
Abstract
Context:
Recently developed concepts for higher efficacy extracorporeal shockwave lithotripsy with low-pressure wide focus systems resulting in finer fragmentation of the calculi.
Objective:
To compare two different electromagnetic shockwave sources (low-pressure wide focus [Xinin Lithotripter, XL] vs high-pressure small focus [Siemens Lithoskop, SL]) by sound field measurements and in vitro fragmentation.
Evidence Acquisition:
The CS-2012A XX-ES lithotripter (self-focusing electromagnetic shockwave generator with concave spherical curved electrical coil; XL) was compared to the (SL) (electromagnetic generator with a flat electric coil with an acoustical lens). Different sound field measurements were performed using a fiber-optic hydrophone. Measurements at three different power settings (XL: 8.0, 9.3, and 10.3 kV and SL: Level 1, 5, and 8). Ten AST stones and 15 BegoStones (9.3 kV, Level 3) with a frequency of 90/minute (SL) and 20/minute (XL). Number of impulses to the first crack and for complete stone comminution (residual fragments <2 mm) was documented.
Results:
The median number of shockwaves for the first crack in AST stones with the XL was 12 (10–14) and 7 with the SL (6–9). Complete disintegration was accomplished after 815 (782–824) shockwaves with XL and 702 (688–712) with SL. The difference was not statistically significant. The median number of shockwaves to produce the first crack in BegoStones was 524 (504–542) with XL and only 151 (137–161) with SL. Numbers of shockwaves for complete disintegration did not differ significantly (XL: 2518 vs SL: 2287). Using a wide focus with low pressure shows more homogeneous disintegration.
Conclusion:
Two stone models showed significant differences regarding form and time of the initial fragmentation. Impulses for stone comminution did not differ significantly. The advantages of a low-pressure wide-focus system include minimal trauma and a homogeneous fragment size but is more time consuming. High-pressure small-focus systems are clinically effective.
Introduction
There is still an ongoing discussion, which type of shockwave geometry and distribution of energy enables optimal stone fragmentation. 1 –4 The initially used electrohydraulic generator of the Dornier HM3 5,6 had a large focal zone (100 × 16 mm) and low peak pressure (32 MPa). Second and third generation lithotripters 7 –9 used a small focus (e.g., Modulith Siemens Lithoskop [SL] 20: 28 × 6 mm) and high pressure (100 MPa). Both systems proved to be effective in clinical applications of extracorporeal shockwave lithotripsy (SWL). 10 However, there is still the debate, which concept would be more favorable in terms of re-treatment rate, complications, and overall efficacy. 2 –4,11 This discussion was stimulated by several physicists presenting different theories of initial stone fragmentation (Table 1), such as tear and shear forces, 1 spallation, 12 quasi-static squeezing, 13 cavitation, 14 dynamic squeezing, 15 or momentum transfer and inertia. 3
Summary of Existing Theories for Initial Stone Fragmentation
We were able to perform sound field measurement on two different electromagnetic lithotripters offering either a low-pressure wide-focus (CS-2012A XX-ES [Xinin Lithotripter, XL]; Xixin Medical Instruments, Suzhou, China) or a high-pressure small-focus system (SL; Erlangen, Germany) combined with in vitro tests using two standardized stone models aiming to add more comparable data to this discussion. We want to not only focus on the initial stone fragmentation but also on final stone comminution. 16
Material and Methods
Description of the lithotripters
Xinin Lithotripter
The self-focusing electromagnetic shockwave generator developed by Eisenmenger 15,17 consists of a concave spherical curved electrical coil and a close to fitted concave metal membrane. The generator is integrated in the over-couch arrangement of the device providing a cushion for coupling. Stone localization is performed by use of a lateral ultrasound probe (45° angle). Generator voltage can be adjusted to maximal 10.3 kV (equivalent to 27.5 MPa). Pulse repetition rate can be varied between 0.33 and 1.67 Hz in 7 settings. Therapeutic applications during clinical SWL are recommended by the manufacturer at 9.3 kV and 0.5 Hz. 17
Siemens Lithoskop
This lithotripter uses an electromagnetic generator consisting of a flat electric coil and an acoustical lens. The generator is integrated in a C-arm to provide both under- and over-couch coupling. Stone localization is performed by using a parallel fluoroscopic C-arm to provide in-line fluoroscopy. Generator voltage can be adjusted to a setting of maximal 8 (equivalent to 83.4 MPa). Repetition rate can be adjusted to 1 Hz–1.5 Hz–2 Hz. Therapeutic applications are recommended by the manufacturer between intensity setting of Level 3 to 5 at 1.5 Hz.
