
Abstract
Purpose:
Analyze the impact of tranexamic acid (TXA) use after percutaneous nephrolithotomy (PCNL) on blood loss and transfusion rate (TR), and secondary outcomes, complications rate and stone-free rates (SFRs), operative time (OT), and length of hospital stay (LOS).
Materials and Methods:
Search made in the Medline (PubMed), Embase, and Central Cochrane for studies published up to August 2021. The study protocol was registered at prospective register of ongoing systematic reviews (CRD42020182197). Eligibility criteria were defined based on Patient, Intervention, Comparison, Outcomes, Study Design acronym (PICOS). Articles included were those who assessed the effect of intravenous TXA in patients submitted to percutaneous nephrolithotripsy (PCNL). Only randomized placebo-controlled trial that included patients with and without TXA perioperatively.
Results:
A total of 1151 patients were included in seven studies. Six studies presented a lower blood TR for the TXA group (p < 0.00001). Four studies presented similar results in relationship to a lower SFRs (p = 0.004) and similar results regarding overall complication rate for the control group (p = 0.03). Regarding the “major complication rate” (Clavien-Dindo ≥3), no difference was found (p = 0.07). Four studies showed a higher mean OT for the control group (159 × 151 minutes, respectively, p = 0.003). Six studies found a lower mean LOS in the TXA group (4.0 × 3.5 days, respectively, p = 0.03).
Conclusions:
The benefit of TXA use in the setting of PCNL perioperatively is clear. Our study showed favorable results to TXA use in relationship to TR, SFR, complication rate, OT, and LOS, but these results did not translate into a lower major complication rate. Further studies evaluating the complexity of the calculi and events unrelated to PCNL may help us select which patients will benefit from the use of TXA.
Introduction
Recent evidence has shown an increase in urinary lithiasis incidence. Epidemiologic reports pointed to a prevalence rate of 8.8% in the general population and a 5-year recurrence rate of 50% in those who presented first renal colic episode. 1 –5 First described by Fernström and Johansson in 1976, 6 percutaneous nephrolithotomy (PCNL) is the first-line approach for large stones (>2 cm) and staghorn calculi. 7,8 This procedure has a superior stone-free rate (SFR) and its cost-effectiveness compared to other endourologic procedures and lower morbidity profile than open surgery. 9 PCNL is a well-known minimally invasive procedure related to not negligible morbidities, such as perioperative fever, collecting system perforation, adjacent organ injury, and severe bleeding. 10 –13
Hemorrhagic events are not infrequent in PCNL, and the transfusion rate (TR) range from 1% to 12%, with 1.5% requiring renal angioembolization to control bleeding. 14 Severe hemorrhage presents a challenge to the hemostatic system, and preventing blood loss in elective surgeries must be paramount. Fibrinolysis surges as an important factor acting on hemostatic control by clots breakdown. However, severe bleeding might lead to a hyperfibrinolysis state and, consequently, a pathologic scenario, worsening the bleeding. 15 Antifibrinolytic agents can be helpful to control fibrinolysis, in a normal and pathologic state, to reduce blood loss in the perioperative setting. Tranexamic acid (TXA), a synthetic derivative from lysine amino acid, inhibits fibrinolysis by preventing plasminogen binding sites on fibrin stands, intermediated on lysine residues enzymatically removed by the drug. 16
A large, multicentric, randomized placebo-controlled trial [randomized clinical trial (RCT)] evaluated the use of TXA in trauma victims. This trial showed a significant reduction in all-cause mortality and a reduced risk of death due to bleeding on trauma patients who received the TXA. 17
A systematic review and metanalysis was performed to assess the impact of TXA use after PCNL on blood loss and TR, secondary outcomes, complication rate, SFRs, operative time (OT), and length of hospital stay (LOS).
