
Abstract
Background:
Different consoles have been described for the da Vinci single-port (SP) surgery since it was cleared by the FDA in November 2018. However, the literature still lacks studies identifying factors related to the SP learning curve and how to overcome the technological limitations, especially in terms of maintaining acceptable positive surgical margins (PSMs). This study describes our perioperative experience implementing a safe SP approach to radical prostatectomy (RP) while minimizing PSM, especially during the initial learning period.
Materials and Methods:
We performed a retrospective analysis of 100 consecutive patients with prostate cancer who underwent RP with the SP robot from June 2019 to December 2020 (IRB 237998). We accessed the perioperative data, pathology report, and short-term oncologic outcomes. We also represented our PSM trends in 100 consecutive cases, discussing potential factors for minimizing the learning curve impact on positive margins and outcomes. Medians and interquartile ranges, as well as frequencies and proportions, were reported for continuous and categorical variables, respectively.
Results and Limitations:
The median follow-up is 14 months (8–17). The cohort has a median age of 62 years (56–68), median prostate-specific antigen of 5.5 (4.3–7.7), median preoperative Sexual Health Inventory for Men (SHIM) of 20, median American Urological Association (AUA) of 7 (3–11), and median body mass index of 25.4 (23.4–27.4). The median total operative time was 114 minutes (104–124), the median console time was 80 minutes (75–90). No intraoperative complications were reported. The overall rate of PSMs was 15% (5% were pT2 and 10% were pT3).
Conclusions:
The SP approach to RP is feasible, safe, and with acceptable intraoperative performance. In this study, we have described crucial factors for considering selection criteria in candidates for SP-robot-assisted RP. We believe that with an appropriate patient selection, this robot can be safely implemented without increasing positive margins and compromising the outcomes, especially during the learning curve period.
Introduction
Robot-assisted radical prostatectomy (RARP) and its outcomes are already established in the literature. 1 Different consoles have been described for this surgery since the first da Vinci Standard until the novel da Vinci single-port (SP), cleared by the FDA in November 2018. 2,3 However, the literature still lacks studies identifying factors related to the SP learning curve and how to overcome the technological limitations for optimizing operative outcomes. Current studies have described the positive surgical margins (PSMs) in radical prostatectomy (RP) ranging from 6% to 22% in patients with clinically localized prostate cancer. Some authors reported >50% of PSM depending on the disease extension, surgeon's experience, and type of robotic console used, such as the da Vinci SP. 4 –8
The SP approach to RP was described by different authors, mostly in small series with <110 patients, and the overall rates of PSM range from 11% to 55%. 3 However, most studies included the initial experience and learning curve with this console, which may overestimate these PSM rates. In this scenario, while implementing the new da Vinci SP, it is crucial to minimize the learning curve impact on the surgical outcomes, especially in terms of PSM because of the higher rates of biochemical recurrence (BCR). 9 Therefore, after a series of studies, we reported the technical modifications necessary to perform single-port-robot-assisted radical prostatectomy (SP-RARP) in a prostate cancer referral center, describing the selection criteria adopted while choosing SP-RARP candidates to optimize outcomes during SP robot implementation. 10,11
After achieving >100 cases performed with this new platform, our objective is to describe the experience and outcomes of a high-volume center implementing the SP approach to RP while minimizing PSMs, especially during the initial learning period.
Patients and Methods
The data of one hundred consecutive patients with prostate cancer who underwent SP-RARP (transperitoneal approach) from June 2019 to December 2020 were collected and analyzed retrospectively. All surgeries were performed by the same surgeon (V.P.) using the same technique and the same tableside assistant. 10,12 All patients were explained about potential surgical complications and signed a consent term for the SP surgery. The study was performed under the Institutional Review Board (IRB) number 237998.
Our study's primary endpoint is to evaluate the PSMs since our first SP-RARP and discuss factors that may minimize PSM rates in patients operated on with the SP robot. The secondary endpoint is to report our operative performance in 100 consecutive SP surgeries evaluating total operative time (OT), console time, blood loss, and complications.
da Vinci SP modifications and challenges
Compared with the standard multiport platform, despite the number of trocars, the SP robot also presents some modifications of the instruments and endoscope mechanisms. 10 Instead of having four independent trocars to house each instrument and endoscope, the SP has only one trocar, in which three instruments and one flexible endoscope are placed at the same time. Therefore, after performing >100 SP-RARP at our center, we could identify different challenges during the SP implementation and learning period that may interfere with the surgical outcomes.