Experimental setup for sound field measurements
Measurements of the acoustic pressure signal p(x,y,z) were performed by a fiber-optic hydrophone FOPH 2000 (RP acoustic, Germany). For signal recording, the photodetector of the device was attached to an oscilloscope. The sensitive element of the hydrophone is the tip of an optical glass fiber (diameter 100 μm) fixed to the holder of the XYZ-positioning system. Because of the optical measurement principle, the FOPH is insensitive to electromagnetic interferences. The sensitivity of the optical hydrophone is 2 mV/MPa and the accuracy ±5%.
For the sound field measurement of the XL, the foam on the therapy table was removed and the water-filled test chamber was fixed on the metal frame of the table (Fig. 1). For localization of the target location (i.e., geometric focal point), a brass pointer provided by the manufacturer was used. The glass fiber tip of the fiber-optic hydrophone was fixed in a holder of the XYZ-positioning system (Fig. 1).
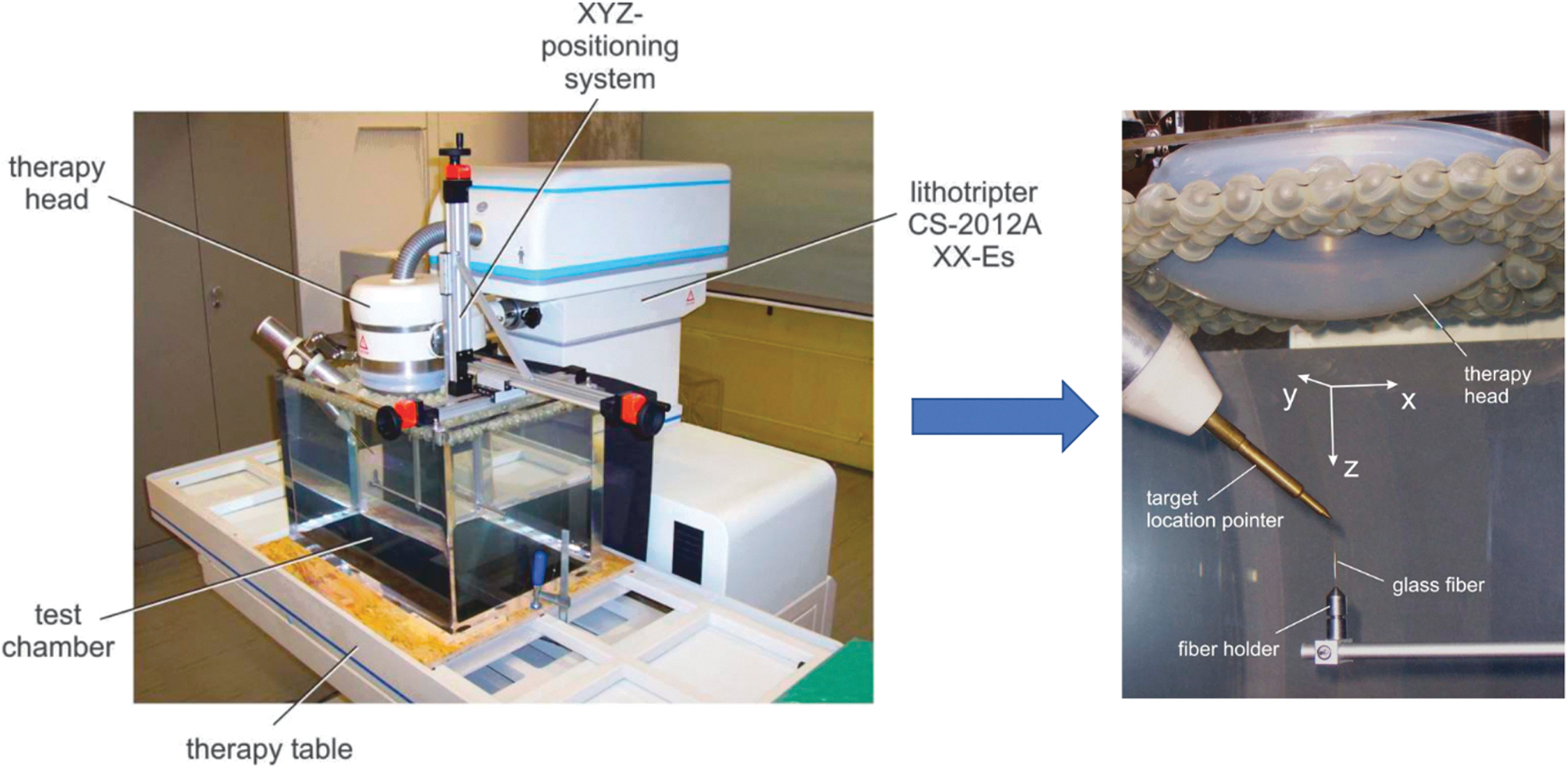
Setup for the sound field measurements using a fiber-optic hydrophone (FOPH 2000). At the CS-2012A XX-ES, the foam on the therapy table was removed and the water field test chamber was fixed on the metal frame of the table. Localization of the target location of the lithotripter (i.e., geometric focal point) using a brass pointer provided by the manufacturer. The glass fiber tip of the FOPH 2000 is fixed in the fiber holder of the XYZ-positioning system.
