
Abstract
Objective:
To assess the fiber–tissue interaction through ablation, coagulation, and carbonization characteristics of the Ho:YAG laser and super pulsed thulium fiber laser (TFL) in a nonperfused porcine kidney model. To assess the degradation of laser fibers during soft tissue treatment.
Methods:
A 50 W TFL generator was compared with a 120 W Ho:YAG laser. The laser settings that can be set identically between the two lasers (pulse energy and frequency), and clinically relevant for prostate laser enucleation, were identified and used for tissue incisions on fresh nonfrozen porcine kidneys. For each parameter, the short, medium, and long pulse durations for the Ho:YAG generator and the different peak powers 150, 250, and 500 W for the TFL generator were also tested. Laser incisions were performed with 550 μm stripped laser fiber fixed on a robotic arm at a distance of 0.1 mm with the tissue surface and at a constant speed of 10 mm/s. Histologic analysis was then performed, evaluating incision shape, incision depth and width, axial coagulation depth, and presence of carbonization. Degradation of the laser fiber was defined as reduction of laser fiber tip length after laser activation.
Results:
Incision depths and areas of coagulation were greater with the Ho:YAG laser than those with the TFL. Although no carbonization zone was found with the Ho:YAG laser, this was constant with the TFL. Although a fiber tip degradation was constantly observed with Ho:YAG laser, except in the case of a long pulse duration and low pulse energy (0.2 J), this was not the case with TFL.
Conclusion:
TFL appears to be an efficient alternative to Ho:YAG laser for soft tissue surgery. The histologic analysis found greater tissue penetration with the Ho:YAG laser and different coagulation properties between the two lasers. These results need to be investigated in vivo to assess the clinical impact of these differences and find the optimal settings for laser prostate enucleation.
Introduction
Lasers are currently an integral part of the armamentarium in endourology, and may be used for lithotripsy as well as soft tissue applications such as vaporization and enucleation of prostate, treatment of urothelial tumors, endopyelotomy, and incision of ureteral strictures. 1 –3 Since its introduction in the 1990s, Ho:YAG laser, emitting at a wavelength of 2120 nm, became the reference of lasers in urology because of its versatility and efficiency. 3,4 However, a new player has been recently introduced: the super pulsed thulium fiber laser (TFL), with potential advantages over Ho:YAG laser such as higher water absorption peak because emitting at a wavelength of 1940 nm, a longer pulse duration that should provide better cutting or coagulation properties, and a better wall-plug efficiency. 1,2,5 –12 Currently, laser technologies play a prominent role in modern endoscopic management of soft tissues treatment such as primary benign prostatic hyperplasia. Because evidence of TFL's tissue ablation and coagulation capabilities is limited, we aimed to assess in an ex vivo model the fiber–tissue interaction through ablation, coagulation, and carbonization characteristics of the Ho:YAG laser and TFL to clarify the different effects during laser enucleation of prostate. 13 –15 As secondary objective, we aimed to assess the degradation of laser fibers during soft tissue treatment.
Methods
Model
Fresh nonfrozen porcine kidneys were used as ex vivo study model to investigate laser–tissue interaction. Although various tissue models were used in the literature to investigate the effects of laser on histologic parameters, porcine kidneys were the most reported. 16 –22 Furthermore, this model has the advantage of a comparable specific absorption coefficient to prostate. 10,23 –26 Kidneys were cut into 4 × 3 cm pieces (Fig. 1). Only pieces with flat surfaces were selected. Then, they were placed and fixed in a metal box.
Incisions on a porcine kidney sample. Color images are available online.
