
Abstract
Background:
Managing complex and large renal stones with percutaneous nephrolithotomy (PCNL) is difficult because of the likelihood of residual stones and multiple access. Endoscopic combined intrarenal surgery (ECIRS) is introduced as an improvement to the procedure to manage stones in one session. The objective of this systematic review and meta-analysis is to compare the efficacy and safety between ECIRS and PCNL for treating large and complex renal stones.
Materials and Methods:
We conducted a systematic review in the Embase, Scopus, and MEDLINE databases based on the 2020 Preferred Reporting Items for Systematic Review and Meta-Analyses guideline. Eligible studies comprised both randomized and nonrandomized studies comparing ECIRS and PCNL.
Results:
A total of five nonrandomized studies and one randomized controlled trial were included. The analysis was divided into two subgroups based on the PCNL type, a conventional PCNL (cPCNL) and a mini-PCNL (mPCNL). The one-step stone-free rate (SFR) of ECIRS were significantly higher compared with both the cPCNL (odds ratio [OR] 5.14, 95% confidence interval [CI] 2.54 to 10.4, p < 0.001) and mPCNL (OR 4.27, 95% CI 2.57–7.1, p < 0.001). There were no significant differences in mean operative time and hemoglobin drop between both groups (p > 0.05). The use of auxiliary procedures was significantly higher in both PCNL groups compared with the ECIRS group (OR 0.19, 95% CI 0.13–0.30, p < 0.001). The overall complication rate of ECIRS was lower compared with PCNL (OR 0.43, 95% CI 0.21–0.85, p = 0.02), especially urosepsis, in which the incidence was lower compared with cPCNL (OR 0.14, 95% CI 0.02–0.78, p = 0.02), but not mPCNL (p > 0.05).
Conclusion:
ECIRS is an effective and safe treatment particularly for large and complex nephrolithiasis, with significantly higher one-step SFR, a lower necessity for auxiliary procedures, and a lower complication rate compared with PCNL.
Introduction
Renal or kidney stones are regarded as one of the most common urinary tract disorders affecting ∼12% of the world population. It is one of the oldest recorded human diseases with an increasing global prevalence. 1 Stone presence in kidney calices may induce pain, hematuria, nausea, and fever because of a secondary infection. In several cases, obstructions may occur, which may lead to kidney injury. 2 There are currently various options available for managing the disease, including pharmacologic to surgical approaches. 3,4 To determine the most appropriate management for the disease, the most important factors that need to be considered are the size and location of the stone. 5
Surgery is often required to remove large stones and preserve normal urinary function. According to the latest European Association of Urology guidelines for Urolithiasis, percutaneous nephrolithotomy (PCNL) is the gold standard management for renal stone with a diameter of >20 mm in size. 6 The procedure was introduced as a revolutionary minimally invasive approach for large and complex renal stones. PCNL has been performed for decades and is still recommended as the preferred treatment because of its safety and efficacy. 7 The procedure is less invasive compared with open surgeries and able to remove large renal calculi in fewer steps compared with a single retrograde procedure. 8
Recently, various developments have been introduced in PCNL, including different positions, smaller instrumentation, and a tubeless PCNL. 9 –12 Despite the evolution of technology and instrumentation to the technique, managing complex renal stone with PCNL has always been difficult because of the greater likelihood of residual stone and multiple access requirements. 13 The site and total accesses are not only determined by the location and the complexity of the calculi but also by the accuracy of the initial puncture. It is considered a challenging procedure that requires experience and training. 14 Staghorn stones usually require multiple tracts or sessions, resulting in the increase of complications. 15
Endoscopic combined intrarenal surgery (ECIRS) is a combination of both retrograde and antegrade approaches using both flexible and rigid endoscopes for treating large or complex renal stones in one procedure. It is a novel and revolutionary way of performing PCNL in a modified supine position. This procedure offers the opportunity to monitor the renal puncture, observe tract dilation, and Amplatz sheath advancement. 16 The advantages of faster more accurate needle placement, and the ability to perform concurrent flexible ureteroscopy (fURS) and laser stone fragmentation are why the procedure is considered superior to other procedures based on several studies. 17
The term ECIRS was first used in 2008; however, the method has not been popular for a long time. In the past 7 years, the procedure has become more accepted, shown by the increasing number of articles. Several observational and randomized controlled trial (RCT) studies had reported the superiority of ECIRS over PCNL for treating urolithiasis. 17 –22 However, to the best of our knowledge, a systematic review regarding the comparison between ECIRS and PCNL has not been conducted yet. Therefore, this review aimed to compare the efficacy and safety between ECIRS and PCNL in managing patients with large and complex renal stones.
Methods
Before the conduction of this systematic review, a protocol of objectives, search strategies, inclusion and exclusion criteria, outcome measurements, and statistical analysis methods adhering to the Preferred Reporting Items for Systematic Reviews and Meta-Analysis were prepared and registered in the PROSPERO database (CRD42021229085). 23
Inclusion and exclusion criteria
Online databases consisting of EMBASE, ScienceDirect, and PubMed up to August 2021 was systematically searched. If studies were not identified in computerized search, a cross reference search of qualified studies was performed. Our searches also include the proceedings of several meetings. MeSH terms and keywords were used in the search strategy. The keywords used during the search strategy are listed in Supplementary Table S1.
Search strategy
Published studies were included according to the following criteria: (1) both RCT and observational studies, (2) in English, (3) included adult patients (>18 years old) with a large renal stone (>20 mm), and (4) reported efficacy and safety outcomes listed as follows.