The following parameters were evaluated on both lithotripters: pulse-to-pulse variation and focus measurement, including focal size (−6dB), focal volume (ellipsoid), rise time, acoustic pulse energy, and energy flux density at the focal zone. Measurements were carried out at three different power settings of both devices corresponding to low, medium, and high intensity level (XL: 8.0, 9.3, and 10.3 kV and SL: Level 1, 5 and 8). For the evaluation of the measured data, two computer programs were used (CALDEC FOPH300v1.0.01 and Origin 7.5G75853.0853).
Description of the used stone models
BegoStones are made of commercially available super-hard plaster originally developed for dental applications. Liu and Zhong 18 characterized them in comparison to human kidney stones comparable to calcium oxalate monohydrate. AST stones are made of dental cement mixed with glass microspheres and are considered close to calcium oxalate dihydrate stones. 19 Ten AST stones and 15 BegoStones were treated with each lithotripter using standard clinical settings (XL: 9.3 kV and SL: Level 3) for stone fragmentation with a frequency of 90/minute (SL) and 30/minute (XL). To avoid spreading of the fragments, the stones were positioned on a mesh with 2 mm pores and surrounded by a rubber ring (Fig. 2). The stone was localized either by use of target location pointer (XL), respectively, in-line fluoroscopy (SL). We noted the number of impulses required for the first crack as well as the number of shock waves for complete stone comminution, which was defined by residual fragments less than 2 mm.

Setup for the in vitro stone models using AST stones and BegoStones. To avoid spreading of the fragments, the stones (i.e., AST stone) were positioned on a mesh with 2 mm pores and surrounded by a rubber ring. At the CS-2012A XX-ES, the stone was localized either by using target location pointer or by using lateral ultrasound (BK 2000; B&K Medical, Herlev, Denmark).
