
Abstract
Objectives:
Larger ureteral access sheaths (UASs) have the potential to improve ureteroscopic stone removal outcomes but are often avoided by surgeons because of concerns of ureteral injury. Using our novel UAS force sensor and previously defined force thresholds for ureteral injury, we sought to evaluate the impact of 1 week of stenting on the maximum safe dilation of ureteral luminal circumference.
Methods:
Twelve juvenile female Yorkshire pigs (24 ureters) were evaluated. The inner (i.e., luminal) circumference of each ureter was determined using Cook urethral dilators ranging from 8F to 24F in 2F increments, 37 cm in length. Each dilator was sequentially passed while applying the UAS force sensor to measure insertion force before and after 1 week of stent placement. Each ureter was randomized to receive either a 4.7F or 7.0F stent (20 cm). Maximum ureteral luminal circumference was defined as effective passage of the dilator to the ureteropelvic junction with ≤6 newtons (N) of force (the force threshold previously defined by porcine and clinical studies to avoid ureteral damage). After passage of the largest dilator at 6 N, flexible ureteroscopy was performed and a post-ureteroscopic lesion scale (PULS) was recorded.
Results:
After 1 week of stent placement, the median ureteral luminal circumference increased to 15F representing a mean increase of 3.8F ± 2.8F (p < 0.001). Twenty-one (88%) of the pre-stented ureters had an increase in luminal circumference, with 12 ureters (50%) dilated to ≥16F (p = 0.032), 6 ureters (25%) dilated to ≥18F, and in 2 cases a maximum size of 24F was recorded. The PULS grade was ≤2 in all cases, indicating no high-grade ureteral injuries. Laterality and stent size did not impact ureteral luminal circumference after pre-stenting (p = 0.232 and p = 0.337, respectively).
Conclusions:
One week of ureteral stenting resulted in nearly a 4F increase in the luminal circumference of porcine ureters.
Introduction
Ureteroscopy has rapidly become the most common modality for treating ureteral and renal stones worldwide. 1 Accordingly, there is great interest in systems that could facilitate ureteroscopic stone removal, such as the ureteral access sheath (UAS). The UAS provides efficient repeated access to the renal collecting system as it protects the ureteral wall, provides a direct “conduit” to the renal pelvis, improves irrigation, and reduces intrarenal pressure. 2 To date, because of fear of potential ureteral injury, the consensus has been to use as small a UAS as possible; accordingly, most surgeons have limited themselves to deploying a 12F or 14F UAS. 3 However, recent studies have demonstrated that passage of a 16F UAS during ureteroscopy (URS) is of value as it provides for a greater reduction in intracaliceal pressure, better stone clearance rate, and significant decreases in operative times. 2,4
Ureteral tone is often cited as the limiting factor for UAS passage. Sequential ureteral dilators, balloon dilators, and stents have been tested as methods of expanding the ureter. 5 –7 The first two are passed at the time of URS and it is hypothesized that ureteral injury occurs from excessive insertion forces. In contrast, stents placed before a procedure have the distinct advantage of creating passive dilation. 8,9 In porcine models, which most closely duplicate the human urinary system, ureteral stents have been shown to result in aperistalsis and hence ureteral dilation within a 72-hour period. 10,11
Lim and colleagues demonstrated in a porcine model that the optimal pre-stenting period is 5 days. 10 Clinically, there remains great controversy surrounding the efficacy of pre-stenting, particularly with respect to stent morbidity, postoperative outcomes, and cost-effectiveness of a secondary procedure to place the stent. 12,13 Of note, past investigations have shown that when an initial attempt at URS fails because of ureteral spasm, placement of a ureteral stent for a week is invariably followed by a second attempt at URS. 14
In our prior porcine study with our novel UAS force sensor, we noted that limiting deployment forces to ≤6 newtons (N) resulted in no high-grade ureteral injury. 15 Also in our clinical studies, we noted that even without pre-stenting, we could place a 16F access sheath at ≤6 N in 39% of our patients, raising the question as to what would be the largest access sheath the ureter could accommodate, especially after stenting. 16 Armed with this knowledge, we sought to determine the maximal safe dilation of the porcine ureter before and after 1 week of stenting.