Laser systems
A 50 W super pulsed TFL generator (IPG Photonics, Russia) with a wavelength of 1940 nm was compared with a 120 W Ho:YAG laser (P 120H; Lumenis, Israel) with a wavelength of 2120 nm. The Ho:YAG laser was used in a regular mode ( = non-Moses setting). The laser settings that can be set identically between the two lasers (pulse energy and frequency), and those considered clinically relevant for prostate laser enucleation (1 J × 30 Hz, 1 J × 50 Hz, 1.5 J × 30 Hz, 2 J × 25 Hz), were identified and used for tissue incisions (Table 1). Some additional parameters, only settable with the TFL, were evaluated: 0.1 J × 60 Hz, 0.1 J × 250 Hz, and 0.2 J × 250 Hz. A third parameter can be set on these two laser generators: the pulse duration for the Ho:YAG laser and the peak power for the TFL. For each laser setting (pulse energy and frequency), the short, medium, and long pulse durations for the Ho:YAG generator and the different peak powers 150, 250, and 500 W for the TFL were also tested. Stripped surgical laser fibers of a single manufacturer with core diameters of 550 μm were used for both laser systems (SlimLine SIS Endo, Lumenis, Israel) to avoid any confusion because of a variability in laser fiber characteristics. Before each test, laser fibers were cut with ceramic scissors and stripped.
Common Laser Settings to Ho:YAG Laser and Super Pulsed Thulium Fiber Laser Used for Tissue Incisions
Experimental setup
We performed laser incisions on fully immerged porcine kidney samples in saline with an automated robotic arm employed to hold the firing laser fiber at a fixed distance from tissue samples, and to maintain the cutting speed constant (KR6R900; Kuka International, Germany). The distance between the tissue surface and the laser fiber tip was set to 0.1 mm with a micrometer screw, and cutting speed was set at 10 mm/s. For each laser generator, four incisions per laser setting were performed on a kidney sample (Fig. 1). Degradation of laser fibers was also evaluated. The degradation was defined as reduction of laser fiber tip length and evaluated by photography before and after laser activation for each test.
Histologic analysis
Once incisions were made, histologic analysis was performed. Each sample was then preserved in a 4% formaldehyde solution. The following steps consisted of inclusion of the samples in paraffin blocks. Then, 3 μm slices were made using a microtome and stained with hematoxylin phloxine saffron. Each slice included the four incisions. One slice per sample was examined. Microscopic examination was then carried out using a Leica DM 2500 microscope equipped with the Leica