In clinical use, different settings have different indications, that is, to treat ureteral (high energy) vs renal stones (medium energy). Basically, the two stone models we have used should represent a hard stone (BegoStone), such as calcium oxalate monohydrate, and a softer stone (AST stone), such as calcium oxalate dihydrate. The effect of the applied shock wave energy on the stone includes initial fragmentation (“first crack”) and stone comminution. Most theories about stone fragmentation focus on the initial fragmentation (Table 1). Therefore, we had to evaluate the number of impulses until the first crack with both devices and the respective energy levels, as well as the number for complete disintegration. Obviously, XL and SL have different energy levels and repetition rate recommended by the manufacturer.
Statistical analysis
The U test, Kruskal-Wallis test, and regression were used for statistical analysis. All statistical calculations were performed using SAS 9.2 with the significance level set at p = 0.05.
Results
Physical measurements
Xinin lithotripter
Except from a little loss of peak pressure after the first impulse, the pulse-to-pulse variation was minimal (Fig. 3a). It is expected that the trigger spark gap of the device is causing this effect. The rise time of the shock wave front decreases with increasing generator voltage from 395 ns at 9.3 kV to 285 ns at 10.3 kV, which is in the range of the Lithoskop at Level 3 with 313 ns (Fig. 3b). Focal size and volume decrease with increasing generator voltage. The comparison of both shock waves at the clinically used power setting (9.3 kV, respectively, Level 3) demonstrates two significant differences: the focal size of the XL is more than 10-fold larger compared with the SL at Level 3 (26.5 cm vs 1.6 cm3) and the negative pressure is very pronounced in the low-pressure system (Fig. 3). Accordingly, the peak positive pressure (XL: 16–24 MPa vs SL: 39–83 MPa) and energy flux density (XL: 163–254 J/m2 vs SL: 397–1,373 J/m2) and the acoustic pulse energy (XL: 11–16 mJ vs SL: 20–65 mJ) are significantly lower in the XL.

Comparison of pulse-to pulse accuracy of both electromagnetic shock wave sources.
Siemens Lithoskop
Pulse-to-pulse variation: The pulse shape is highly reproducable without any loss of peak pressure (Fig. 3b). The measurements confirm the characteristics of a high-pressure small-focus lithotripter. The focal dimensions at the therapeutic level are 5 × 120 mm compared to 15 × 220 mm of the XL. The maximal peak positive pressure at Level 8 amounts to 83.4 MPa with a very short rise time of 19 ns. Interestingly, the focal volume does not change significantly between Level 3 and Level 8 (1.6 vs 1.8 cm3).
Stone experiments
The XL 9.3 kV was used for disintegration of the AST stones and 10.3 kV for the BegoStones (Table 2). The median number of shock waves to produce the first crack in the AST stones was 12 (10–14) (Fig. 4). Complete disintegration was accomplished after 815 (782–824) shock waves with the XL. The median number of shock waves to produce the first crack in BegoStones was 524 (504–542) with the XL, complete disintegration was obtained at 2,518 shock waves.