Methods
After Institutional Animal Care and Use Committee approval, under protocol AUP-19-171, 12 female juvenile Yorkshire pigs (weighing 30–45 kg) were included in the study. Before the procedure, each left ureter was randomized to receive a 4.7F or 7F stent and the remaining size stent was placed on the contralateral side. A single surgeon performed all the procedures. The pigs were administered intravenous sedation and then placed in a supine position.
A flexible cystoscope (Karl Storz, Tuttlingen, Germany) was inserted into the bladder. The left ureteral orifice was cannulated with a 0.889 mm super stiff guidewire, which was then advanced into the renal pelvis. Next, a 5F open-ended ureteral catheter was advanced over the guidewire; the guidewire was removed, and a retrograde pyelogram was performed. The guidewire was then replaced. Cook urethral dilators (ranging from 8F to 24F, 37 cm in length) (Cook Medical, Inc., Bloomington, IN) in 2F increments were passed with the UCI purpose-built UAS force sensor (Fig. 1) until either they reached the renal pelvis or 6 N was recorded.
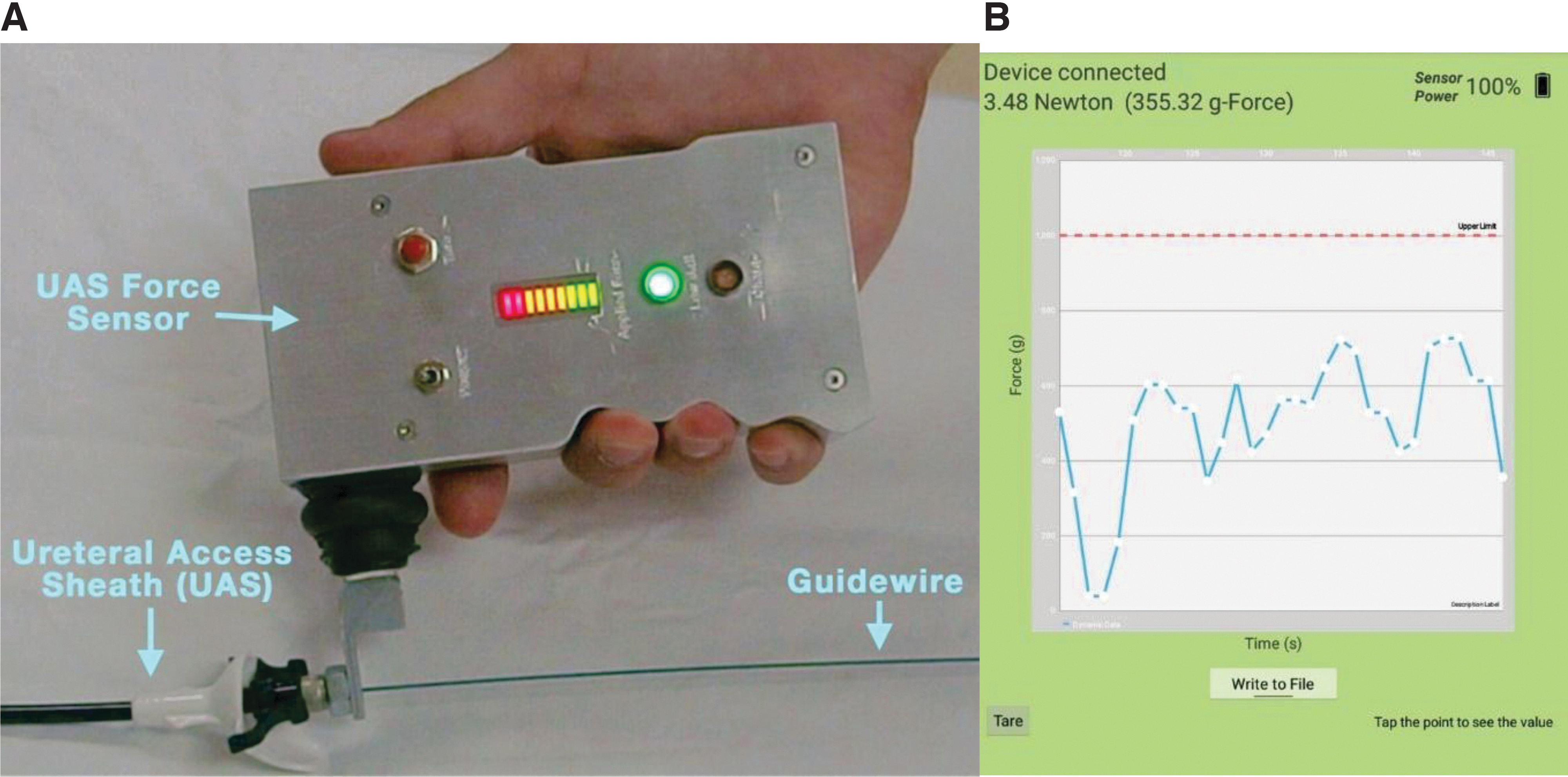
In the latter circumstance, the location of peak force (distal, mid, or proximal ureter) was recorded. Maximum ureteral luminal circumference was defined as effective passage of the dilator to the ureteropelvic junction at ≤6 N of force. After dilation, flexible URS (Karl Storz) was performed to evaluate the ureter throughout its entire length and a post-ureteroscopic lesion scale (PULS) grade (Table 1) was assigned based on consensus of two surgeons. 17 Next a 20 cm ureteral stent (either 4.7F or 7F, size previously randomized) was placed under fluoroscopic guidance. This procedure was then repeated on the contralateral side.
