely confirms oncologic safety. The overall PSM rates were 27.4% for SP-RARP and 29.5% for MP-RARP, respectively. Similarly, a tertiary referral center in the United Kingdom reported an overall PSM rate of 30.6%. 41 Nevertheless, some key issues should be emphasized when comparing the PSM results of SP-RARP with MP-RARP. First, tumor stage, PSA level, and prostate volume are among the relevant factors for predicting the incidence of PSMs. 42,43 In this meta-analysis, following the analysis of PSM rates in <PT3 and ≥PT3 tumors, SP-RARP and MP-RARP exhibited no significant difference. Second, a recent study reported a large and statistically significant variation among individual surgeons regarding oncologic outcomes. 44 As such, the variation between surgeons must be considered when undertaking a comparative analysis between surgical techniques. We think that with more experience in the new SP platform-related procedures, surgeons can achieve best oncology results currently reported in the literature. 45 In terms of BCR, four studies reported no significant differences between SP-RARP and MP-RARP. However, tumor stage and follow-up time were crucial factors in the prediction of the incidence of BCR. Of note, we did not include a study that compared BCR in tumor stages, and the follow-up time of the two studies was relatively short (the mean duration was 4 months). 18,22 Furthermore, the BCR was defined by different PSA values; therefore, we could not arrive at a concrete conclusion. In the future, we would require more studies on different tumor stages and long-term follow-up to verify this conclusion.
SP-RARP is a new technology, yet some important aspects are worth in-depth discussion. First, the advent of the SP robotic platform has prompted the rediscovery of different access routes to the prostate. 46 Notably, the different surgical approaches might represent a major source of bias in our analysis. Although we performed a subgroup analysis based on the different surgical approaches for the SP platform, we did not find any statistical difference within the subgroup in some outcomes. However, subgroup analysis was not performed for all results as the data were lacking. A recent study evaluated SP-RARP and found that the postoperative hospital stay was significantly shorter shortened with extraperitoneal approaches compared to transperitoneal approaches. 47 In contrast, patients with a history of complicated abdominal surgery may be disqualified for surgical treatment because of the high risk of intraoperative or postoperative complications and the high risk of side effects of radiation on scar tissue or adjacent intestinal adhesions. These patients may also be declared unsuitable for radiotherapy or brachytherapy. 48 –50 The SP platform could avoid the bulkiness related to the volume of the robotic arms that led to external clashing, not limiting certain movements and bedside assistance compared with the MP platform. There are recent reports on the safety and feasibility of the perineal approach using the SP console for highly selected patients declared unfit for abdominal surgery or radiotherapy. 8,24,51 In the present study, the average BMI and prostate volume of the patients enrolled were quite low (mean BMI <32 kg/m2; mean prostate volume <53 mL). Whether the SP approach could provide similar outcomes to MP-RARP for patients with obesity and large volume prostate remains elusive. More studies are warranted to compare SP-RARP to MP-RARP and assess the actual benefits of using different operation methods and platform.
Second, because the results reported with regard to the use of the SP robotic platform are derived from the experience of using a multiport system before SP, the impact of learning the curve on this study should be explored further. The readmission rate was higher in the SP group, which appears to be clinically relevant. The higher readmission rate could be explained by the learning curve for SP manipulation. A study reported that 70% of readmission occurred in the first half of patients. 20 As experience matured, the number of readmissions decreased. In addition, operative time could be adopted as a measure of the learning curve. However, there is no statistical significance in the operative time between two robotic platforms, implying that the learning curve of SP-RARP is short for a surgeon experienced in MP-RARP. One study reported that the SP approach was likely associated with a longer console time. Furthermore, constant use of the relocation pedal would increase the console time because the process takes a few seconds until the platform slowly targets the robot toward a different surgical site and place the gel point. This study recommends that we could use an auxiliary assistant port (single port plus one) to minimize the impact of our learning curve and decrease the operative time. 18 In the future, we can make some better improvements such as iterative improvements may be by coming to improve suction or retract to overcome the necessity for an assistant and enable true SP procedure. 52
Third, the potential shortcomings of the SP robot platform include novel instruments and cost considerations, which exist in all robotic surgical approaches. 53 Therefore, the da Vinci SP as a dedicated surgical platform for radical prostatectomy must be assessed financially. One study reported higher costs for SP compared with conventional MP-RARP in surgical materials. However, because the higher SP cost of surgical consumables is offset by the lower cost of fewer hospitalizations, the costs for SP-RARP and MP-RARP prostatectomy are comparable. 23 We believe that SP robotic may follow the same trend seen for several past examples of new technologies in terms of cost, which has declined over time.
The present study has some limitations which need to be mentioned for the interpretation of the results. First, the da Vinci SP surgical system is a novel robot platform, the SP-RARP was performed by experienced robotic surgeons in the included studies, and the results were retrieved from a high-volume referral center with extensive expertise in urologic oncology (three studies were from the same institution). So, the conclusions of this meta-analysis may be unsuitable for less experienced centers. Second, the included studies are retrospective with intermediate quality; they may have been affected by selection bias and unmeasurable confounding factors. Third, because of the absence of data in each study, most of our comparisons rely on data from some of the seven included studies. Fourth, the short follow-up and the absence of standard definition limit the comparison between the platforms in terms of functional or oncologic outcomes. Finally, because of the insufficient number of studies included, we could not assess publication bias.
Conclusions
The findings of this meta-analysis are encouraging for SP-RARP. Particularly, the SP platform was associated with a shorter hospital day and a decreased need for postoperative pain medication. It also provides similar perioperative, functional, and oncologic outcomes compared to the MP platform. Because the included studies were of intermediate quality and retrospective, higher level evidence and prospective randomized trials are warranted to prove the superiority of SP and reveal the patients most likely to benefit from the SP.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This work was supported by City of Nanchong Strategic Cooperation with Local Universities Foundation of technology (NSMC20170421, NSMC20170111, 18SXHZ0581, 18SXHZ0128). This work was supported by Application and Basic Research Program of Sichuan Science and Technology Department (2020YJ0185).
Supplementary Material
Supplementary Data
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.