Materials and Methods
Protocol and registration
The study's protocol was approved by all authors and was registered in the international prospective register of ongoing systematic reviews registration number: CRD42020182197, according to Preferred Reporting Items for Systematic Reviews and Meta-analysis (PRISMA) statement. 18
Eligibility criteria
Clinical questions were formulated in the Population, Intervention, Comparator, and Outcomes format. 18 The articles included in the systematic review were those that compared the effect of intravenous TXA to placebo or usual care in adults patients submitted to PCNL. Studies in which the first dose of TXA (before the start of the procedure) was administered by a route other than intravenous (such as orally or by irrigation of the collection route) were excluded, as the time of action of the substance may impact its effect in preventing bleeding. Only RCT, which included patients with (TXA group) and without TXA (control group) perioperatively were included in the analysis. The primary outcome evaluated was TR. The secondary outcomes were bleeding based on SFR, complication rate according to Clavien-Dindo (CD) classification, OT, and LOS.
Studies presenting incomplete data, such as mean without standard deviation (SD) and noncomparable unit measurable, were excluded. Studies that use TXA in different access other than intravenous use, such as intrarenal irrigation, were excluded. The most recent and complete data only were considered for studies, including the same population.
Information sources
The search was performed using Medline (PubMed), Embase, and Central Cochrane for studies published up to August 2021. Articles in English, Spanish, French, or Portuguese were identified through a computerized blinded search. A gray search was performed based on the references of included studies.
Search, study selection, and data collection process
The following search strategy was used for each database: Percutaneous Nephrolithotom* AND (Tranexamic Acid OR Antifibrinolytic Agents). According to the PRISMA statement, the studies found in each database were filtered by the “Titles/Abstract” category by two authors, using a data table developed for this purpose. 18 In case of discrepancies, a third author solved this issue, or the full text was evaluated by the authors. All cross-referenced studies from the retrieved articles were screened for pertinent information.
Data items
Three authors extracted the following information from each included study: population characteristics (age, gender, and mean stone surface area); data regarding nephrolithotomy (site of renal access, use and type of urinary diversion at the end of procedure [none, nephrostomy tube alone, Double-J stent alone, or both]); description of TXA use in the experimental group (dosage, frequency, and duration); data regarding outcomes (TR, SFR, total and major complication rate, mean OT, mean LOS); and the number of patients included and in the last follow-up.
Risk of bias assessment
The risk of bias for the included studies is related to variations inherent to each surgery performed. These variations might be related to patients characteristics (such as age, body mass index, and comorbidities), to disease complexity (such as stone surface area and staghorn calculi), to surgery technique (such as patient position [prona, supine, or both], number of punctures, site of access, size of dilation, and type of lithotripter), and to description of intervention—TXA use. In addition, the risk of bias is related to how the studies reported the outcomes. First, if they accurately defined the outcome, second if they reported even the nonoccurrence of events, and finally when they assessed the outcome.
The included studies were assessed with regard to protocol registration, and all the studies were RCT. Finally, two authors applied the Cochrane Risk-of-Bias Tool for RCT.
Data synthesis and analysis
Continuous variables are presented as mean ± SD, and its comparison was performed using the inverse variance statistical method. While dichotomous variables were presented as rate (%) based on risk difference (RD), effect measure and its comparison were performed using the Mantel-Haenszel statistical method. Studies that presented their results with median and confidence interval (CI), were converted to mean and SD. The results summary was graphically presented as a forest plot. Significant heterogeneity was stated as I2 ≥ 50%. Random effects models were used for results in that case; otherwise, fixed-effects models were used. Review Manager version 5.4 (The Cochrane Collaboration, London, England, United Kingdom) was used to run the analysis considering a threshold of p < 0.05 as significant.