Trocar placement
Different techniques have been described for the SP-RARP trocar placement. 3 In our institution, we place the robotic trocar in the midline above the umbilicus, 20 cm away from the pubic bone, using Hasson's technique. 13 We also place a 12 mm assistant trocar in the right lower quadrant (SP plus one).
Each SP instrument has two different articulation points (elbow and shoulder-like), and the appropriate working angles and rotations are achieved when these instruments are entirely deployed from the trocar. Therefore, the correct trocar placement is crucial for attaining the optimal triangulation and working distance from the surgical site. In our experience, placing the trocar too close to the prostate, with a distance <15 to 20 cm from the pubis, inhibits the appropriate instrument triangulation, increasing internal clashing and restricting the endoscope movement.
Every new technology must be carefully implemented and adapted to patient needs. Therefore, in our experience, the assistant trocar was crucial during the learning period because it allowed us to maintain our established RARP technique, minimizing the learning curve impact on the surgical outcomes. In addition, the assistant helps to perform suction and hemostatic clipping, which benefits the patient with OT reduction.
Different endoscope angles and working distances
The SP presents modifications in the working distance and endoscope angles that demand a new learning curve. Even with the appropriate trocar placement and instrument triangulation, the working distance differs from the previous multiport console. Although the Xi robot enables a close view during the surgery, the SP demands a wider distance (similar to the laparoscopy) because all arms are working simultaneously with constant repositioning to avoid clashing and movement restrictions.
The flexible endoscope has different settings necessary for each surgery step to achieve appropriate angulation and movement. 11 In our experience, the most challenging step is the posterior dissection and nerve-sparing (NS) because, even with a flexible endoscope, the angulation used to view the posterolateral prostate (between the Denonvilliers layers) is not as good as the Xi with the endoscope toggled 30° up.
One extra pedal, named the relocation pedal, is responsible for guiding the endoscope and all instruments to work in a different quadrant. During this maneuver, all instruments must be located at the center of the screen under observation to avoid unexpected lesions outside the operative field. This pedal is often used during the lymphadenectomy to guide the robot to the left and the right pelvic side. However, this relocation process often adds extra minutes to the total OT because it usually happens slowly.
Traction and capacity of dissection
Whereas the multiport Xi console has four 8 mm working ports, the SP has reduced the instrument thickness to 6 mm to enable the surgery with a single trocar. However, this modification impacts the capacity of gripping, traction, and dissection of this robot.
During our study period in the laboratory, we realized that cases with a higher need for traction during the surgery might not be ideal candidates for SP-RARP. The delicate instrument tip and lack of rigid arms reduced the optimal gripping and traction during the surgery. Therefore, to minimize the learning curve challenges, overcome the instrument limitations, and maintain our established surgical outcomes, we identified crucial factors to select SP-RARP candidates.
Preoperative selection criteria for SP-RARP candidates
Our selection criteria for SP-RARP candidates include prostates <80 g, clinical stage (cTNM) ≤T2, body mass index (BMI) <35 kg/m2, no previous abdominal surgeries, and no previous local treatment such as prostate radiation or ablation. We also avoid patients with multiple prostate biopsies and local treatments for benign prostatic diseases such as simple prostatectomy, transurethral resection of the prostate, UroLift
SP-RARP technique
The patient undergoes surgery in dorsal decubitus with pad protection in all articulations and parts in contact with the operative table. After general anesthesia, all patients undergo bilateral Transversus Abdominis Plane (TAP) Block.
15
Our SP-RARP transperitoneal technique follows the same concept and steps of our multiport surgery performed with the Xi.
10
–12,14,16
No abdominal drain is placed at the end of the surgery. The NS is divided into grades, combining the preservation percentage of both sides.
14
We perform our SP-RARP technique with a transperitoneal access according to the following steps: Patient positioning and trocar placement (single port plus one) Bladder dropping and Retzius space access Anterior bladder neck dissection Posterior bladder neck dissection and seminal vesicles approach NS (posterior access and lateral dissection) Prostatic pedicles control with Hem-o-lok clips Minimal apical dissection DVC control with running suture and urethra division Posterior reconstruction and anastomosis Lymphadenectomy.