Study selection and data extraction
Five investigators (D.R.W., Y.P.K., F.H., Z.A.R., A.C.F.N., and L.H.) screened all titles and abstract, identified using the determined keywords. The full text of each selected article was then independently evaluated to check whether the study fits the inclusion criteria. Discrepancies were resolved through consultations and discussions until an agreement was achieved.
Objectives and outcome measures
Several outcomes were measured in our study, including stone-free rate (SFR), operative time, hemoglobin (Hb) drop, and urosepsis incidence. SFR is defined as no residual fragments or <4 mm based on CT scan or kidney, ureter, and bladder radiograph (KUB) imaging. The analyzed results were the rates after a single procedure. Operative time is defined as the time between the start and the finish of surgery. Hb drop is determined by subtracting the preoperative Hb concentration with postoperative Hb concentration. Urosepsis is diagnosed based on the presence of sepsis and urinary tract infection. Signs and symptoms of systemic inflammatory response syndrome are main indicators of sepsis. The diagnosis of sepsis may also be made based on the Sequential Organ Failure Assessment (SOFA) score. These outcomes were measured from the comparison between ECIRS and PCNL, both conventional PCNL (cPCNL) and mini-PCNL (mPCNL).
Quality assessment and statistical analysis
Cochrane risk of bias (RoB) tool 2 was used to assess the RoB in RCTs, 24 whereas Newcastle–Ottawa Scale was used to evaluate observed random-effects model was used if I 2 was >50% and the chi-square analysis (p < 0.05) indicated significant heterogeneity across studies, otherwise a fixed-effects model was used. All analyses were performed using the Review Manager software (Version 5.4, The Cochrane Collaboration, 2020).
Results
Eligible studies
Our search process was described in Supplementary Figure S1. Online database search extracted 6 final studies from initially obtained 264 potential studies. Fourteen articles were excluded because of duplications. Upon full-text articles screening, 20 articles were excluded because of unavailability of full text (4), not evaluating patients with large or complex renal stones (3), not comparing between ECIRS and PCNL (7), and review articles (6). The remaining six articles 17 –22 were included in the qualitative and quantitative analysis using standard subgroup and pairwise meta-analysis. The baseline characteristics of the study are summarized in Table 1 and the studies' variables' characteristics are listed in Table 2.