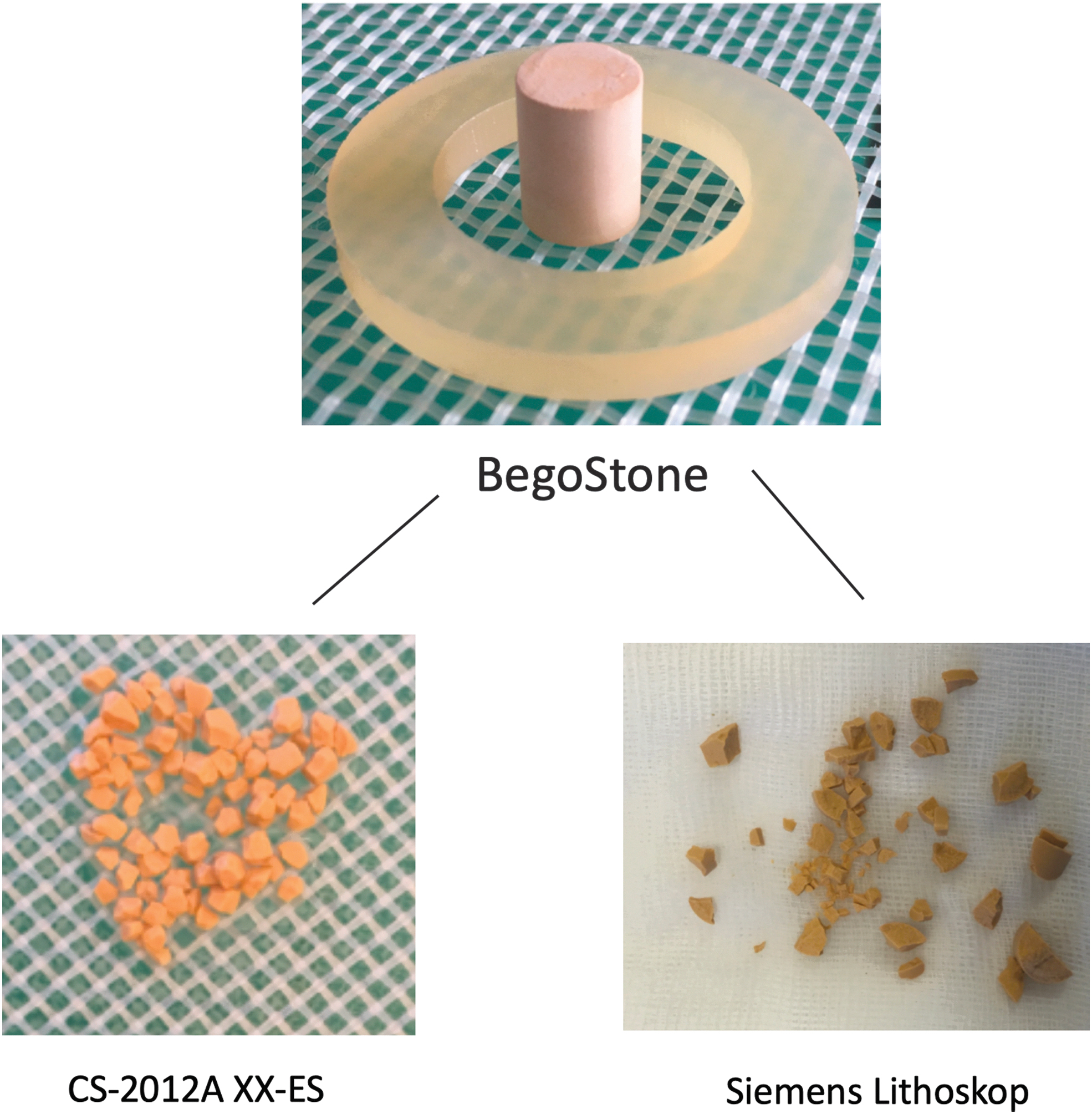
Comparison of the quality of fragmentation using the hard BegoStone model. Note the similar sizes of the fragments when using the wide-focus system (CS-2012A XX-ES) compared to the irregular shaped fragments after shockwave lithotripsy with small-focus system (SL).
Two Different Artificial Stones were Treated by Each Lithotripter (Xixin XX-ES and Siemens Lithoskop)
Complete disintegration was defined by fragments <2 mm.
SL = Siemens Lithoskop.
Using the SL Level 3 was sufficient to disintegrate the AST stones and BegoStones. For the first crack, a median number of shock waves of 7 (6–9) was needed (Fig. 4). For complete disintegration, 702 (688–712) shock waves with the SL were needed. The first crack in BegoStones was seen at only 151 (137–161) shock waves with the SL with a complete disintegration at 2,287.
