
Abstract
Introduction:
Active surveillance (AS) is a treatment strategy for low-risk prostate cancer (PCa) patients, with extended indication to some intermediate-risk PCa. However, active treatment is necessary in case of disease progression and robotic radical prostatectomy (RALP) is one of the treatment modalities. The aim of the study is to compare outcomes of a delayed RALP after an initial heterogeneous surveillance strategy with those of immediate RALP in a single referral center.
Methods:
Data from patients who underwent RALP after initial assumed “active surveillance” (referred from different institutions and backgrounds) were compared to those of patients who underwent an immediate RALP after propensity score (PS) matching. The PS analysis was performed matching ISUP score at the time of entering surveillance with ISUP at RALP for the control group; other matching covariates at the time of surgery were considered (including age, prostate-specific antigen, body mass index, prostate size, cT, pre-op Sexual Health Inventory for Men, etc.). Perioperative, functional, and oncological outcomes were compared between groups.
Results:
Three hundred sixty-two RALP patients were included (181 after surveillance and 181 immediate RALP). Patients after surveillance had a worse pT and ISUP score (p < 0.001); LVI and EPE were higher in the surveilled group (13% vs. 5%, p = 0.001; 38% vs. 22%, p = 0.001), without significant difference in positive surgical margin. At a median follow-up of 24 months, the risk of biochemical recurrence (BCR) was significantly higher for delayed RALP (hazard ratio: 4.0; 95% confidence interval: 1.4–12; p = 0.013), whereas potency and continence rate did not differ significantly.
Conclusions:
At a referral center receiving patients from diverse backgrounds, outcomes of RALP after heterogeneous surveillance strategies are variable and less predictable, maybe attributable to different protocols and surgical planning. The higher BCR rate in a high-risk surveilled cohort may suggest an increased burden of cancer-related care for RALP patients after surveillance.
Introduction
Active surveillance (AS) represents the standard of care for patients with low-risk prostate cancer (PCa): it aims to minimize treatment-related toxicity without compromising survival. The 2021 EAU Guidelines strongly recommend to offer AS to patients with a life expectancy exceeding 10 years, and such a strategy has been increasingly used during the last decade. 1,2 More recently, indications to AS have been extended also to intermediate ISUP 2 with favorable characteristics. 1 The use of AS is continuously gaining attraction in the urological community: a recent survey on 225 urologists from the United States found that 99% recommended AS to all their low-risk patients and the majority believed that AS is effective (97%). 3
AS has been proven to be safe as far as long-term oncological outcomes are concerned. The ProtecT trial reported similar rates of CSS and OS at 10 years between men undergoing active monitoring and those treated 4 ; similar results were provided by the PRIAS trial, although almost three-quarters of AS patients received definitive treatment over 10 years. 5
Disease progression with crossover to active treatment is reported in at least 20% to 30% of men, 5 –9 based on tumor heterogeneity, mutifocality, and risk of biopsy undersampling 6 ; moreover, an added number of patients (∼30%) may deliberately choose an active treatment owing to anxiety within 10 years. 10
It has been previously hypothesized that length of time from PCa diagnosis to RP may impair functional recovery, given a potential risk of progression over the waiting time with the need for a more extensive dissection. 11 Thus, it could be assumed that patients who delay an active treatment may lose the window opportunity to maximize the tradeoff between functional and oncological outcomes.
In this study, we report outcomes of robotic radical prostatectomy (RALP) in patients who underwent a prior surveillance of PCa, who referred to a high-volume tertiary center from different urological institutions, backgrounds, and strategies of monitoring. After a propensity score (PS) matching, outcomes were compared to those from a similar cohort of men undergoing immediate RALP.