digital camera and the LAS Core V4.8 software (Leica Microsystems, Switzerland). A senior pathologist (E.C.) and a urologist (S.D.) performed the histologic laser incision analysis. During laser incision, a temperature gradient will form inside the tissue. In the zone where the temperature exceeds 300°C, the tissue will vaporize ( = cutting or incision area). This will be followed by a zone with a temperature exceeding 150°C where the tissue will be carbonized; the next tissue layer will be coagulated (Fig. 2). 10 Thus, the following data were collected: incision depth and width (mm), the tissue carbonization level, and the axial coagulation depth (mm) (Fig. 3A). The carbonization grade was evaluated with a visual grading scale, from 0 (no carbonization) to 3 (extensive carbonization) (Fig. 3B).
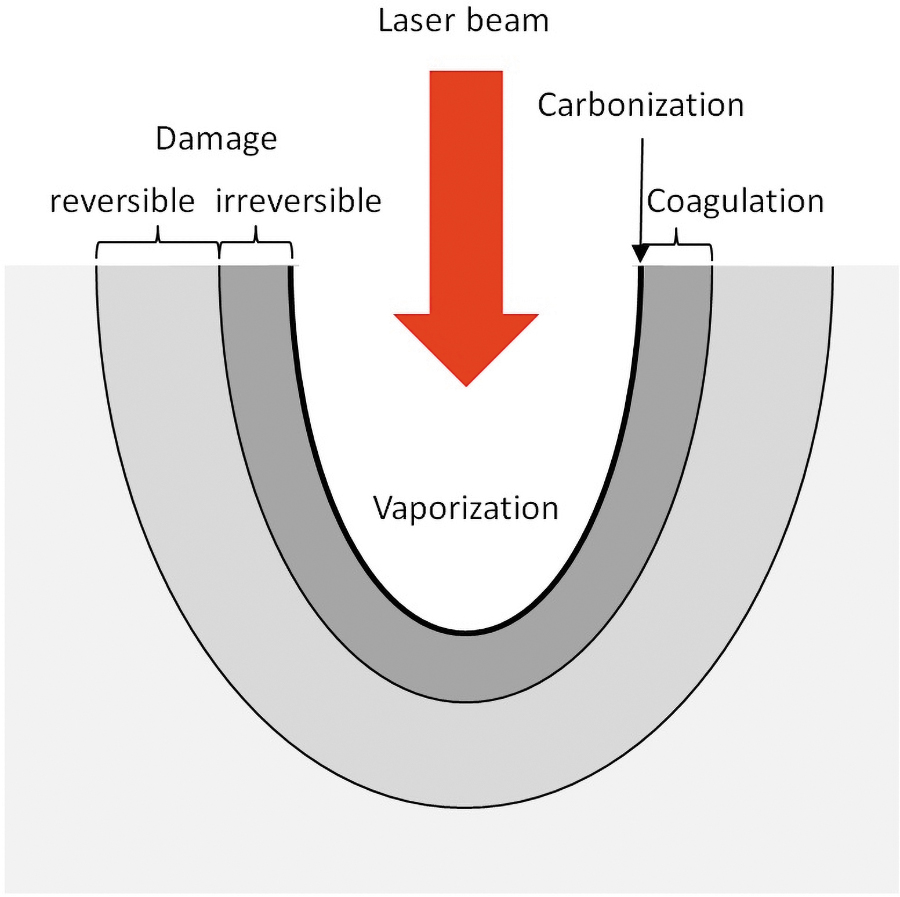
The various action zones during the cutting of tissues. 10 Color images are available online.

Primary outcomes.
Statistical analyses
Results are presented as median with standard deviation. The Mann–Whitney test was used for comparisons between groups. All tests were conducted using the R Software, version 4.0.3. A p-value of 0.05 or less was considered significant.
Results
Ho:YAG laser
Regardless of the laser setting, the shapes of incisions were wider than deeper, with laceration and irregular limits (Fig. 4). The deepest incision was obtained with the following parameters: 2 J × 25 Hz, medium pulse duration. The largest width was obtained with the following parameters: 1 J × 50 Hz, medium pulse duration. The most extensive coagulation zone was obtained with the following parameter: 1.5 J × 30 Hz, long pulse duration. At a fixed pulse energy and frequency, pulse duration change had no effect on incision width, p > 0.05. This was also the case for incision depth, except at 1 J × 30 Hz wherein a short pulse duration was associated with a significantly lesser depth than a medium or long pulse duration. Regarding the coagulation zone, there was no effect of pulse duration, p > 0.05. At a fixed pulse energy and pulse duration, frequency change had no effect on incision width and depth, as well as coagulation zone, p > 0.05. At a fixed frequency and pulse duration, pulse energy change had no effect on incision width and depth, as well as coagulation zone, p > 0.05. No laser fiber tip degradation was observed for the following parameters: 0.2 J × 60 Hz, regardless of pulse duration. For the other parameters, a fiber tip degradation was constantly observed, except in the case of a long pulse duration.
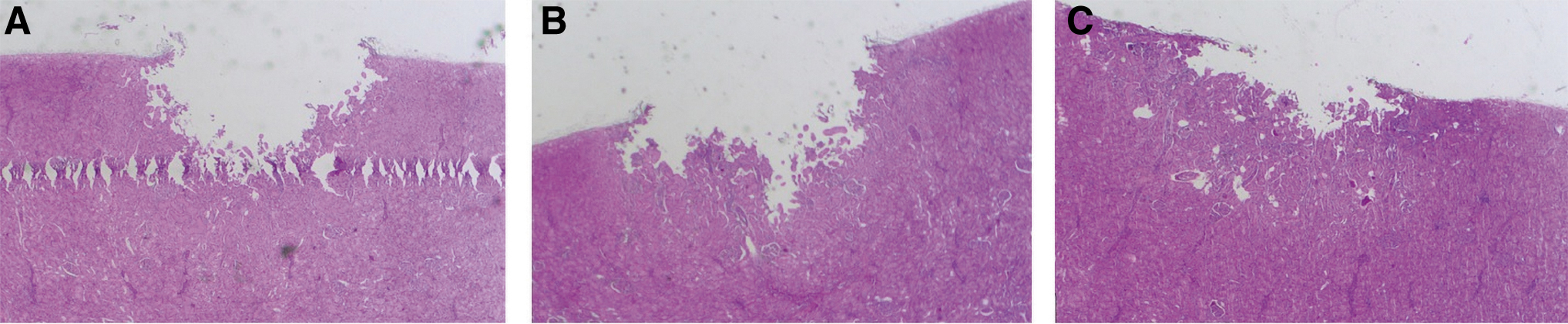
Incisions with Ho:YAG laser.