Postoperative routine and follow-up
All patients receive nonopioid analgesia, heparin for deep vein thrombosis prophylaxis, and stimulation from walking soon after anesthesia recovery. We have reported surgical complications using Clavien–Dindo classification. 17
All patients were discharged the next morning after surgery. The Foley catheter was removed after 5 days, and the first prostate-specific antigen (PSA) examination was performed 6 weeks after surgery. Then, in the first year, these patients had appointments at 3, 6, and 12 months for functional and oncologic outcomes evaluation using PSA, Sexual Health Inventory for Men (SHIM) score, and American Urological Association (AUA) questionnaires. We define continence as the use of no pads and potency as the ability to achieve and maintain erections hard enough to perform intercourse (with or without PDE5). 18 BCR rates were defined as PSA values >0.2 ng/mL in two or more consecutive examinations.
Statistical analysis
The statistical analysis performed is based on established guidelines describing continuous variables as the median and interquartile range (IQR). 19,20 We used absolute and percentage relative frequencies for categorical variables. The statistical analyses used Stata 16 (Stata Corp. 2019. Stata Statistical Software: Release 16. College Station, TX: Stata Corp LLC) and R 4.0.2 (R Core Team, 2020. R Foundation for Statistical Computing, Vienna, Austria). A two-tailed test with p < 0.05 was considered statistically significant.
To evaluate the association between surgeon experience and surgical margin status we fitted a multivariable logistic regression model as previously reported in previous articles describing surgical learning curve. 21 Surgeon experience was entered in the model using restricted cubic splines with knots at the terciles. Differences in case mix were adjusted for by including in the model age, logarithm of preoperative PSA, pathologic Gleason grade (6 or less, 7 or greater), and extraprostatic extension. To produce a learning curve, we used the mean value for covariates to estimate the probability of PSM predicted by the model for each surgical experience level. Learning curves were estimated using R ver. 4.0.5 (R Foundation for Statistical Computing, Vienna, Austria).
Results
Preoperative demography
Table 1 describes the preoperative characteristics reporting the median value with the IQR and the number of patients with the percentage. The biopsy report was described according to the International Society of Urologic Pathology (ISUP) Grade Groups (GrGp). 22
Preoperative Demography Reporting the Median Value with the Interquartile Range and the Number of Patients with the Percentage
AUA = American Urological Association; BMI = body mass index; ISUP = International Society of Urologic Pathology; PSA = prostate-specific antigen; SHIM = Sexual Health Inventory for Men; SP-RARP = single-port-robot-assisted radical prostatectomy.
Intraoperative outcomes
The intraoperative data are represented in Table 2. Estimated blood loss was <100 mL in 78% of the cases, median OT was 114 minutes (104–124), and console time was 80 minutes (75–90). No intraoperative complications were reported.
Perioperative Characteristics Reporting the Median with the Interquartile Range for Continuous Variables and the Number of Patients with Percentage for Categorical Variables
EBL = estimated blood loss; NS = nerve-sparing; OT = operative time.
Pathology report and postoperative outcomes
Table 3 describes the pathology according to the ISUP GrGp and follow-up data. 22 Fifteen percent presented PSMs. One patient had PSA recurrence after 225 days of surgery, and only one patient was readmitted with lymphocele infection after 55 days.
Pathologic Characteristics and Postoperative Outcomes Reporting the Variables as Median with Interquartile Range for Continuous Variables and the Number of Patients with the Percentage for Categorical Variables
EPE = extraprostatic extension; GrGp = Grade Groups; PSM = positive surgical margin.
PSM and surgeon experience since the SP implementation
Figure 1 illustrates the PSM trend for all patients of this study.