Methods
Among a cohort of 11.000 PCa patients, who underwent RALP from June 2013 to April 2020 at a high-volume referral center (Celebration, FL), 181 patients have been initially treated with an AS strategy. The indication to AS and the monitoring were recommended at different institutions and patients referred for RALP owing to upgrading (65%) and/or for individual decision (i.e., anxiety). Data were retrieved from a prospectively maintained database (Institutional Review Board approval number 237998-40). After a PS matching, these patients with initial assumed AS were compared to those who had immediate RALP. Inclusion criteria were body mass index (BMI) <35 kg/m2, no previous local treatment for PCa, and at least 1-year of follow-up after RALP. The patients had postoperative appointments at 6 weeks and 3, 6, 9, 12, 18, 24, 30, and 36 months after surgery. For both groups, the time between the operative decision and the OR scheduling is the same.
The primary endpoint of the study was to compare outcomes of RALP between patients who underwent delayed RALP after an assumed AS strategy and those who underwent RALP as the initial active treatment matched for the same demographics as men who initially were managed with surveillance. Outcome measures were pT, pathological tumor grade, the rate of extracapsular extension (ECE), of positive surgical margin (PSM), nodal status, and biochemical recurrence (BCR) rate. BCR was defined as prostate-specific antigen (PSA) >0.2 ng/mL. The number of full bilateral nerve-sparing procedures and of pelvic nodal dissection (PND) was considered secondary endpoints, together with continence and potency rates. Urinary continence was defined as the use of no pads and potency as the ability to achieve and maintain erections sufficient to perform intercourse (with or without phosphodiesterase type 5 inhibitor use).
PS matching
To reduce the biasing effect of potential confounders, 181 patients who underwent RALP after surveillance were matched with 181 patients (1:1 ratio) who underwent RALP as the initial active treatment. The PS was estimated using a multivariable logistic regression model that considered the ISUP grade at the time of assumed AS paired with preoperative biopsy ISUP of the group initially operated. The following variables at the time of surgery were also considered in the model: age, BMI, Charlson comorbidity index (CCI), preoperative Sexual Health Inventory for Men (SHIM) score, American Urological Association symptom score (AUASS), prostate size, PSA levels, PSA density, and cT. Matching was performed using the nearest-neighbor matching algorithm (caliper width 0.2 of the standard deviation of the logit score) with a 1:1 ratio without replacement.
Statistical analysis
Statistical analysis and reporting were performed according to established guidelines. 12,13 The two-sample Wilcoxon rank-sum test was used to test the hypothesis of equal distributions in the matched groups for the preoperative continuous variables. For categorical variables, the proportions in the matched cohorts were compared using Fisher's exact test. For continuous outcomes, the confidence intervals (CIs) of the median difference between the two study groups were estimated by the Hodges-Lehmann method. 14 In addition, the STSURVDIFF module in Stata 15 was used to calculate, for the time to event outcomes, the difference of cumulative incidences at a fixed time point between the study cohorts. Cumulative incidence functions for potency and continence recovery and BCR were estimated using the Kaplan-Meier method. The statistical analyses were performed using Stata version 16 (Stata Corp., College Station, TX) and R version 4.0.2. Statistical significance was set at p < 0.05 for a two-tailed test.
Results
The study comprised two different RALP groups: (1) n = 181 patients who underwent RALP after an initial surveillance strategy and (2) n = 181 patients who underwent RALP after PCa diagnosis (controls) with similar preoperative characteristics after PS matching. All procedures were carried out by a single high-volume surgeon (V.P.) using the da Vinci SI and Xi console. A concomitant PND was performed according to nomograms and/or tumor grade, after counseling the patient. The time distribution of interventions was similar between groups with 75% (137/181) and 70% (128/181) of RALP performed from 2017 to 2019 in the AS and in the control group, respectively (p = 0.07).
Baseline patient characteristics
Biopsy results are according to the International Society of Urological Pathology grade groups. When entering the surveillance, 152 patients (84%) had an ISUP 1, 21 (11%) had an ISUP 2, and 7 (4%) had an ISUP 3.