Included Studies' Details and Characteristics
cPCNL = conventional PCNL; ECIRS = endoscopic combined intrarenal surgery; GMSV = Galdakao-modified supine Valdivia; mPCNL = mini-PCNL; PCNL = percutaneous nephrolithotomy; RCT = randomized controlled trial.
Variables' Baseline Characteristics of the Included Studies
Hb = hemoglobin; NR = not reported; SFR = stone-free rate.
Quality assessment
The included RCT by Wen and colleagues 18 had a low RoB, as shown in Supplementary Figure S2. The included observational studies also showed a satisfactory level of quality, as shown in Table 3.
Quality Assessment of the Included Observational Studies Based on the Newcastle–Ottawa Scale
Quantitative analysis of SFR between ECIRS and PCNL
Six studies were included in the meta-analysis for the SFR outcome in Figure 1. Even though the included studies evaluated the SFR at different durations, ranging from 1 day to 4 weeks, the evaluation was performed after a single session of the procedure. Forest plot showed that patients underwent ECIRS had a higher SFR compared with both cPCNL (odds ratio [OR] 5.14, 95% confidence interval [CI] 2.54–10.41, p < 0.001) and mPCNL (OR 4.27, 95% CI 2.57–7.10, p < 0.001). Overall, ECIRS had superior SFR outcomes compared with both PCNL types (OR 4.57, 95% CI 3.02–6.90, p < 0.001). A fixed-effects model was utilized in this analysis because the studies were homogenous (I 2 = 0%).
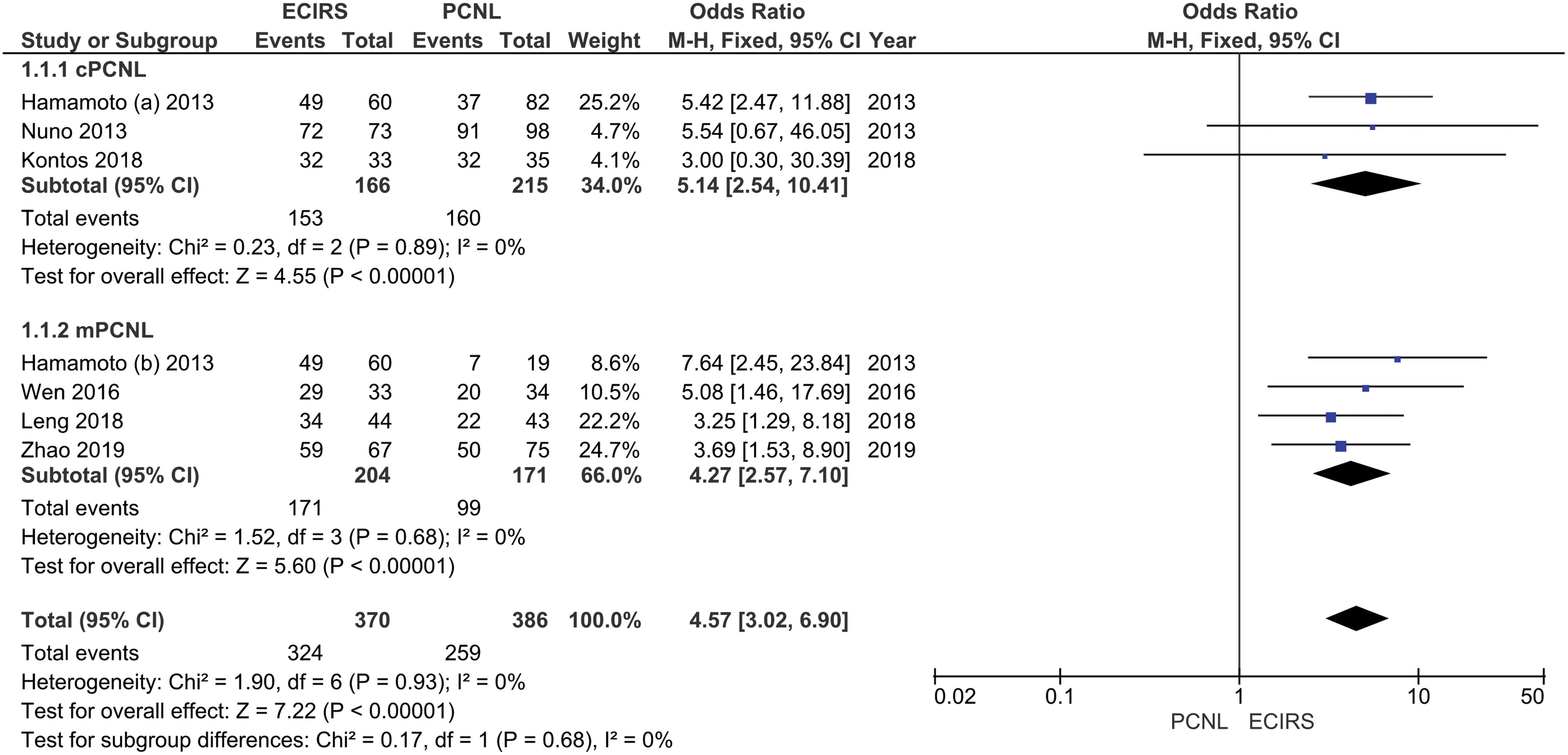
Forest plot of the stone-free rate probability between ECIRS and PCNL. cPCNL = conventional PCNL; CI = confidence interval; ECIRS = endoscopic combined intrarenal surgery; M-H = Mantel-Haenszel; mPCNL = mini-PCNL; PCNL = percutaneous nephrolithotomy. Color images are available online.
Quantitative analysis of operative time between ECIRS and PCNL
Figure 2 displayed the six studies reporting operative time outcomes. No significant difference was found regarding operative time between the use of ECIRS compared with cPCNL (mean difference [MD] −4.29, 95% CI −34.66 to 26.08, p = 0.78) and mPCNL (MD −15.69, 95% CI −47.82 to 16.43, p = 0.34). Our analysis revealed no significant difference (MD −10.93, 95% CI −28.97 to 7.10, p = 0.23) comparing the procedure with both PCNL types. Because of the high heterogeneity (I 2 = 98%), a random-effects model was used.
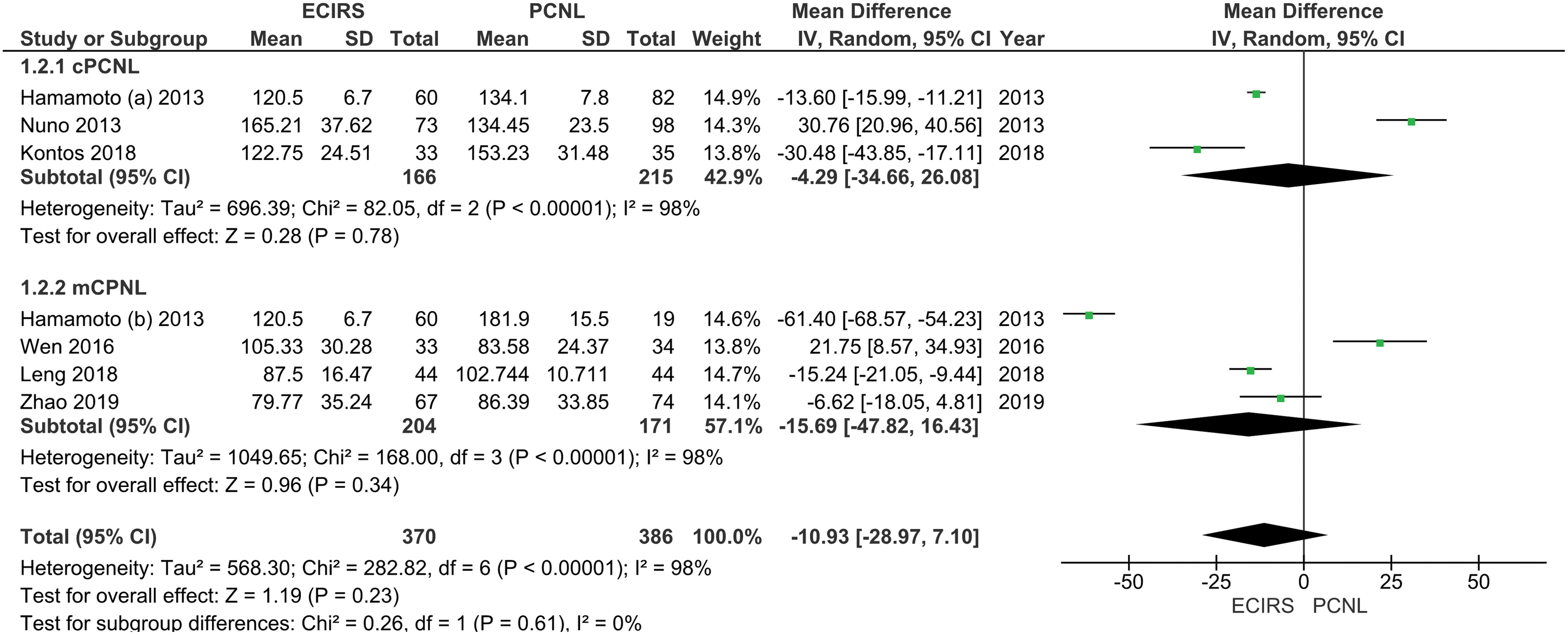
Forest plot of the operative time difference between ECIRS and PCNL. IV = inverse-variance; SD = standard deviation. Color images are available online.