Thulium fiber laser
Incision shapes were variable, depending on the laser parameters, but the limits were constantly regular (Fig. 5). The deepest incision was obtained with the following parameters: 1.5 J × 30 Hz, 500 W peak power. The largest width was obtained with the following parameters: 1 J × 50 Hz, 500 W peak power. The most extensive coagulation zone was obtained with the following parameters: 2 J × 25 Hz, 125 W peak power. At a fixed pulse energy and frequency, peak power change had no effect on incision width and depth, as well as coagulation zone, p > 0.05. At a fixed laser pulse energy and peak power, frequency change had no effect on incision width and depth, as well as coagulation zone, p > 0.05. At a fixed frequency and peak power, pulse energy change had no effect on incision width and depth, as well as coagulation zone, p > 0.05. There was no fiber tip degradation for all the tests.
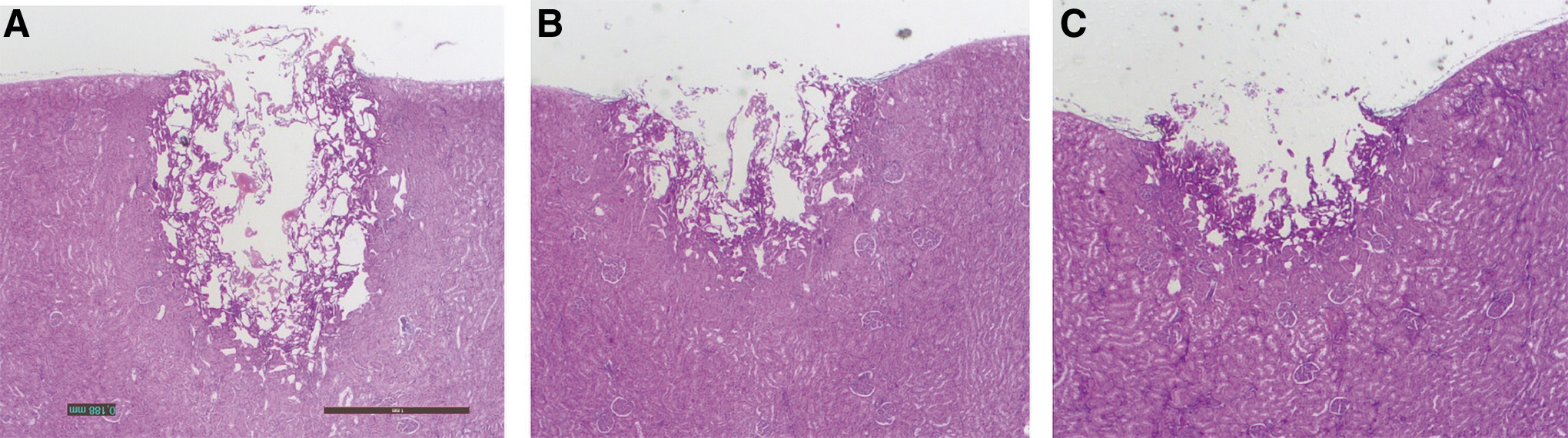
Incisions with TFL.