Results
Study selection and characteristics
Seven studies were included in the final analysis. The study selection flowchart is shown in Figure 1. The characteristics of the included studies are exposed in Tables 1 and 2
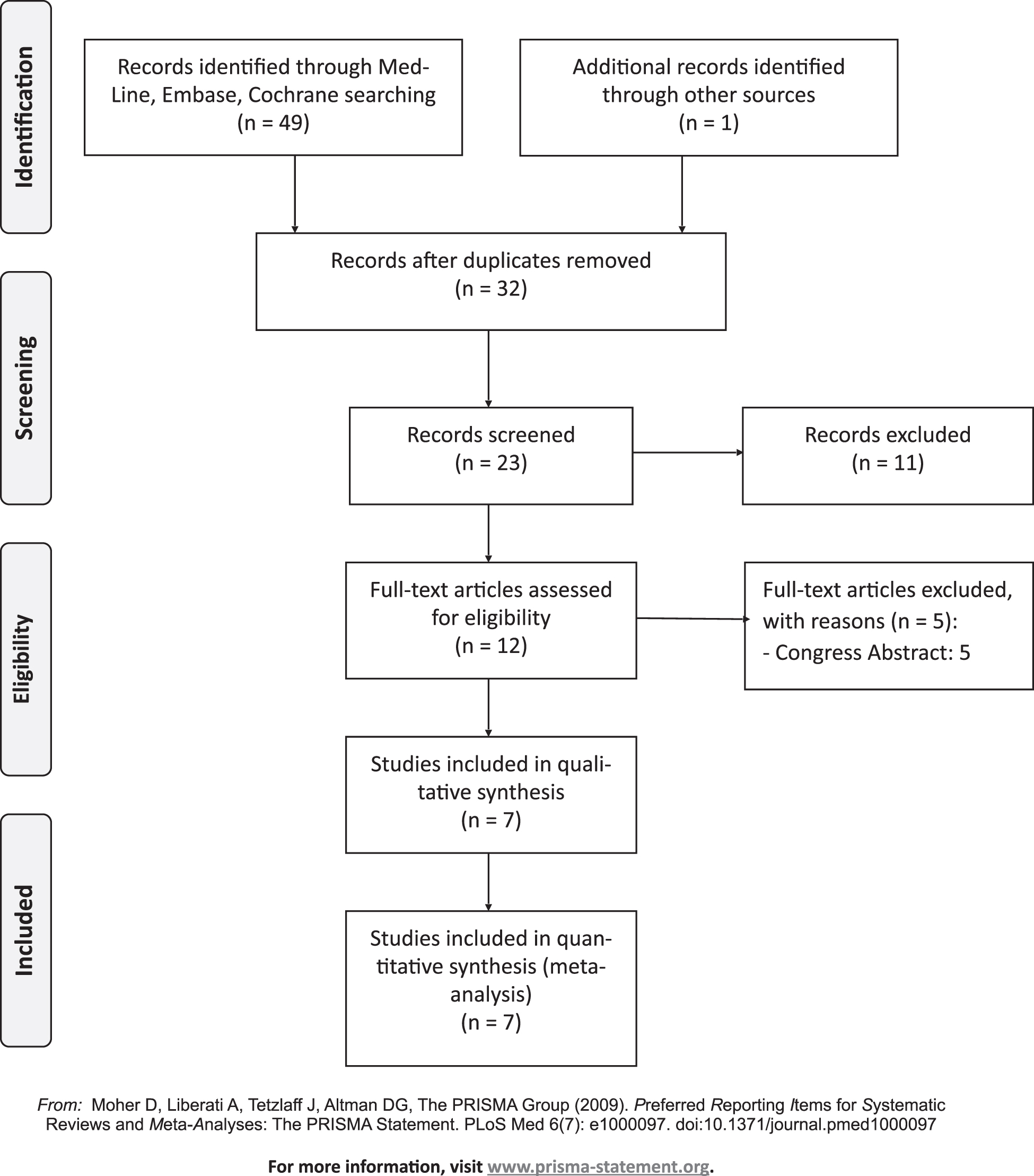
Flow diagram of study selection.
Basic Characteristics and Data of Included Studies
Stone size <4 cm.
Stone size >4 cm.
C = comparison; CR = complication rate; I = intervention; IQR = interquartile range; IV = intravenous; LOS = length of hospital stay; MR = major complication rate; OT = operative time; PC = prospective cohort; RCT = randomized clinical trial; SD = standard deviation; SFR = stone-free rate; TXA = tranexamic acid; TR = transfusion rate.
Characteristics Related to Percutaneous Nephrolithotomy
CS = can't say.
Risk of bias assessment
The characteristics regarding the PCNL technique are shown in Table 2. Two studies did not report the patient's position during PCNL. 19,20 Three studies did not report the site of access and number of punctures. 19,21,22 Two studies did not report the size of dilation. 19,22 Two studies did not report the type of lithotripter. 19,22 Also, Batagello et al. used ultrasonic lithotripter, while four other studies used pneumatic lithotripter. 20,21,23 –25
Mohammadi et al. did not describe the schedule of TXA administration postoperatively. 19 Three studies presented its protocol registration at the Iranian Registry of Clinical Trials, but all three studies were registered retrospectively after its last follow-up. 19,21,22 Mohammadi et al. 21 presented their sample size calculation in an incomplete way, which turns its replication impossible. The risk of bias across studies is presented in Supplementary Appendix Figures SA1 and SA2.