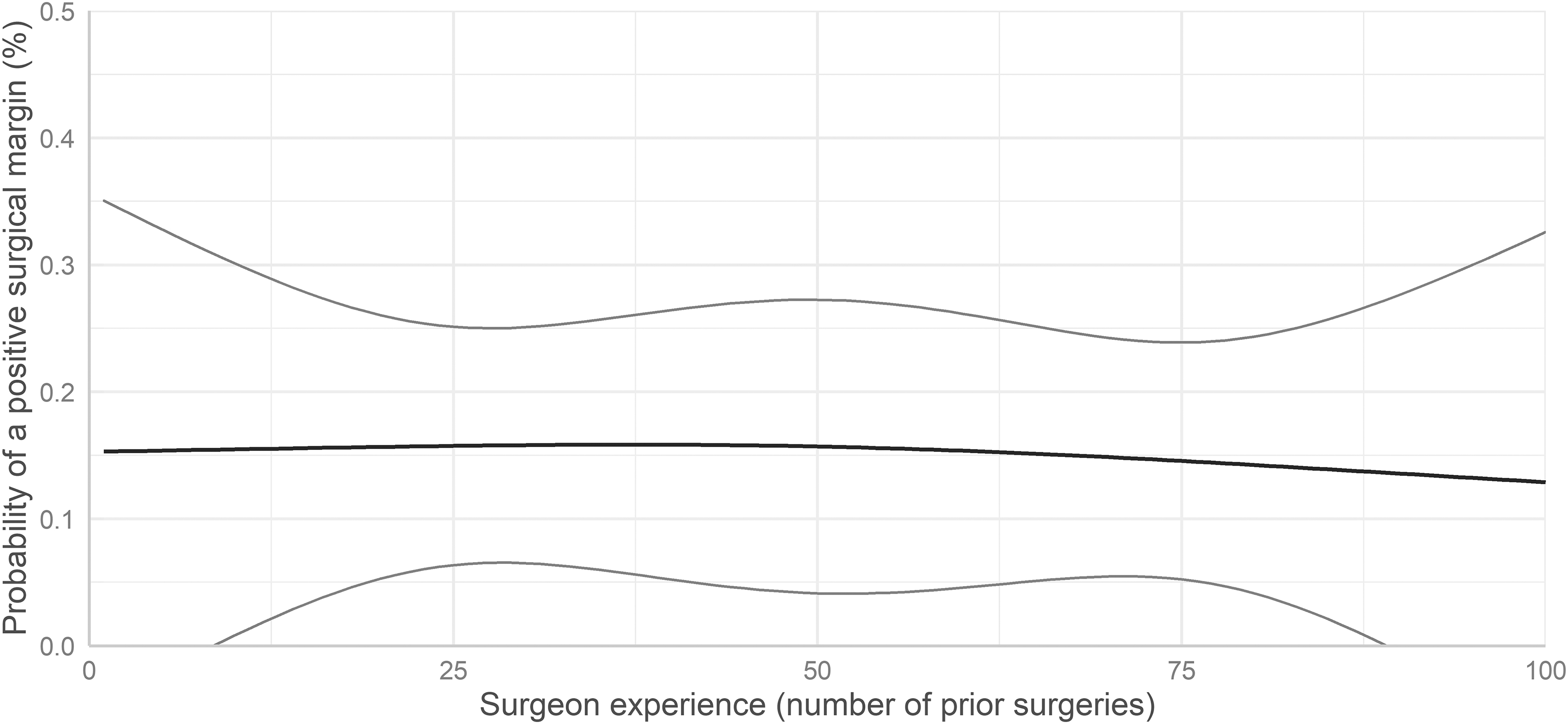
Probability of PSMs since the first SP-RARP according to the surgeon's experience. PSM = positive surgical margin; SP-RARP = single-port-robot-assisted radical prostatectomy.
Discussion
Multiple authors have described the da Vinci SP approach to urologic procedures. The first surgery performed with the SP was described by Kaouk and colleagues in a study reporting 11 patients who underwent RP with a transperitoneal approach. 23 Since then, despite the versatile application in urologic surgeries, RP is the most common use of this robot. However, before adopting this technology in our center, we searched for the available literature, and our concerns while implementing the SP were the rates of PSMs and increased OTs described in radical prostatectomies. 3
Therefore, by performing selection criteria for SP candidates, we minimized the impact of our learning curve on patient outcomes. By selecting the cases, we avoided changing our established surgical technique and outcomes because, in our concept, the technique should be performed according to the patient's needs and not modified according to the platform limitations. In this scenario, with the growing expansion of this robot to other centers, we decided to report the challenges we faced for maintaining the same operative quality offered with the multiport robot.
When designing our selection criteria, according to our experience in RP, we selected factors that normally increase the surgical challenges or potentially impair the surgical outcomes. Patients with previous abdominal surgeries have higher chances of adhesions, and the SP trocar is a limitation to perform lysis of adhesions unless adding extra trocars for a laparoscopic approach, which may contradict the SP concept of doing the surgery with only one or two incisions. Selecting patients with BMI <30 to 35 kg/m2 facilitates the trocar placement and minimizes the challenges because of higher traction needed in obese patients.
Prostates >70 or 80 g, multiple biopsies, previous surgery for BPH, and salvage prostatectomy usually demand increased use of the fourth arm for gripping and greater traction for dissection. Being the instrument's strength and capacity of dissection some of the SP limitations, we avoid using this robot for these candidates. Finally, as mentioned previously, because of the high rates of PSM reported in the literature, 3 we selected patients with clinical stage ≤T2 to minimize the impact of our learning curve on oncologic outcomes.