Quantitative analysis of Hb drop between ECIRS and PCNL
Three studies were enrolled in the analysis for the Hb drop outcome, shown in Figure 3. Forest plot showed that there was no significant difference between ECIRS and cPCNL (MD −0.65, 95% CI −1.91 to 0.61, p = 0.31), and mPCNL (MD 0.13, 95% CI −0.20 to 0.45, p = 0.45). All analysis was done by using a random-effects model because of the high heterogeneity of the studies (I 2 = 98%).
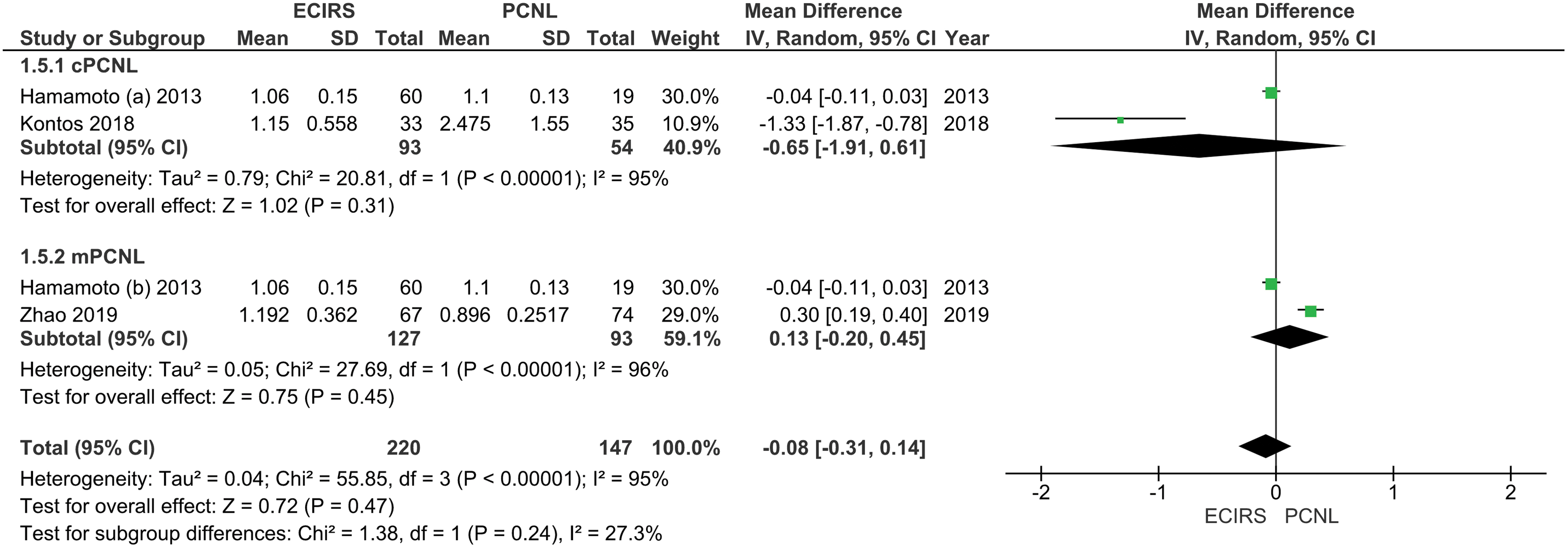
Forest plot of the hemoglobin drop difference between ECIRS and PCNL. Color images are available online.
Quantitative analysis of auxiliary procedures rate between ECIRS and PCNL
There were five included studies, reporting the rate of auxiliary procedures between the ECIRS and PCNL, as shown in Figure 4. A lower rate of auxiliary procedures can be seen in the ECIRS group compared with both the cPCNL (OR 0.13, 95% CI 0.06–0.30, p < 0.001) and mPCNL groups (OR 0.24, 95% CI 0.14–0.40, p < 0.001). Overall, there is a lower rate of auxiliary procedures in the ECIRS group compared with the PCNL group (OR 0.19, 95% CI 0.13–0.30, p < 0.001).

Forest plot of the auxiliary procedures requirement probability between ECIRS and PCNL. Color images are available online.
Quantitative analysis of complication rate based on the Clavien–Dindo classification between ECIRS and PCNL
Three studies reported the complication rate of patients based on the Clavien–Dindo classification. There is no significant difference between the rate of complications of each grade between ECIRS and the cPCNL (OR 0.44, 95% CI 0.18–1.07, p = 0.07) and mPCNL (OR 0.52, 95% CI 0.15–1.72, p = 0.28) groups. However, comparing the overall rate of complications of all grades showed a lower rate of complications in the ECIRS group compared with the PCNL group (OR 0.43, 95% CI 0.21–0.85, p = 0.02) as shown in Figure 5.