The initial fragmentation line using the XL was orthogonal to the shock wave front corresponding to the theory of quasi-static squeezing, whereas with the SL the first crack was in the lateral third of the stone corresponding to the theory of spallation (Table 1). The difference regarding the number of shock waves for complete disintegration for AST and Bego stones, however, was not statistically significant. In both models, refocusing of the shock wave source was 40% more often required when using the SL. Based on our measurements, the fragments produced by the XL were more uniform (2 mm) than the fragments produced by the SL (2–4 mm) (Fig. 4).
In summary, regarding early disintegration, the SL was superior over the XL in both stone models. However, the number of shocks required for complete stone disintegration was comparable for both lithotripters, regardless of the type of artificial stone. Owing to the lower application frequency (0.5 Hz vs 1.5 Hz), the XL is significantly more time-consuming. The fine and equal fragmentation achieved with the low-pressure wide-focus system support the theory of binary fragmentation by quasi-static squeezing (Fig. 4). Another advantage is the lower need to reposition the lithotripter.
Discussion
Decreasing use of SWL
The use of SWL decreased within the last decades because of changing indications and recent technological developments, such as flexible ureteroscopy and percutaneous nephrolithotomy. 4,20,21 Although SWL offers still the most minimal invasive treatment for urolithiasis, more and more patients are treated by ureterorenoscopic or percutaneous stone removal. Endoscopic stone treatment achieves fine fragmentation using the dusting mode of the holmium laser, which has basically abolished the risk of a steinstrasse. Therefore, shockwave lithotripsy can only survive if the quality of fragmentation can be significantly improved. 22,23
Role of focal size of lithotripters
Based on the discussion of different mechanisms of stone disintegration (Table 1), several shockwave sources have been developed during the last years. However, none of them was implemented in last generation lithotripters. Most technological innovations of recent lithotripters focused only on integration of navigation systems to localize the stone or camera-controlled quality of coupling the shock wave energy. 2,4,11,24,25
Just recently, Wess and Mayer 3 published an article presenting a new theory for stone disintegration based on momentum transfer and inertia mainly as an argument against the advantages of a wide focus. The aim of our study was not to argue against the clinically proven efficacy of the two devices, but to analyze advantages and disadvantages of both concepts to stimulate future developments in the field of SWL.
Advantages of wide-focus low-energy systems
The sound field measurements of both devices demonstrate significant differences. In the therapeutically used setting (XL: 9.3 kV and SL: Level 3), the focal volume of the wide-focus system (XL) is 16-fold larger than the SL system.
On the other hand, the peak positive pressure is significantly lower (XL:16 MPa; SL:39.4 MPa). The high-pressure system achieves in both stone model earlier initiation of the fragmentation (“first crack”); however, for complete disintegration, no significant differences were encountered. It has to be emphasized that only the highest power setting of the CS-2012A XX-ES (10.3 kV corresponding to 24.3 MPa) was able to fragment BegoStones, which have a compressive strength of 60 MPa and a tensile strength of 12 MPa (18). On the other hand, an almost double acoustic energy output per impulse of the SL (SL: 20.5 vs XL: 10.8 mJ) did not result in less shock waves for complete stone disintegration of the AST stone (Table 2). For the BegoStones, the differences were less impressive (SL: 20.5 vs XL: 16.3 mJ).