Synthesis of results
Blood TR
Six studies with a total of 1031 patients presented a higher blood TR for the control group compared to the TXA group (11.4% × 3.7%, respectively; RD −0.08; 95% CI −0.11 to −0.04; p < 0.00001; I 2 = 0%) 20 –25 (Fig. 2). One study, Mohammadi et al., 19 did not present blood TR, only in the mean blood transfusion volume, however, no difference was found between groups.

Forest plot—comparison between TXA group and control group in relationship to blood transfusion rate. TXA = tranexamic acid.
Stone-free rate
Four studies with a total of 683 patients presented a lower SFR for the control group in comparison to the TXA group (70.6% × 79.6%, respectively; RD 0.09; 95% CI 0.03–0.15; p = 0.004; I 2 = 5%) 20,21,23,24 (Fig. 3). One study, Mohammadi et al., 21 showed a total SFR of 95%, but they mentioned that 10 patients (7.6%) required retreatment. This leads us to question what the authors stated as “stone free,” if it was based on one or >1 intervention.
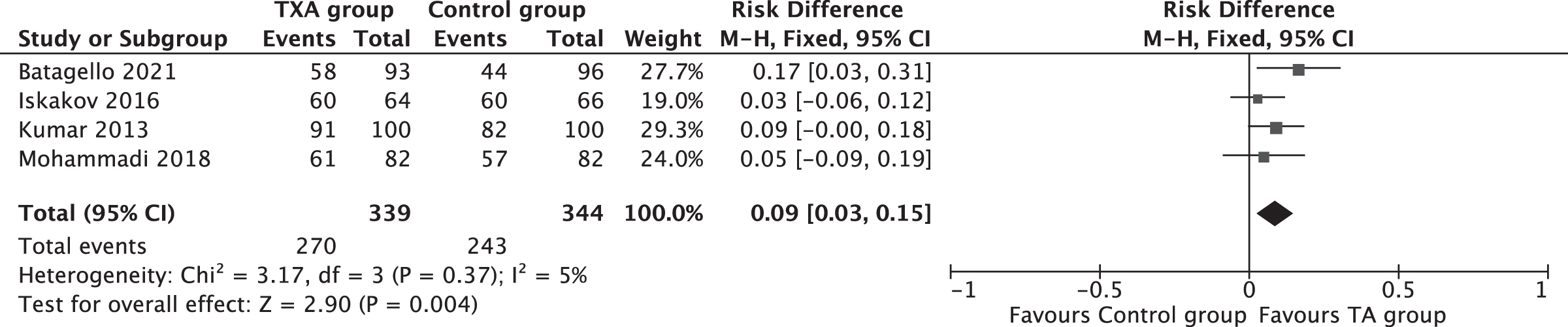
Forest plot—comparison between TXA group and control group in relationship to stone-free rate.
Complication rate and Safety
Four studies (683 patients) presented a higher complication rate in the control group compared to the TXA group (48.3% × 36.0%, respectively; RD −0.11; 95% CI −0.21 to −0.01; p = 0.03; I 2 = 59%) 20,21,23,24 (Fig. 4).