Table 1 reports ISUP grade (one of the matching variables) for the surveillance group (ISUP at surveillance entrance) and for immediate RALP group (preoperative ISUP).
ISUP Grade for Patients Entering Heterogeneous Surveillance Protocols and for Patients Undergoing Immediate Robotic Radical Prostatectomy in the 1:1 Matched Cohort
RALP = robotic radical prostatectomy.
Table 2 presents the preoperative demographics of the groups after PS matching. At the time of RALP, age, cT, BMI, Charlson Comorbidity Index (CCI), preoperative SHIM score, prostate weight, total PSA, PSA density, and preoperative AUA symptoms score were similar between groups. The median number of biopsies in the AS group was 2 (interquartile range [IQR] 2–3); patients spent on surveillance a median number of 35 months (IQR 21–53).
Preoperative Demographics After Matching, Including Number of Biopsies for Patients on Prior Surveillance
Continuous variables are reported as median and IQR and categorical variables as absolute and percentage frequencies.
Applicable for surveillance group (overall number of biopsies performed counting the initial biopsy performed to select the patient for AS).
AS = assumed active surveillance; AUASS = American Urological Association symptom score; BMI = body mass index; IQR = interquartile range; PS = propensity score; PSA = prostate-specific antigen; SHIM = Sexual Health Inventory for Men.
Perioperative and postoperative characteristics
The perioperative and postoperative characteristics are described in Table 3. The median blood loss, the proportion of patients with blood loss >100 mL, and the catheter time did not differ significantly between groups. The median console time was higher for delayed RALP (80 minutes) compared to RALP after diagnosis (75 minutes), maybe related to a higher rate of PND procedure after surveillance. As far as surgical planning is concerned, a full bilateral nerve-sparing strategy was planned in a significantly lower number of patients in the surveillance group (32%) compared to patients in the control group (51%). A significantly higher number of patients after surveillance (61%) underwent PND, compared to 34% of patients in the immediate RALP group. The rate of Clavien ≥ IIIb complications did not show significant differences between groups.
Comparison of Perioperative and Postoperative Characteristics Between the 1:1 Matched Cohorts
Continuous variables are reported as median and IQR and categorical variables as absolute and percentage frequencies.
EBL = estimated blood loss
Pathological and functional outcomes
The pathological characteristics for the matched cohorts are reported in Table 4. Overall, the frequency of pathological grade pattern 4 and 5 was significantly higher in delayed prostatectomies; the occurrence of pT3, ECE and lymphovascular invasion was significantly higher in the prior assumed AS group compared to patients with an immediate RALP. The number of patients with nodal invasion was similar between groups.
Comparison of Pathological Characteristics Between the 1:1 Matched Cohorts
Continuous variables are reported as median and IQR and categorical variables as absolute and percentage frequencies.
The median follow-up after RALP was 24 months. The recovery of continence did not significantly differ between surveillance patients and controls (hazard ratio [HR] 0.9; 95% CI: 0.8–1.2; p = 0.6), as well as for potency recovery for preoperative SHIM ≥21 and age ≤65 (HR 1; 95% CI: 0.6–1.6; p = 1).
The risk of BCR was significantly higher for patients who had a delayed RALP after surveillance compared to those who underwent immediate RALP (HR 4.0; 95% CI: 1.4–12; p = 0.013) (Fig. 1). Table 5 lists cumulative continence rates, potency rate, and biochemical-free survival rates at different time points for the study groups.