Comparison of Ho:YAG laser and TFL
At a fixed energy and frequency, there was no significant difference between the two lasers regarding the incision widths, except at 1 J × 30 Hz and 1.5 J × 30 Hz. Incision depths and areas of coagulation were statistically greater with the Ho:YAG laser than with the TFL. Regarding the incision depths, there was no significant difference in the following cases: 0.2 J × 60 Hz, 1 J × 50 Hz. Regarding the coagulation zones, no significant difference was found in the following cases: 1 J × 50 Hz, 2 J × 25 Hz. No carbonization zone was found with the Ho:YAG laser, whereas it was constantly observed with the TFL. This carbonization zone, located on the resected zone, tended to be greater as the peak power decreased (Figs. 4 and 5).
The data are presented in Table 2.
Outcomes of Ho:YAG Laser and Super Pulsed Thulium Fiber Laser on Tissue at Different Laser Settings
NM = nonmeasurable; TFL = super pulsed thulium fiber laser.
Discussion
This study found that incision depths and areas of coagulation were greater with the Ho:YAG laser than with the TFL. Although no carbonization zone was found with the Ho:YAG laser, this was constantly seen with the TFL. Although a fiber tip degradation was constantly observed with Ho:YAG laser, except in the case of a long pulse duration and low pulse energy (0.2 J), this was not the case with TFL.
The comparison of our results with the literature is complex because only few studies reported the tissue effects of TFL, and among them the laser settings used during their tests were not detailed. 16,21 The only study, reporting the laser parameters, used stripped 600 μm laser fibers and compared three lasers: the Ho:YAG laser, the TFL, and a diode laser. 22 Contrary to their results, we found a significant difference on incision depths and coagulation zones between the Ho:YAG laser and TFL. However, only one laser setting was evaluated in this study (1.2 J × 10 Hz), without assessment of the effect of pulse duration for Ho:YAG laser and peak power for TFL. The presence of carbonization was reported, this being minimal with Ho:YAG laser and TFL. Similarly, Becker et al. observed the absence of carbonization with a TFL with a peak power of 1000 W, the laser parameters were not detailed. 16 Contrary to these studies, we constantly found a carbonization zone with the TFL, this tending to be more extensive as the peak power decreased, whereas there was none with the Ho:YAG laser.
Regarding our results obtained with the Ho:YAG laser, unlike Emiliani and coworkers we did not find any effect of frequency and pulse energy on incision widths and depths. 27 This difference can be explained by the difference of cutting speed (10 mm/s in our study vs 3 mm/s in their study) and the use of different fiber diameters: 272 and 365 μm in their study against 550 μm in ours, this larger fiber diameter resulting in a lower irradiance ( = power per unit surface). Indeed, Becker et al., 17 as well as Taratkin and coworkers, 21 have shown that with an increasing cutting speed, the incision depths decrease. Similarly to Emiliani et al., 27 we found that laser pulse duration did not affect incision depth. However, contrary to our results, their study demonstrated an influence of the pulse duration on incision widths, this being wider with a shorter pulse duration. Finally, the coagulation zone was more extensive with a higher pulse energy, without influence of frequency and pulse duration, whereas our results found no influence of these factors on this parameter. The other studies on Ho:YAG laser did not detail the laser parameters used, or if reported they differed from those used in our study. 17 –20
Owing to the paucity and the heterogeneity of reports in the literature, our study sheds some light on the differences between Ho:YAG laser and TFL on soft tissue applications. We have been able to observe that tissue penetration (incision depth + coagulation zone) was greater with the Ho:YAG laser than with the TFL, when the fiber tip is in quasi-contact with tissue. These results are in accordance with higher theoretical tissue penetration depth of Ho:YAG laser than TFL. Indeed, the TFL has a wavelength of 1940 nm with a maximum water absorption peak in tissue, and a theoretical tissue penetration depth of 100 μm, whereas the Ho:YAG laser reaches 400 μm because of a wavelength of 2120 nm. 11 Since soft tissues are predominantly composed of water (∼80%), the thermal effects of TFL should then be reduced by a factor of 4 compared with Ho:YAG laser, with the theoretical inference of less tissue disruption and more carbonization for TFL. In theory, this might translate to a more precise incision than achieved with Ho:YAG laser. Our results found greater penetration depths for both lasers than these theoretical depths and we did not report a 4:1 ratio between them. Only few studies compared directly Ho:YAG laser and TFL, and also they did not find such ratio in penetration depth between these lasers. 21,22 These results support a safe profile of TFL for use on living tissue when moving the laser fiber.