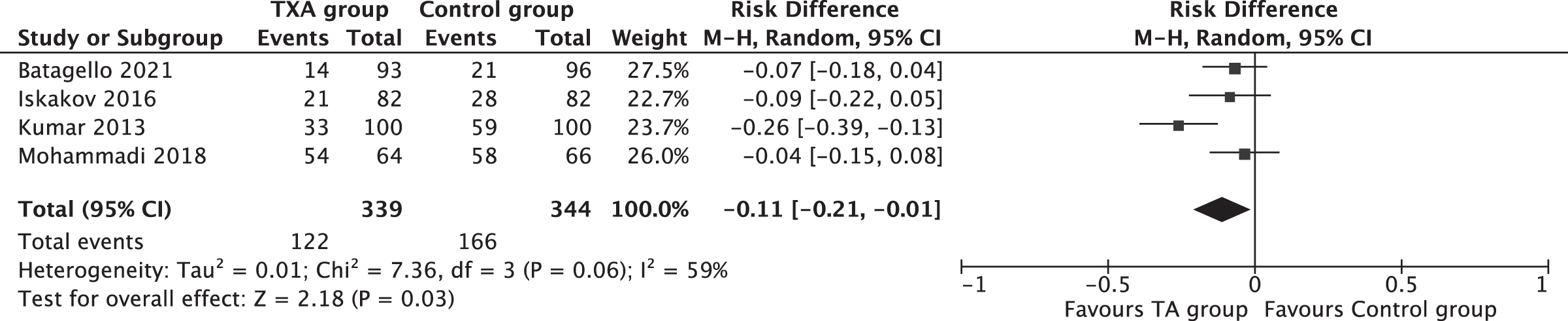
Forest plot—comparison between TXA group and control group in relationship to complication rate.
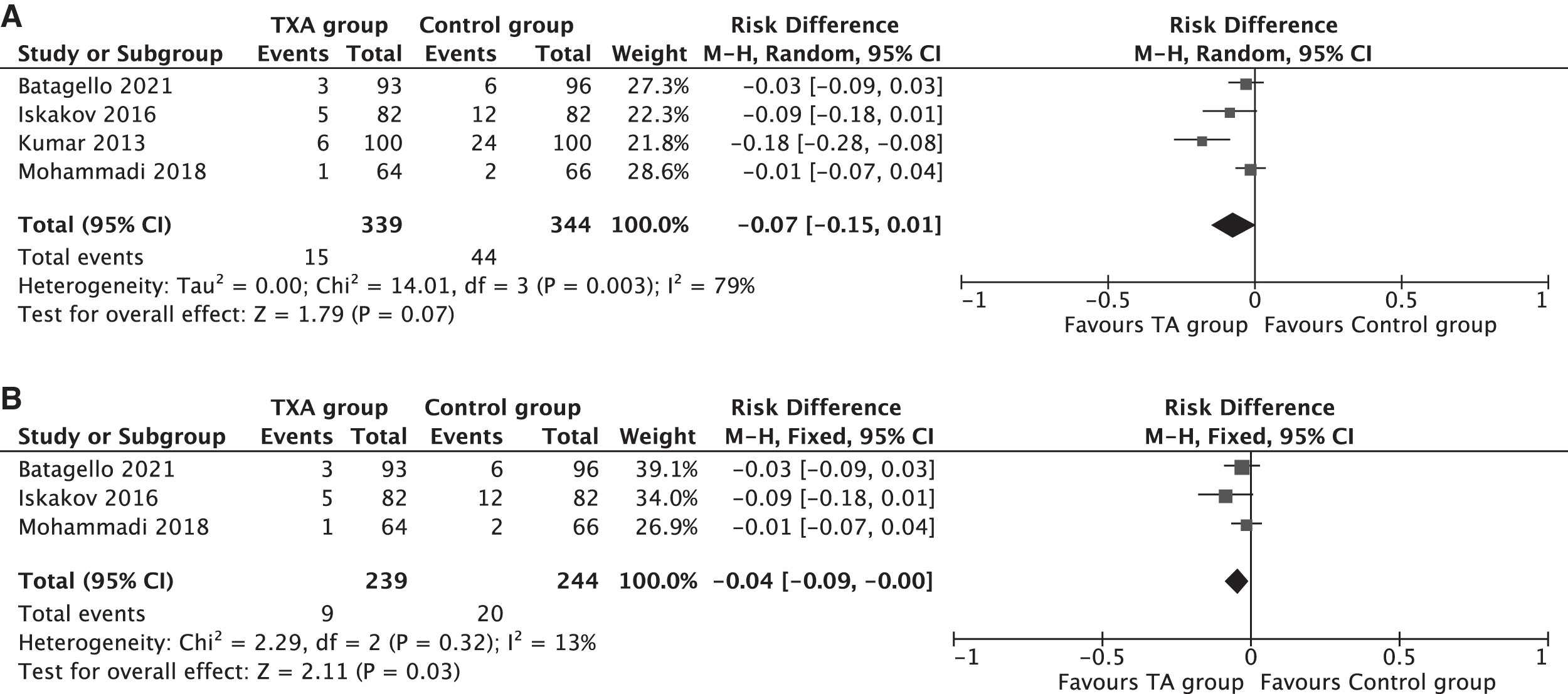
In relationship to “major complication rate” (CD ≥3), four studies (683 patients) found no difference between control and TXA groups (12.8% × 4.4%, respectively; RD −0.07; 95% CI −0.15 to 0.01; p = 0.07; I 2 = 79%) 20,21,23,24 (Fig. 5A). After exclusion of one study responsible for the high heterogeneity in the “major complication rate” analysis, 24 three studies (483 patients) found a higher CD ≥3 rate in the control group compared to the TXA group (8.2% × 3.8%, respectively; RD −0.04; 95% CI −0.09 to 0.00; p = 0.04; I 2 = 13%) 20,21,23 (Fig. 5B). One study, Kumar et al., 24 did not use a validated classification to evaluate its complications (such as CD classification). For instance, the authors considered blood transfusion as a “major complication,” which confronts the definition stated by CD. In addition, the authors considered moderate and severe hematuria as a “major complication” without any definition of these events.