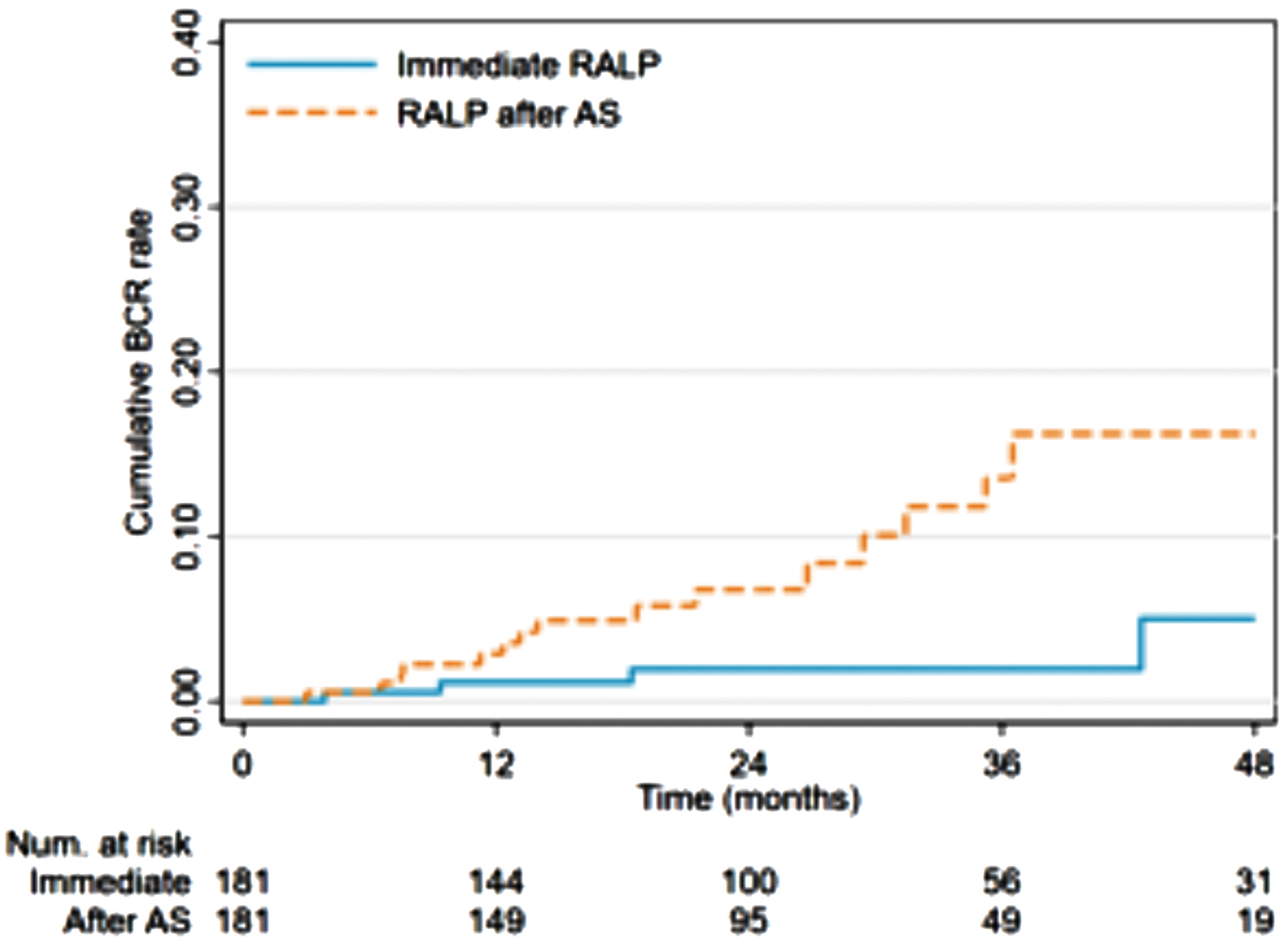
Kaplan-Meier estimates for BCR between Groups (Immediate RALP vs. RALP after an assumed prior AS protocol). AS = active surveillance; BCR = biochemical recurrence; RALP = robotic radical prostatectomy. Color images are available online.
Cumulative Incidence at Different Time Points for Time to Event Outcomes
For preoperative SHIM ≥21 and age ≤65.
BCR = biochemical recurrence; CI = confidence interval; HR = hazard ratio.