The oncologic influence of PSM rates was demonstrated by several groups in the literature. In a multicentric study reporting >7000 patients, Karakiewicz and colleagues described BCR rates for PSM of 0.53 (95% confidence interval [CI]: 0.494–0.566) in 5 years and 0.36 (95% CI: 0.28–0.45) in 10 years. 24 Furthermore, some studies have described the relation of Gleason score at PSM and increased rates of BCR. Patients with higher Gleason at the margin are more likely to have BCR than those with lower Gleason. 25 –28 In our study, the only patient with BCR had a postoperative Gleason 7 (3 + 4), PSMs, and pT3 stage. Therefore, in our concept, since most reports are based on retrospective studies, the exact behavior of PSM in RP is still unclear, and we cannot underestimate the tumor grade. PSM must be avoided in all cases, despite the preoperative ISUP classification.
When evaluating the PSM rates since the first SP-RARP of our center, we maintained a constant and acceptable trend even during the learning period. Figure 1 illustrates a plot with a flat learning curve. This means that the rates of positive margins are almost constant as experience grows. In our previous study, the PSM rates were similar and comparable with our multiport (Xi) approach to RP. 14 We recognize that our chief surgeon (V.P) has years of experience in the robotic surgery field and that PSM is also influenced by the surgeon's expertise and refined technique. However, as other centers with experienced surgeons reported an increased PSM using the SP, we believe that these consistent results were mainly influenced by the criteria we used to select the best candidates to overcome the SP instrument limitations.
Another concern was the increased OT of the SP-RARP series reported in the existing literature. 3 Because of the lack of data describing possible factors explaining this OT difference and only a few studies reporting the SP intraoperative performance and outcomes, we have decided to avoid modifying our surgical technique. Thus, since the beginning, we have adopted an assistant trocar on the right lower quadrant to perform Hem-o-lok clipping and blood suction, avoiding excessive cautery on the pedicles, self-clipping, and self-suction. We believe that maintaining our surgical technique using an assistant port for the SP-RARP was another crucial factor in preserving our new OT within an acceptable range.
As previously described, the SP robot is associated with a new learning curve to approach different instrument angles and endoscope movements inside the abdominal cavity. Managing the relocation pedal is another learning process while working in different quadrants, especially during the bilateral pelvic lymphadenectomy. This pedal allows the relocation of all instruments at the same time. Once this movement is performed, the lymphadenectomy technique is similar to the Xi. 29 However, even with the tableside assistant involvement with suction and clipping, we noticed some challenges while dissecting large lymph node templates caused by the delicate instruments and restricted traction capacity, which potentially increases the OT.
Despite its strengths, our study is not devoid of limitations. The retrospective data analysis and its inherent limitations may increase the chances of selection bias. The lack of a comparison group is also another limiting factor. Furthermore, the follow-up period may interfere in evaluating the long-term oncologic impact on these patients with PSM. However, all available literature describing the SP outcomes in RP is recent and restricted to a few centers because of the SP's short period in the market. All current studies in the literature have <100 RARP cases, and none have addressed technical aspects of reducing PSM. To the best of our knowledge, this is one of the largest series describing the SP-RARP oncologic outcomes and crucial factors to reduce the PSMs since the implementation of this new technology.
Conclusion
The SP approach to RP is feasible, safe, and with acceptable intraoperative performance. In this study, we have described different factors for considering selection criteria in candidates for SP-RARP. We believe that with an appropriate patient selection, this robot can be safely implemented without increasing positive margins and compromising the outcomes, especially during the learning curve period.
Footnotes
Authors' Contributions
Conception and design by M.M. and V.P. Data acquisition by S.B. and J.N. Analysis and interpretation by T.R. and D.M. Drafting by M.M., S.K., and I.B. Critical review and intellectual content by V.P. and M.M. Statistical analysis by M.S. Supervision by V.P.
Author Disclosure Statement
According to the International Committee of Medical Journal Editors conflict of interest (ICMJE), the authors Dr. M.C.M., Dr. S.B., Dr. T.R., Dr. S.R., Dr. J.N., M.S., S.K., and Dr. V.P. declare that they have no conflict of interest or competing financial interests related to the article. Dr. V.P. is a consultant for Exact Sciences/Genomic Health, Decipher/Genomic DX, Active Surgical, and AVRA.
Funding Information
No funding was received for this article.