The major complication related to bleeding after PCNL reported by the included studies were bleeding requiring angiographic embolization, hematoma requiring surgical drainage, perirenal abscess caused by hematoma requiring drainage, and bleeding requiring nephrectomy. Iskakov et al. and Kumar et al. reported one (1.2%) and three (3.0%) patients with bleeding requiring angiographic embolization, all patients in the control group. 20,24 Iskakov et al. reported one patient in the control group with arteriovenous (AV) fistula submitted to an attempt of angiographic embolization and the following nephrectomy. The same patient required a second procedure to drainage an abscess. Also, the authors reported another patient in the control group with a hematoma requiring surgical drainage. 24
Only two studies reported complications related to TXA use. Batagello et al. and Kumar et al. reported one (1.1%) and two patients (2.0%) with clot obstruction in the TXA group, respectively. 20,23 Batagello et al. reported two patients (2.2%) with symptomatic pulmonary embolism (PE) in the TXA group. These events were related to TXA use, as both patients were at high risk of thromboembolic events. In addition, the authors assessed the occurrence of deep vein thrombosis (DVT), myocardial infarction, and stroke. None of these events occurred in either group. 23
OT and LOS
Four studies enrolling 591 patients showed a higher mean OT for the control group in comparison to the TXA group (159 × 151 minutes, respectively; RD −12.31; 95% CI −13.91 to −10.70; p = 0.003; I 2 = 0%) 20 –23 (Fig. 6). One study, Kumar et al., 24 did not present its results with SD.

Forest plot—comparison between TXA group and control group in relationship to operative time.
Six studies with a total of 1031 patients found a higher mean LOS in the control group compared to the TXA group (4.0 × 3.5 days, respectively; RD −0.53; 95% CI −1.01 to −0.06; p = 0.03; I 2 = 96%) 19 –24 (Fig. 7).

Forest plot—comparison between TXA group and control group in relationship to length of hospital stay.
Discussion
PCNL is the gold standard to treat renal stones larger than 2 cm. 7,8 However, PCNL is related to a not insignificant rate of severe complications such as collecting system perforation, adjacent organs injury, and bleeding with transfusion requirement. 10 –13 The incidence of hemorrhagic events associated to PCNL, which requires blood transfusion, is 7%. These cases have a propensity to intensity care unit admission, arterial embolization, to increase the risk of needing a second procedure. 26 –28 Despite some improvements in armamentarium arsenal field, such as less traumatic dilator instruments, high-definition optical devices, miniaturized techniques, and hemostatic glues, bleeding still is an issue related to PCNL. Accordingly, some studies have evaluated the use of TXA in the perioperative setting of endourologic procedures, such as transurethral resection of prostate and PCNL. 29
Our meta-analysis found favorable results to TXA group regarding TR, complication rate, SFR, as well as LOS. The OT was lower in the TXA group, but even though the difference was statistically significant, there were no clinical benefit as the difference was only 7 minutes in favor of the TXA group. Major complication rate was similar between groups. Blood transfusion related to PCNL has some indications such as hemodynamic instability, laboratory alteration, and visual severe blood loss. Notwithstanding, this is at the discretion of the medical team without any specific protocol among included studies. However, the TXA use presented as an interesting alternative to complications related to PCNL, specifically bleeding.