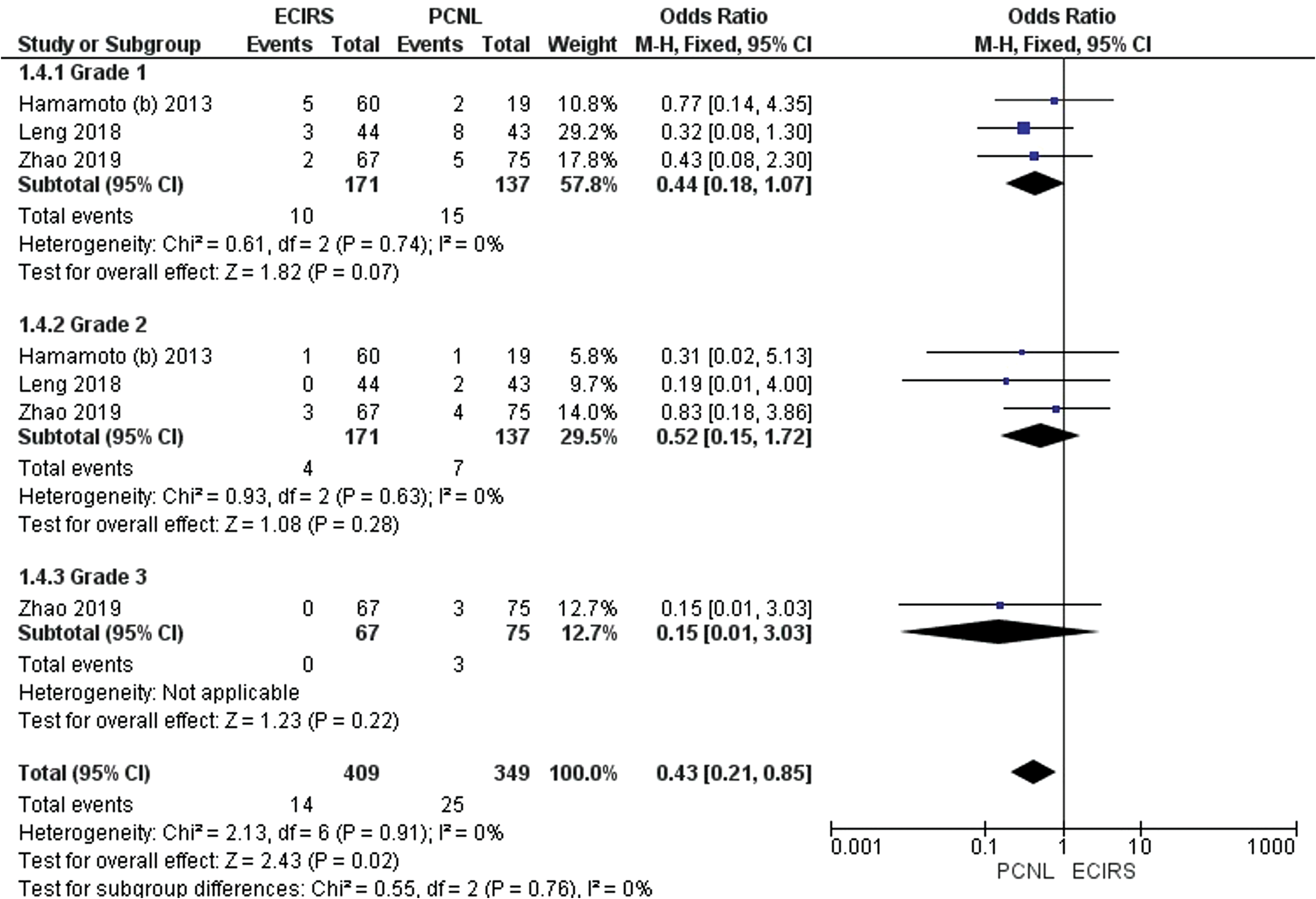
Forest plot of the complication occurrence probability between ECIRS and PCNL. Color images are available online.
Quantitative analysis of urosepsis incidence between ECIRS and PCNL
Four studies reported the incidence of urosepsis, as shown in Figure 6. Our results showed that ECIRS had a significantly lower urosepsis incidence compared with cPCNL (OR 0.14, 95% CI 0.02–0.78, p = 0.02). However, if compared with mPCNL, the difference was insignificant (OR 0.71, 95% CI 0.21–2.41, p = 0.58).