Regarding the coagulation properties of lasers, it is important to underline that heating tissue >60°C but not exceeding 100°C causes denaturation of proteins and initial pyrolysis, leading to thermal coagulation (bleaching by coagulation). 28 If all water molecules are vaporized, carbon atoms are released and the adjacent tissues are blackened; this stage is called carbonization. We found significantly larger areas of coagulation with the Ho:YAG laser than with the TFL. However, although no area of carbonization was seen with the Ho:YAG laser, it was consistently seen with the TFL in the resection zone. Thus, the coagulation properties of these two lasers are different, with those of TFL appearing to be more superficial than Ho:YAG laser. These differences can be explained by different laser pulse shapes, different water absorption coefficients of laser, and different peak powers. 29 The pulse spike shape of Ho:YAG laser, as well as its high peak powers regardless of the pulse duration and energy, leads to an “explosive” effect with a rise in temperature and instantaneous vaporization of the water. This instantaneous energy delivery profile cannot lead to a phenomenon of carbonization, but can cause a greater tissue penetration. This resulted in incision widths similar to those of TFL but with greater depths and dilacerations at the limits. Indeed, incision shapes and limits in our study were dysmorphic and inconsistent with Ho:YAG laser compared with the regular limits of incisions with TFL. Similar results on tissue have been reported with Ho:YAG laser in the literature. 21 At the opposite, the nearly rectangular flat-top pulse shape of TFL, its significantly longer pulse duration regardless of energy, its lower peak power, and the longer cavitation bubble lifetime compared with those of the Ho:YAG laser probably result in a temperature rise and energy distribution to the tissue over a longer period of time and in a constant manner during a single laser pulse. These characteristics combined with a maximum water absorption coefficient of laser lead to a tissue vaporization and carbonization effect.
Finally, degradation of the laser fibers was observed with the Ho:YAG laser only. This degradation occurred for energy >1 J, regardless of the frequency, and with short and medium pulse durations only. It was probably linked to a burn back effect because of greater peak power for the short and medium pulse durations than for the long pulse. At the opposite, the absence of laser fiber tip degradation with TFL may be explained by its pulse shape, lower peak power, and longer pulse duration. Thus, efficacy of the Ho:YAG laser during lasering may be affected.
This study has some limitations, the first of which is that the experiments were performed on porcine kidneys and not on prostatic tissue, these nevertheless having similar histologic characteristics. 10,23 –26 The second limitation is that experiments were not performed on live animals with perfused tissues reproducing the surgical conditions, allowing us to assess hemostatic properties. 30,31 Therefore, our results may have been affected by this limitation. However, Khoder et al. showed that the laser effects on tissue are similar between perfused and nonperfused porcine kidneys. 32 Finally, the effect of cutting speed and the distance between the fiber tip and the surface of tissue on histologic parameters have not been studied. Based on the study of Taratkin and coworkers, we may expect a decrease in tissue effect with an increased distance between the fiber and the surface of tissue. 22 About the cutting speed, Becker and coworkers 17 and Taratkin et al. 21 reported a lesser tissue effect when the speed increases. Finally, when the laser fiber is maintained fixed with no displacement, we may expect that the effects found in this study are greater. All these limitations need to be further investigated in future studies.
Conclusions
TFL appears to be an efficient alternative to Ho:YAG laser for soft tissue surgery. The histologic results showed a greater tissue penetration with Ho:YAG laser than with the TFL. Coagulation properties of these two lasers were found to be different, those of TFL appearing to be more superficial with a carbonization effect than larger areas of coagulation with Ho:YAG laser. These results need to be investigated in vivo to assess the clinical impact of these differences and find the optimal settings for laser prostate enucleation.
Footnotes
Author Disclosure Statement
O.T. is consultant for Boston Scientific, Coloplast, EMS, IPG Medical, Olympus, and Rocamed. S.D., T.G., F.P., E.C., and L.B. have no conflict of interest to declare.
Funding Information
No funding was received for this article.