Post-Ureteroscope Lesion Scale 17
URS = ureteroscopy.
After 1 week of stenting, the pig was sedated. The stents were removed, and the aforementioned dilation procedure was repeated. The maximum size dilator that was passed to the UPJ at ≤6 N of force was recorded.
Shapiro–Wilk test was used to assess normality of continuous variables. Normally distributed continuous data were analyzed using Student's t-test, otherwise Wilcoxon rank sum test was used. Chi-square tests were used to compare categorical variables. All statistical analysis was performed using SPSS version 24 (IBM, Armonk NY) and a p-value <0.05 indicated statistical significance.
Results
A total of 24 ureters were included in the analysis. After 1 week of stent placement, the median ureteral luminal circumference increased to 15F representing a mean increase of 3.8F ± 2.8F (p < 0.001) After pre-stenting, 21 ureters (88%) increased in size. The location of failure was not significantly different pre-stent vs post-stent (p = 0.323), with distal ureter being the most common site of resistance before stenting and the proximal ureter being the most common site after stenting.
After 1 week of stenting, 12 ureters (50%) dilated to at least 16F (p = 0.032), 6 ureters (25%) dilated to 18F, and in 2 cases a maximum size of 24F was recorded (Table 2). Figure 2 shows the overall distribution of effective dilator passage (≤6 N) at each size. Of note, in 96% of ureters, adhering to a force of ≤6 N, resulted in a PULS score of 0 to 1; there was only one ureter that was a PULS 2 and in no case was a high-grade (PULS 3–5) injury sustained. On subgroup analyses, there were no differences in ureteral luminal circumference with regard to laterality or stent size (p = 0.232 and p = 0.337, respectively) (Tables 3 and 4).
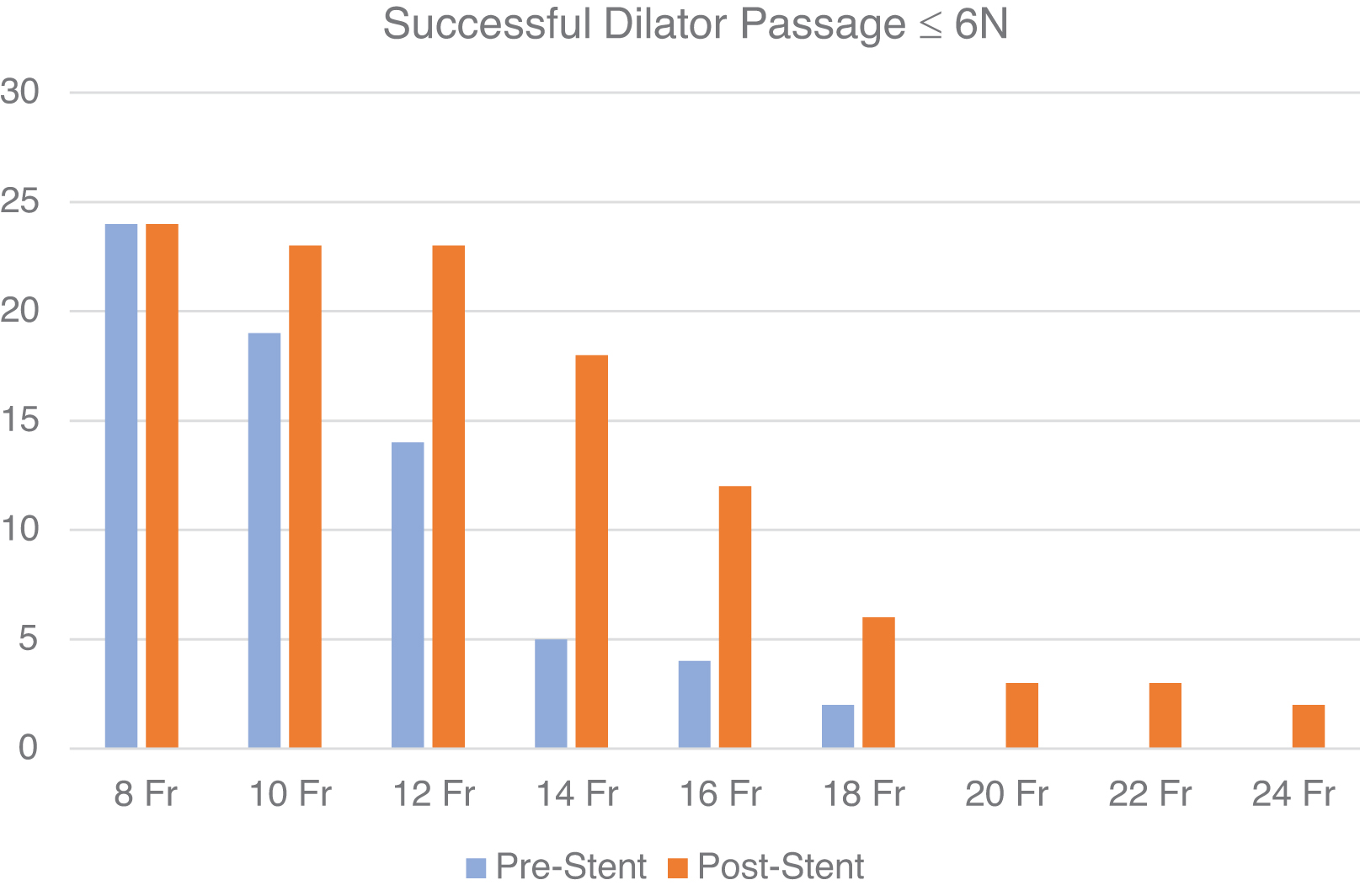
Overall distribution of successful dilator passages (≤6 N of force) pre- and post-stenting in 24 ureters.
Comparison of Ureteral Luminal Circumference Pre- and Post-stent Placement
Bold represents statistically significant p<0.05.
PULS = post-ureteroscopic lesion scale; SD = standard deviation.
Subanalysis of the Impact of Laterality on Ureteral Luminal Circumference Pre- and Post-stent Placement