Neisius and colleagues modified the acoustic lens of the original electromagnetic System C of Siemens by an annular ring cut. 26 This resulted in a significant enlargement of the focal zone because of superposition of a second delayed wave originating from the same electromagnetic shock wave source. The focal point has to be moved 40 mm upwards along the z-axis. The new lens had a 22% lower peak pressure p+ (39 MPa vs 52 MPa) and 29% lower peak energy flux density with a 49% broader focal width (11 mm vs 7.4 mm) than the original lens. The new lens parameters (p+ = 39 MPa, peak energy flux density = 0.6 mJ/mm2, and focal width = 11 mm) are similar to those reported for the HM3. The CS-2012A XX-ES shows even lower pressure (p+ = 24 MPa, focal width = 11.8 mm, and energy density 0.25 mJ/mm2). Despite the lower peak pressure of the modified lens, the stone comminution using BegoStones was similar; however, in the porcine model, the shock wave-induced renal injury was minimal, whereas in the older version, more hemorrhagic lesions were encountered. 26 Evan et al. also did not encounter any significant lesion in the model of the porcine kidney, when testing the XL device. 27
The role of fine fragmentation
Although the minimal toxicity of low-pressure wide-focus systems is widely accepted, the efficacy with respect to stone comminution is still under discussion. 3 Most theories of stone fragmentation focus on the initial fragmentation, because further stone comminution is very difficult to calculate in a respective model, 11 –15 Table 1. Using standardized stone models, the therapeutic range of different shock wave sources can be compared. 19
Obviously, the high-power small-focus system achieves a more rapid initial fragmentation (Table 2). However, the type of fragmentation differs in both systems. According to the theory of quasi-static squeezing and dynamic squeezing, the use of a wide-focus system resulted in a fracture line orthogonal to the blast path, whereas with the small-focus device, the initial fragmentation occurred in the lateral part. Interestingly, the amount of shock waves for fine fragmentation (<2 mm) of the test stones did not differ significantly in both types (Table 2). However, the size of the individual fragments was more homogeneous when using the XL (Fig. 4). This again supports Eisenmenger`s theory of binary fragmentation. 17 Fine disintegration into similar sized small fragments is preferable to minimize the risk of a steinstrasse. 22 Further clinical studies will show the efficacy and outcome of such fine stone fragmentation. Unfortunately, the clinical data are not yet available. However, it was really important to compare the two lithotripters before performing a clinical trial to see the efficacy of the XL and to test the different power settings
New concepts of extracorporeal stone lithotripsy
Recent technological developments like Burst wave lithotripsy (BWL) or high-frequency SWL (HF-SWL) can achieve such fine pulverization of stones. 28,29 Burst waves are modified ultrasound waves applied at a high frequency (390 kHz) during a short time (59 microseconds). In previous experiments, BWL achieves a much finer fragmentation in a shorter period. 28 In the first clinical case, the duration for BWL was only 9 minutes with maximal 7 MPa and a repetition rate of 10 to 17 Hz. 30 Immediately after BWL, ureteroscopy confirmed complete stone comminution into small particles of less than 2 mm.
Rassweiler-Seyfried used an electrohydraulic source generating high-frequency shockwaves (100 Hz; Storz-Medical, Switzerland) with the same amplitude and pulse behavior as standard shockwaves. They were able to pulverize BegoStones in less than 2 minutes. Using a standardized model of perfused kidney, such high-frequency shockwaves did not show any significant renal lesion. 29
Only new methods of fine fragmentation may represent a valid option for long-term survival of SWL either using low-pressure wide-focus systems or even developments such as burst or HF-SWL. It is up to the manufacturers to bring these promising technologies on the market.
One limitation of the XL is that the intervention is more time-consuming, owing to the lower application frequency. On the other hand, you do not need to reposition the lithotripter, attributable to the wide focus, but we are not able to completely evaluate the impact of the lower repetition rate on the outcome of our study in the stone model.
Conclusions
Sound field measurements using a fiber-optic hydrophone were able to distinguish significant differences of two electromagnetic shockwave generators providing either a low-pressure wide focus or a high-pressure small focus. Two standardized stone models showed significant differences regarding form and time of the initial fragmentation (“first crack”), however, impulses for stone comminution did not differ significantly. The advantages of a low-pressure wide-focus system (XL) include a homogeneous fragment size as we found in our trial and minimal trauma as shown in a previous preclinical trial. High-pressure small-focus systems such as SL are clinically effective. However, the inhomogeneous fragmentation may lead to a higher risk of steinstrasse or even re-treatment. Rapid fine fragmentation is one of the major issues brought up by recent alternative extracorporeal technologies such as BWL or HF-SWL. Further basic research as our trial is required to improve SWL technology and outcomes to evolve to preclinical and clinical trials.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
There was no funding for this study.