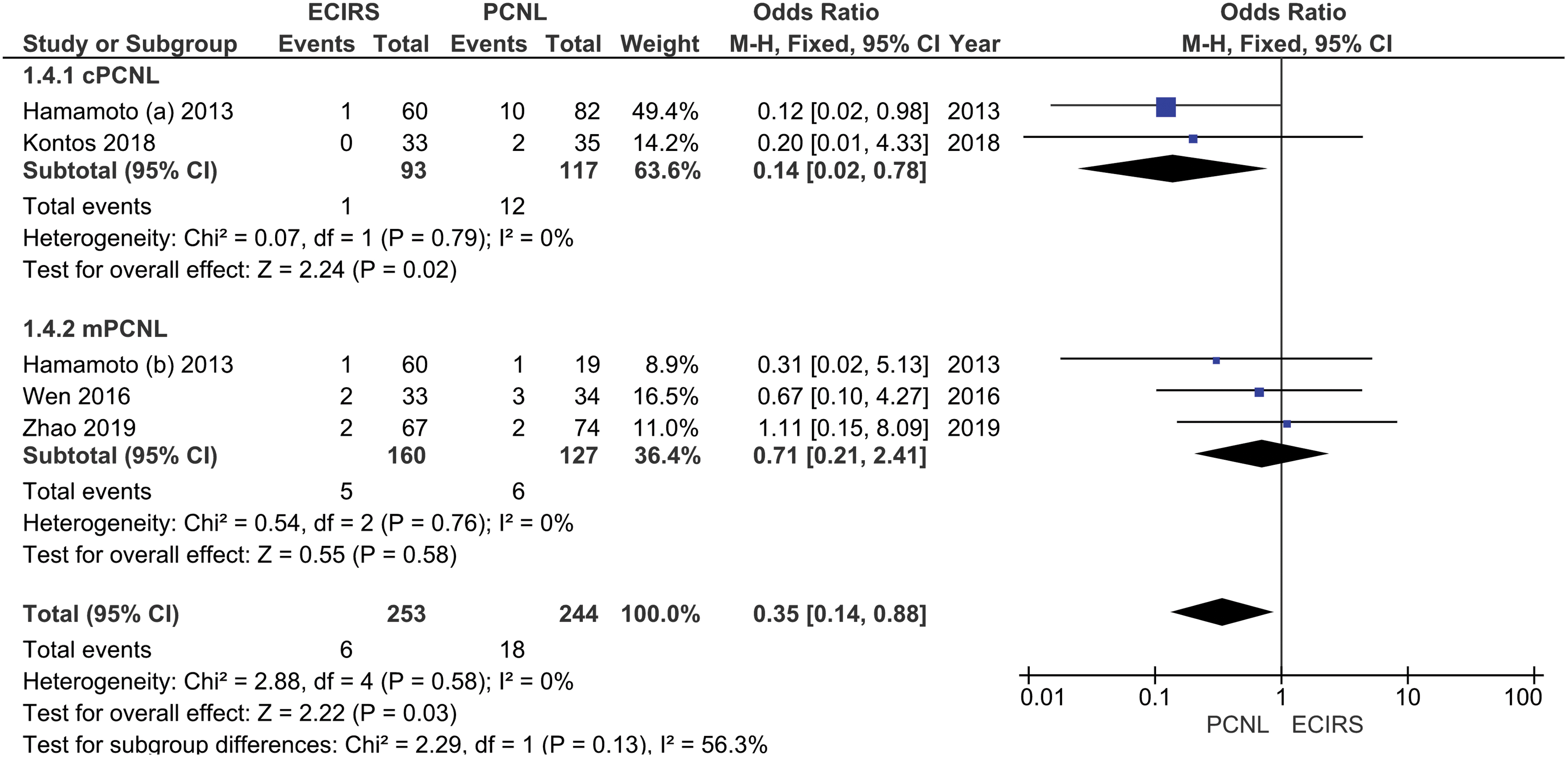
Forest plot of the urosepsis incidence probability between ECIRS and PCNL. Color images are available online.
Discussion
The ideal management of renal stones has been one of the main focuses of studies in the field of endourology for years. Studies have reported innovations and modifications of surgical techniques for treating renal stones. 25 Various techniques, technologies, and procedures have been developed based on the necessity to find the most effective management with a minimal complication rate. 26 The choice of intervention is made based on the clinical conditions as well as the location and size of the stone. Large stones are difficult to pass spontaneously and often require surgery. Retrograde intrarenal surgery (RIRS) and PCNL are currently regarded as the most routinely performed procedures, with PCNL being the gold standard for treating large kidney stones. 27
Endourologic techniques development has led PCNL to become the gold standard for large and complex renal stones management worldwide. 28 Staghorn stones have a complex branched morphology that can fill the renal pelvis and one or more renal calices. 29 Several studies reported unsatisfactory SFRs from one PCNL procedure without an additional procedure. Some procedures require multiple access to the kidney because of the size and morphology of the stones so that bleeding and infection complications are prone to occur. 30 Bryniarski and colleagues 31 reported the advantages of RIRS in the management of stones >20 mm with a lower complication rate than PCNL.
However, this procedure is quite difficult and takes a long time and, therefore, the procedure is less frequently used. To overcome these issues, the ECIRS procedure, which is a combination of retrograde and antegrade approaches, was introduced as an alternative to PCNL for large stones. 8 In the past several years, the ECIRS procedure has become widely accepted in daily practice and is frequently discussed in research articles for the management of large stones. Since 2017, there has been increasing ECIRS utilization in both developed and developing countries. 32 In this systematic review, we found studies comparing the measures of ECIRS with two types of PCNL, namely cPCNL and mPCNL.
Standard PCNL or cPCNL is performed with sheaths size of 24F to 30F, whereas mPCNL is performed with smaller sheath sizes (14F–20F). 33 The analysis was carried out separately because there were differences in efficacy and safety between PCNL procedure sizes with different sheath sizes. 34 In this review, we included five retrospective studies and one RCT. Three studies compared ECIRS with mPCNL, two compared ECIRS with cPCNL, and one study compared all three. All included studies reported SFR results between the two procedures. The size, location, and weight of the stone are important factors in determining the SFR after a single procedure session.
PCNL monotherapy for large or complex stones has been reported to have high SFRs with multiple access in staghorn stones, complex stones, and simple stones (57%, 66%, and 78%, respectively). 26,35 –38 In contrast, the ECIRS procedure, which is usually performed with single percutaneous access, had an average SFR of 61% to 97%. 32 These results are consistent with the comparison of SFR between studies in this systematic review, which showed that ECIRS had a significantly higher SFR than cPCNL (OR 5.14, 95% CI 2.54–10.41, p < 0.001), mPCNL (OR 4.27, 95% CI 2.57–7.10, p < 0.001), and both procedures (OR 4.57, 95% CI 3.02–6.90, p < 0.001).