Subanalysis of the Impact of Stent Size on Ureteral Luminal Circumference Pre- and Post-stent Placement
Discussion
The benefits of using an UAS to facilitate ureteroscopic stone removal include reduced intrarenal pressure, improved visibility, and higher levels of stone clearance. 2,18,19 Nonetheless, some urologists around the globe have continued to shy away from using UAS because of concerns of ureteral damage and possible, although rare, ureteral stricture formation. In this regard, recent studies reported by experienced endourologists recorded high-grade ureteral injuries in 26% to 47% of patients. 20,21 Of interest, the risk of ureteral injury decreased sevenfold when patients were pre-stented.
In a prospective study by Stern and colleagues of 56 patients with UAS-induced ureteral injuries (36 with grade 2 and 18 with grade 3) from deployment of a 14F UAS, only 1 patient developed a ureteral stricture (1.8%). 22 Further corroborating the low rate of UAS associated strictures is the retrospective study by Shvero and colleagues; among 165 unstented patients undergoing URS, there was no ureteral stricture formation regardless of the size of UAS deployed. 23
Based on CT scans, the mean ureteral circumference is 13F (4.3 mm), with the narrowest point being at the ureterovesical junction (5F or 1.7 mm). 24,25 Given the similarity between the porcine and human ureter, it is not surprising that our study noted the most common location of failure was the distal ureter before stenting. However, after 1 week of stenting, the location of failure moved to the proximal ureter. This remains a mere observation as the differences did not reach statistical significance. Of note, in practice today, the most commonly used UAS is 11F; however, in prior studies, stone-free rate has been demonstrated to be higher among patients who had a larger UAS deployed. 26,27
Currently, the largest commercially available UAS is 16F with a 14F luminal circumference. We demonstrated that after 1 week of pre-stenting, the ureteral luminal circumference increases an average of nearly 4F. Furthermore, this is the first report to note that after pre-stenting 25% of porcine ureters accepted a ≥ 18F dilator, with a maximum of 24F; notably these hitherto unreported larger sizes are on par with currently deployed mini-PCNL sheaths.