Discussion
AS is recognized as a treatment of choice for low-risk PCa and offers important benefits in reducing overtreatment and preserving quality of life.
Recognizing the safety on long-term CSS and OS, the heterogeneity of AS patients and protocols may affect the outcomes of delayed surgery, compared to those of patients elected to immediate radical prostatectomy.
We performed a matched paired analysis with the ISUP score as the first variable of matching from the initial biopsy (at the beginning of surveillance for AS patients); other variables of matching were collected at the time of surgery for both groups (age, BMI, prostate size, cT, preoperative SHIM, etc.) to homogenize factors possibly impacting RALP intervention and outcomes.
From this study, the risk of grade pattern 4 and 5, non-organ confined disease (pT3), ECE, lymphovascular invasion is higher in patients undergoing a delayed active treatment. Likely, this occurrence may have accounted for a higher risk (HR 4) of BCR for men with a delayed prostatectomy compared to those undergoing immediate surgery, at a median follow-up of 24 months after RALP.
Pathological outcomes of surgery from this series are consistent with those from Maggi et al. 16 Authors performed a retrospective analysis of long-term risk of metastasis in 1450 men on AS. 16 Approximately, a third of them (412) had a crossover to surgery and analysis of prostatectomy specimens showed 38% of pT3 or greater, 38% of ECE, and 23% of PSMs. BCR was not assessed, nodal metastasis itself (pN1)—and not the follow-up after surgery—was considered a primary endpoint. 16
Opposite to our study, Ahmad et al. 7 found no significant difference between immediate and delayed prostatectomy in terms of long-term oncological outcomes. Authors performed a retrospective analysis of 170 men who were initially diagnosed with clinically nonsignificant PCa and underwent a deferred RP. With a one to four matched paired comparison to men undergoing immediate prostatectomy, similar rates of pT3, PSM, pN1, and 5-year BCR were found. 7
However, the matching was performed with de novo GG2 or greater undergoing immediate prostatectomy; thus, the latter group may display outcomes similar to those of patients progressing during AS, but possibly poorer than those of men fitting the initial definition of clinically nonsignificant PCa (Gleason Score 6), while entering AS. To address this issue, we choose the ISUP score at the very first diagnosis of PCa as the primary variable of matching, aiming to explore a possible alternative course of low-risk patients if an immediate RP would have been offered.
To note, our findings may not reflect the general outcome of patients undergoing surgery after a standardized and monitored AS protocol but are rather representative of the real-life experience of a high-volume tertiary center, where primarily surveilled patients are referring from different institutions and settings with unknown protocols. On the other hand, AS patients in the studies of Maggi and Ahmad derived from single institutions with definite eligibility criteria and surveillance schedules.
Indeed, patients primarily surveilled referring only for RP may be a heterogenous group and outcomes of a salvage or deferred surgery may vary accordingly. Several factors may contribute to this heterogeneity.
First, criteria to enter AS and strategies for monitoring evolved during time. The recently released EAU guidelines 1 suggest that a “personalized risk-based approach will ultimately replace protocol-based management of patients on AS.” Even if agreeable, such a recommendation makes AS patients prone to different schedules of monitoring that could enhance the variability of AS cohort with possible impact on salvage surgery.
Second, the recent inclusion of Gleason 3 + 4 favorable intermediate-risk patients into AS may further enhance the heterogeneity of outcomes of salvage surgery. From the study of Yang et al., evaluating 10.089 patients with 3 + 4 favorable intermediate-risk PCa, approximately one in three patients harbored a disease of higher stage and grade and required an active treatment. 17 Consistently, the 2021 EAU guidelines suggest AS to highly selected grade group 2 disease (i.e., <10% pattern 4, PSA <10 ng/mL, ≤cT2a, low disease extent), but with the added disclosure of potentially increased risk of metastatic progression. 1
Third, the variability in grade attribution is another matter of concern affecting the quality of a low-risk cancer diagnosis: the interpathologists' concordance with respect to the Gleason sum is reported to be 58% (K = 0.43) and also after the ISUP 2014 update, a certain level of interobserver variability still persists, with a degree of discrepancy close to 45%. 18 –20 Thus, grading attribution may vary according to pathologist's experience, setting, and accessibility to a second opinion or central revision.