Wang et al. reported a meta-analysis and selected six RCT to evaluate the need of blood transfusion as primary outcome. 30 It is important to highlight that two of the six included RCT are conference abstracts and was not published at the time this review was performed. Therefore, the authors assessed the risk of bias applying by Jadad score without access to all information about the methods of these two conference abstracts. Comparing the present study to this previous systematic review, two published studies were added and a proper bias analysis was made. In addition, the present study showed more data with regard to the outcomes assessed.
A prospective study analyzed 301 patients undergoing PCNL found that diabetes, multiple renal punctures, prolonged OT, and intraoperative complications rate were related to an increased risk of blood loss after the procedure. 31 El-Nahas et al. 27 evaluating 3878 PCNL showed that single kidney, upper pole puncture, large stones, and multiple renal tracts were related to bleeding after the procedure. TR was 5.5%, and angioembolization was required in only 1% of cases. Among the studies included in our meta-analysis, only one found no difference between the groups in terms of bleeding. However, the authors did not present the characteristics related to the complexity of the procedure, such as access site.
In addition, a minority of patients had staghorn stones that may mitigate the benefit of using TXA. At the same time, another study found that stones >4 cm had less bleeding in the TXA group, which leads us to better results with TXA in patients with more complex stones 19,21 (Table 2).
Renal upper pole is surrounded by an extensive vascularization, including segmental arteries, which demands meticulous attention during renal puncture and tract dilation. 32 Our meta-analysis included three studies which presented data regarding renal puncture site. 20,24,25 Upper pole puncture was necessary in TXA and control group in 47.5% × 49.2% (p = 0.44), 5% × 4% (p = 0.99), and 18.3% × 34.1% (p > 0.05), respectively, in these three studies. Only two studies presented data related to number of renal punctures. 21,24
TXA and control group were submitted to multiple renal punctures in 16.7% × 20% (p = 0.50) and 42.2% × 30.3% (p = 0.20), respectively, in these two studies. Considering the exposed, further trials may look to patient stratification regarding stone position and complexity. A more criteria patient selection might lead to identify the best scenario to the TXA use, which it is probably in the setting of patients who require complex procedures.
In contrast, only two studies assessed the safety related to TXA use. Batagello et al. and Kumar et al. reported one (1.1%) and two patients (2.0%) with clot obstruction in the TXA group, respectively. 20,23 Batagello et al. reported two patients (2.2%) with symptomatic PE in the TXA group. These events were related to TXA use, as both patients were at high risk of thromboembolic events. In addition, the authors assessed the occurrence of DVT, myocardial infarction, and stroke. None of these events occurred in either group. 23 However, the incidence of these events is lower in relationship to the benefit acquired with TXA in preventing bleeding, and further studies, including patients who are candidates for more complex procedures, may clarify our results. Furthermore, additional studies that assess other potential events, such as cardiac, allergic reactions, and thrombotic events are needed to assist in the indication of TXA.
Our study has some limitations. First of all, the high heterogeneity among some of the outcomes assessed, such as complication rate, OT, and LOS; in any case, the TXA use is still in its infancy and future studies may select more homogeneous patients who will benefit from the TXA use. In addition, in most included studies, the authors did not state the stone complexity as well as mentioned about the number of access tract performed in the procedure. This might play a role in hemorrhagic episodes, as well as another complication, but in summary the outcomes were better in almost all analysis, except for major complications, in which there was no difference between groups. Finally, there was a lack of standardization in TXA posology, which may have underestimated the difference between the groups, especially in relationship to major complication rate. However, all studies used TXA at the beginning of the procedure, which is the most important moment to avoid bleeding and, consequently, improve the other outcomes.
Conclusion
The benefit of TXA use in the setting of PCNL perioperative is clear. Our study showed favorable results to TXA use in relationship to TR, SFR, complication rate, OT, and LOS, but these results did not translate into a lower major complication rate. Further studies evaluating the complexity of the calculi and events unrelated to PCNL may help us to select which patients will benefit from the use of TXA.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.
Supplementary Material
Supplementary Appendix Figure SA1
Supplementary Appendix Figure SA2
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.