In a study by Yuk and colleagues, they demonstrated that pre-stenting allowed for an increase in the success rate of UAS placement from 85.3% to 93.8% (p = 0.023) while simultaneously showing that the UAS size in the pre-stented group was larger than controls. 28 Similarly, a prospective small (n = 7 patients) study by Tefik and colleagues showed that pre-stenting before retrograde intrarenal surgery allowed for larger UAS size sheaths (i.e., 14F) to be advanced compared to nonstented patients who accepted only 11.5F and 12F UASs. 29 Sung and Cho in their retrospective case study analyzed 122 patients in which 73 patients had preoperative stenting performed; the pre-stented group had a success rate of 97.3% for UAS insertion vs 87.8% for the control group. 30
By employing our previously described UAS force sensor, we were able to have real-time measurements of the force exerted on the ureter while passing an UAS. Our porcine and extensive clinical studies corroborated that forces up to 6 N are well tolerated and thereby preclude high-grade ureteral injury. 15,16 As such we sought to not only test the degree to which the ureter might enlarge as corroborated in earlier studies, but also to learn, for the first time, whether a pre-stented ureter might be capable of accepting even larger access sheaths than the UAS currently available; specifically UAS (i.e., 18F–24F) that would actually rival the sheath size used for mini-PCNL.
Overall, among 24 porcine ureters, we noted an increase in ureteral luminal size in 88%. Furthermore, we noted that in 25% of cases, the ureter could safely accept an ≥18F dilator and in two (8%) cases a maximum luminal size of 24F was recorded. Accordingly, it is our belief that access sheaths at 18F or even larger could be safely passed into the human ureter with the benefits being all those of a percutaneous stone removal (PCNL) without the risks of hemorrhage or perirenal organ damage.
This expansion of natural orifice surgery would in theory empower urologists with the ability to safely remove even staghorn stones in an outpatient minimally invasive manner. Presently we are pursuing the creation of 18F, 20F, 22F, and 24F UASs with the belief that as long as the force of insertion is kept below 6 N, they can be safely deployed with no damage to the ureter. With the addition of these sheaths to the urologists' armamentarium the high stone-free rates associated with PCNL could one day be achieved without incurring the morbidity of percutaneous renal access.
Our study is not without limitations. Although the porcine urinary system is quite similar to the human urinary system, the results may not directly translate at a clinical level. Nonetheless, we have noted that the 6 N limit defined in our earlier porcine studies was duplicated in our clinical study. 15 Although PULS grading can be subjective, we further correlated the subjective visual findings with objective force measurements. Furthermore, in this study, we did not have a true control group in which sequential sizing would have been performed in unstented pigs a week after the initial ureteral sizing.
The reason this was omitted was because of concerns over ureteral edema and potential complications of leaving an unstented system after passage of the aforementioned dilators up to 6 N. Also, the dilators used in this study only came in 2F increments. It is foreseeable that finer calibration with 1F increment would provide more accurate results. Finally, the urethral dilators we used lack the lubricious hydrophilic coating of the UASs; hence, our study may have underestimated the maximum ureteral luminal circumference in the pre-stented ureter.
Conclusion
One week of ureteral stenting resulted in a nearly 4F (1.33 mm) increase in the luminal circumference (diameter) of porcine ureters. Laterality and stent size did not impact the degree of ureteral enlargement.
Footnotes
Authors' Contributions
The authors confirm contribution to the article as follows: study conception and design by P.J., R.M.P., J.L., and R.V.C.; data collection by P.J., A.A., A.B., A.P., T.K., S.D., M.A., K.L., and H.S.; analysis and interpretation of results by P.J., L.L., and R.V.C.; draft article preparation by P.J., A.A., R.M.P., J.L., and R.V.C. All authors reviewed the results and approved the final version of the article.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No external funding was used.