Fourth, tumor's bilaterality has been recently recognized as a factor likely to be related to disease progression to Grade Group ≥2 during AS. 21
Finally, several factors other than those PCa related can influence the decision to undergo a definitive treatment: the socioeconomic status, race, marital status, insurance status, and geographical differences 22 may account for different clinical backgrounds of patients referring for surgery.
Beyond these considerations, a deferred active treatment may have an impact on surgical preplanning. From this study, a PND is more likely to be performed in patients undergoing RALP after a prior surveillance. It is well known that the procedure itself may adversely impact the morbidity of surgery, with additional risk of PND-related complications such as symptomatic lymphocele or deep vein thrombosis. 1 Thus, patients who enter AS should be counseled about the risk of a more invasive surgical approach in case of progression or delayed choice of an active treatment if a strict AS protocol is not followed.
Overall, the morbidity of surgery is not significantly impaired by a delayed RALP in this study.
Operative console time is significantly higher in the AS group, although the clinical impact of this difference is likely to be negligible. As far as surgical strategy is concerned, a nerve sparing is less performed in the AS group; thus, potency recovery of men could be adversely affected, especially in those with a low preoperative SHIM score. 23 However, potency and continence rates are not adversely affected by a delayed surgery; again, it could be speculated that surgeon's volume may lead to these accurate outcomes, whereas a poorer postoperative course could be otherwise expected.
As known, treatment-related drawbacks are the principal cause of regret among patients undergoing surgery: the issue should be considered when counseling patients about a delayed surgical treatment. 24
This study is not devoid of limitations. The retrospective nonrandomized design is the main one.
The absence of information about criteria of AS/monitoring is another issue since patients came from different institutions and data about patient's adherence to AS criteria were unavailable too. Moreover, despite the increasing diffusion of multiparametric magnetic resonance imaging, its practice has not been recorded within this dataset. Finally, the absence of a long-term follow-up avoids any conclusion on CSS and OS.
Given these limitations, the article might raise some concerns about the long-term outcomes of a delayed RP after heterogeneous surveillance strategies in real-life practice. With a significantly higher BCR rate, primarily surveilled patients are more likely to undergo adjuvant treatments after RP—in this series—carrying related toxicities and possible increased morbidity. Salvage radiation therapy may be associated with acute grade 2 toxicity, especially for genitourinary symptoms, with effects increasing with dose escalation and seemingly persisting with newer planning and treatment techniques. 1
Thus, even if accounting for safe long-term oncological endpoints (CSS and OS), heterogeneous AS strategies followed by prostatectomy may increase the overall burden of cancer-related care.
Conclusions
In a high-volume tertiary center, patients with PCa primary surveillance from diverse backgrounds referred for RALP consist of a heterogeneous group leading to variable and less predictable outcomes of surgery, compared to those with similar disease undergoing immediate surgery. Pathological stage and grade are seemingly worsened for delayed prostatectomies after heterogeneous surveillance strategies, and a more aggressive preplanning is likely to impact functional outcomes. In this scenario, the significantly higher BCR rates suggest an increased burden of cancer-related care in patients undergoing prostatectomy after prior surveillance, compared to similar patients undergoing immediate surgery. We believe that these outcomes are useful for surgeons and patients while planning and following AS protocols.
Footnotes
Authors' Contributions
B.R.: project development. M.C.S.: project development and article writing. M.C.M.: data collection. M.S: statistical analysis. S.A.: data analysis. G.B.: article editing. S.M.: article editing. S.B: data collection. V.P.: project development.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was provided for the article