Hamamoto and colleagues, 19 who compared ECIRS with two PCNL subtypes, strongly recommend the ECIRS procedure that has fewer accesses and a higher SFR for one treatment session. With a combination of both retrograde and antegrade approaches, small fragments of stone can be easily rinsed through PCNL access assisted by retrograde irrigation. After the major part of stones has been resolved, a fURS is used to identify any remaining auxiliary fragments inaccessible to the nephroscope, such as stones located adjacent to the PCNL entrance and minor calices. The simultaneous action of the two procedures improves irrigation and reduces the amount of residual stone. 19
ECIRS is also considered to reduce the need for additional procedures compared with PCNL, which often requires several additional procedures to achieve adequate SFR. 39 A higher SFR leads to a higher probability of multiple procedures after the initial operation. This difference highlighted the drawback of PCNL procedures that often require more than one procedure step or multiple accesses in one operation for complex kidney stones. The included studies in this review showed consistency between the significantly different SFR and the need for additional procedures, in which both PCNL groups showed a higher auxiliary procedures rate compared with the ECIRS group (OR 0.19, 95% CI 0.13–0.30, p < 0.001).
To highlight the difference in SFR as an outcome of success, the initial SFR after a single procedure would be less biased compared with a final SFR, which would have been measured in different durations between patients undergoing possible auxiliary procedures or conservative treatments to help with stone expulsion. Studies showed that PCNL could be performed either with the supine or prone position. In addition, several studies reported that the prone position had a larger area for percutaneous access and a lower risk of splanchnic trauma. 40
Some patients might report an uncomfortable sensation in prone position and operators could experience difficulties if the procedure requires RIRS in the middle of an operation that requires a change in the patient's position. 9 ECIRS procedures are mostly performed in the Galdakao-modified supine Valdivia (GMSV) position, which facilitates the procedure but increases the risk of splanchnic injury. Good operator experience and the ultrasonography (USG) assistance in establishing access can significantly reduce iatrogenic injury. 22 Studies by Scoffone and colleagues 41 support the evidence that GMSV positioning could be used for PCNL with a higher success rate than other positions.
Because of the complexity of the procedures, ECIRS is often considered to have a longer operative time than other procedures. 42 However, many studies report that ECIRS actually has a shorter operative time than PCNL. 43 In this study, we discovered that there were showed no significant differences of operative time in ECIRS compared with cPCNL (MD −4.29, 95% CI −34.66 to 26.08, p = 0.78), mPCNL (MD −15.69, 95% CI −47.82 to 16.43, p = 0.34), and both group combined (MD −10.93, 95% CI −28.97 to 7.10, p = 0.23). The discrepancy between the available reports is because of differences and a lack of standardization in the assessment of operative time. 44
The appropriate way to measure the operative time is to count from the beginning of retrograde access until the application of drainage instruments such as nephrostomy and catheter placement. In this review, Zhao et al. 22 and Kontos et al. 17 reported a shorter operative time in ECIRS compared with PCNL, but other studies measured the operative time from the initial patient positioning, which eventually leads to a longer operative time in ECIRS procedures. Several studies reported higher bleeding rates in PCNL compared with ECIRS. The bleeding occurs because of excessive movement of the nephroscope against the pelvicaliceal system as the efforts to reach the stone. 45
In performing PCNL, dilatation that is too minimal in the parenchymal tissue can cause bleeding as the needle must be retracted to perform redilatation. In contrast, excessive dilatation can also cause bleeding. 46 In this systematic review, we found no significant difference in Hb reduction in ECIRS compared with cPCNL (MD −0.65, 95% CI −1.91 to −0.61, p = 0.31), mPCNL (MD 0.13, 95% CI −0.20 to 0.45, p = 0.45), and overall PCNL (MD −0.08, 95% CI −0.31 to 0.14, p = 0.47) groups. However, this insignificant difference could be caused by the small number of studies with relatively small sample size. Several studies reported that less bleeding is caused by less percutaneous access in ECIRS. 18
However, studies reported that in the ECIRS procedure, massive bleeding can occur because of improper puncture technique and excessive twisting motion in extracting stones. These complications can be minimized with the experience of the operator. In addition, the difference in puncture size is not a factor in the severity of bleeding, whereas the 24F and 18F needle sizes had no difference in the bleeding rate. Circular motion with minimal rigid nephroscopy occurs in the ECIRS procedure that uses a flexible-type nephroscope to ensure a safe papillary puncture with minimal bleeding. 47,48 The transfusion rate of ECIRS was reported to be lower than PCNL in most studies, as shown in Table 2.
However, the indication for transfusion in each center could be different since transfusion practice between surgeons varies among studies. The worldwide implementation of transfusion protocols differs, with different degrees of success. Most global organizations recommend against blood transfusion in patients with >7 or 8 g/dL Hb levels. However, many centers still continue to do so, ignoring the evidence-based recommendations supporting the restrictive use of blood transfusion. 49 Moreover, the transfusion targets might also be different for each patient, ranging from 8.0 to 11.9 g/dL. 50 These differences generate a potential bias of relying on a small difference in the rate of transfusion between the procedures among the included studies.
The combined approach of ECIRS generated favorable results in the low rate of complications based on the Clavien–Dindo classification compared with the PCNL groups (OR 0.43, 95% CI 0.21–0.85, p = 0.02). The reported complications of ECIRS varied from 10% to 48%. 18,51 Infection is one of the most significant complications of PCNL, which commonly presents as postoperative fever (10.8%) and urosepsis (0.5%) that had a high mortality rate. 35,52 Various comorbidities such as diabetes, neurogenic bladder, renal abnormalities, multiple access, large stone size, long operating time, and high irrigation flow pressure increase the risk of postoperative infection. 6
High intrarenal pressure during irrigation in PCNL measures is also relevant in predicting the incidence of infection. Several previous studies have suggested that PCNL with a size of 30F should have optimal irrigation flow, but there are other factors that can increase intrarenal pressure such as the perpendicular position of the Amplatz sheath in the prone position or improper ratio of sheath to nephroscope. Several studies have also reported that the ratio between needle size and nephroscope diameter as a risk factor for infection. In addition, ECIRS is recommended for a lower incidence of infection because it can minimize the number of PCNL accesses, intrarenal pressure, and excessive irrigation flow. 53,54
The results of these studies are consistent with the results of this systematic review, which showed that the incidence of urosepsis in patients undergoing ECIRS was significantly lower compared with cPCNL (OR 0.14, 95% CI 0.02–0.78, p = 0.02), but not in mPCNL (OR 0.71, 95% CI 0.21–2.41, p = 0.56). Overall, the ECIRS procedure had a lower incidence of urosepsis compared with PCNL (OR 0.35, 95% CI 0.14–0.88, p = 0.03). The difference in the incidence of infection between the two types of PCNL might indicate the possibility of differences in complication rates because of differences in the PCNL needle size. 38
Technological advances and surgical approaches have evolved and changed the field of endourology, including ECIRS. One of the possible newer methods for lithotripsy in ECIRS is thulium fiber laser, which has been shown the be more efficacious compared with a holmium:YAG laser fiber as it is much smaller, thus able to create smaller fragments and dust particles. Tiny fragments can be flushed through the PCNL sheath or ureteral access sheath (UAS). 55 Based on the findings of this review, there are advantages of ECIRS over PCNL. Apart from the outcomes analyzed in this review, several studies suggest the ease of performing the procedure, including the avoidance of the need for multiple tracts and the improvement of helping decide the need for a ureteral stent or a second-stage procedure.
However, it is currently not more widely adopted because of the added cost and expertise required for handling two endoscopic mechanisms by experienced urologists. 56 In addition, there are disadvantages to the GMSV position, commonly used in ECIRS, aside from its known benefits. The hypermobility is caused by the supine position of the kidneys and respiratory movements; a renal puncture may be more difficult. The working space of the procedure is also more restricted compared with the prone position. These limitations hinder the wide adoption of ECIRS, especially among centers in developing countries where the aspect of cost becomes more apparent. 8
The technical aspect of ECIRS involves renal access and dilatation, which may involve UAS. The access allows fURS to identify and remove missed ureteral fragments. The use of a flexible nephroscope and UAS increases the cost of the procedure; however, it is not higher compared with a second or third procedure for clearing of the remaining fragments. Because of the insertion of UAS and a retrograde ureteroscopic procedure, long-term evaluation and observation for ureteral stenosis after ECIRS are necessary. 43 The presence of UAS influences intrapelvic pressure, in which a larger UAS in diameter is associated with a lower intrapelvic pressure (IPP). However, a large UAS diameter may be associated with ureteral lesions. 57
Most studies commonly used 12F/14F UAS. Increasing the diameter to 14F/16F generated an insignificant difference in the flows and IPP. 58 Several studies on ECIRS reported various UAS diameters from 10F/12F to 12F/14F. 59 The ideal size should be small enough to prevent ureteral injury, but big enough to maintain a low IPP. However, as of the conduction of this study, there are no data on IPP in ECIRS. 60
This systematic review and meta-analysis had several limitations. Several included studies had different patient positioning and lack of operative time standardization, which contribute to the significant heterogeneity. In addition, a limited number of studies that analyze bleeding parameters make the sample size relatively small. The lack of RCTs included also contributed to the results of this systematic review. In general, the results of this meta-analysis indicate that ECIRS is an effective and safe procedure, especially for large and complex renal stones, which allows anterograde and retrograde approaches with higher SFR results in one procedure with relatively low morbidity compared with PCNL.
There is currently no consensus regarding the method of evaluation for SFR, causing a variation in the imaging modalities used and time points for evaluation. Most studies used CT scan to evaluate SFR, whereas others used plain abdominal KUB and USG in some patients. To minimize the bias in evaluation time points, we analyzed the initial SFR as opposed to the final SFR. Nevertheless, a standard postoperative SFR evaluation should be determined for future studies. The addition of parameters in future studies, such as the difference in cost and length of stay between the two procedures, should also be the focus of the study. A significant cost differential could affect the feasibility of implementing this procedure in developing countries, such as Indonesia among many others.
Conclusion
This systematic review and meta-analysis showed that ECIRS is a safe and effective procedure for treating large and complex renal stones. It is superior to PCNL based on its higher one-step SFR, lower necessity for auxiliary procedures, and lower complication rate compared with PCNL.
Footnotes
Authors' Contributions
Data acquisition, analysis, interpretation, and drafting the article by D.R.W. Data acquisition, analysis, and interpretation by Y.P.K., F.H., and Z.A.R. Verification of data obtained, critically revising for important intellectual content by A.C.-F.N. and L.H.
Author Disclosure Statement
The authors have nothing to disclose.
Funding Information
No funding was received for this article.
Supplementary Material
Supplementary Figure S1
Supplementary Figure S2
Supplementary Table S1
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.