
Abstract
Introduction:
Approximately 3% of pregnancies are complicated by symptomatic hydronephrosis and up to 0.8% with urolithiasis. Pain, coupled with the possibility of superimposed infection, increases the risks of premature labor and delivery, fetal loss, and caesarian sections. Surgical intervention as well as standard ionizing radiation imaging modalities are typically avoided making this a difficult, high-risk patient cohort to manage. In this study we propose a standardized contemporaneous approach to investigations and management in the pregnant population with acute upper tract pathology analysis.
Methods:
A literature search of PubMed, Cochrane, and EMBASE databases was performed to identify original, peer-reviewed articles from 2010 onward on the management of ureteral calculi and symptomatic hydronephrosis occurring during pregnancy. Search yielded 5636 articles and after exclusions, 24 full-text articles met inclusion criteria for analysis.
Evidence Synthesis:
Ultrasound remains the cornerstone of initial investigation with MRI in reserve if the diagnosis remains uncertain. Low-dose CT imaging can be used in limited cases. Conservative approaches for symptomatic hydronephrosis as well ureteral calculi is the preferred initial management option in the well patient. If intervention is required, ureteral stent and nephrostomy can be used with informed consent on the risks and benefits of each. Primary ureteroscopy with definitive stone management in centers with the appropriate expertise can safely deliver excellent stone-free rates and symptomatic improvement.
Conclusions:
Individualized investigation and management plans following a structured approach in pregnant women with symptomatic hydronephrosis or calculi are discussed. At all stages, the patient, obstetrician, anesthetist, and surgeon should be involved in a shared decision-making approach.
Introduction
Physiological hydronephrosis is found in 90% of pregnant women by 28 weeks' gestation and develops from as early as 6 weeks of gestation. 1 The etiology of maternal hydronephrosis is multifactorial owing to compression of the ureter against the pelvic brim from the enlarging uterus, increased progesterone causing smooth muscle relaxation with reduced peristalsis. The right ureter is typically more hydronephrotic because of the overlying congested uterine vein and dextrorotation of the uterus. Therefore, the diagnosis of true renal colic can be difficult to diagnose in pregnancy. 2 Furthermore, even in the absence of stones, symptomatic physiological hydronephrosis can be found in up to 3% of pregnancies with the majority of stone diagnoses and admissions for renal colic occurring in the third trimester. 3,4
Pain and ureteral stones in pregnancy are significant medical concerns as they may precipitate complications such as gestational diabetes, hypertension, preeclampsia as well as premature labor and delivery, low birth weight or fetal loss and an increased need for caesarean sections. 4 –6 Incidence has been estimated at 0.49% of all pregnancies. 7 Urinary stasis owing to symptomatic hydronephrosis or obstructing ureteral calculi predispose to urinary tract infections, urosepsis, and acute renal impairment. 8 In addition, pregnant patients are a complex group considering surgical intervention and radiation exposure are typically avoided because of the potential risks to both mother and fetus. In this study, we propose protocolized assessment and management of these patients to standardize their treatment and prevent adverse outcomes.
Methods
Search strategy
An electronic literature search was performed using PubMed/Medline, Cochrane, and EMBASE library databases to identify original peer-reviewed articles on the optimal management of ureteral calculi and symptomatic hydronephrosis occurring during pregnancy (Figure 1). The search was performed using the following MeSH terms and search strategy: “(pregnancy) AND (urolithiasis) OR (kidney stones) OR (hydronephrosis).”
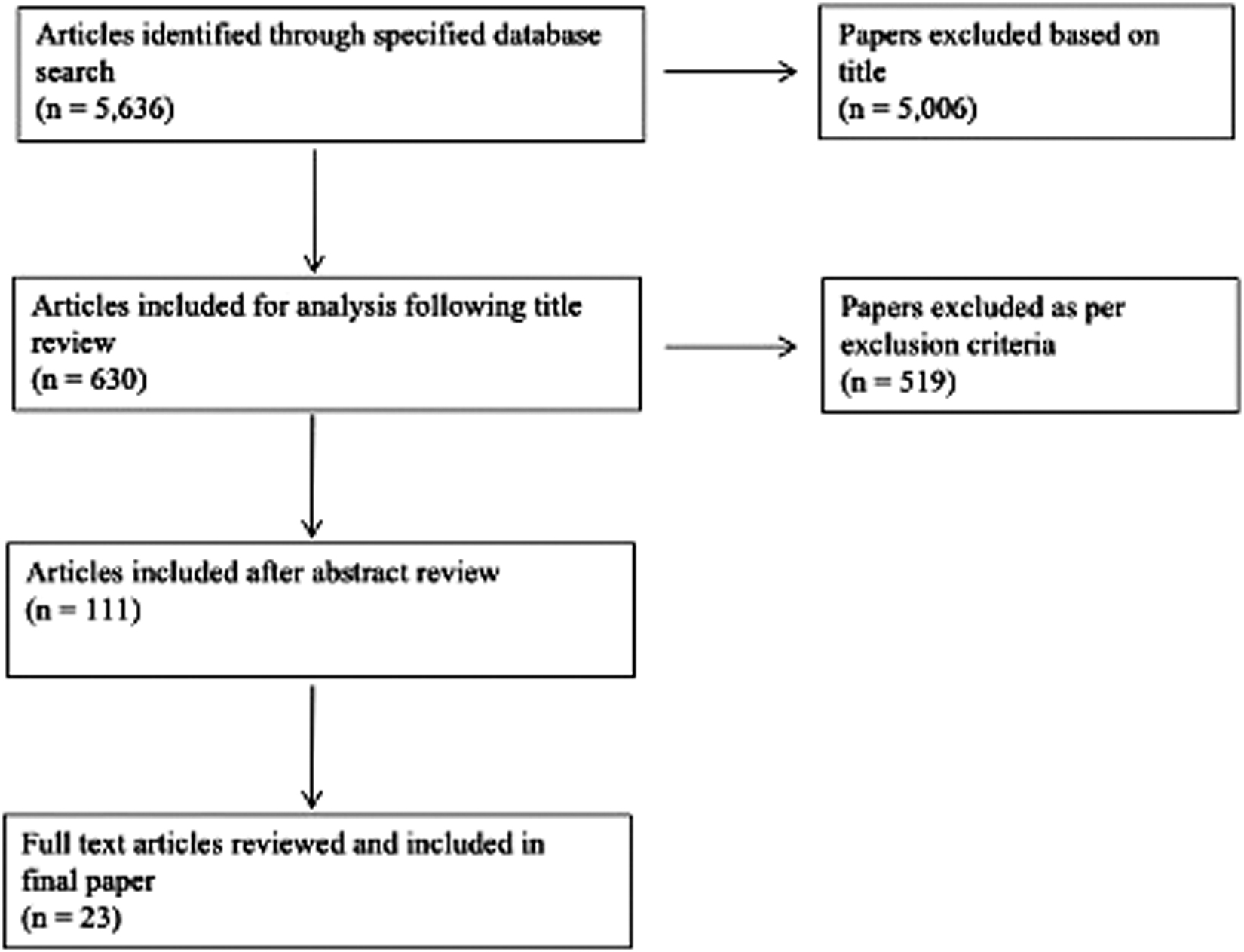
Search strategy used for suitable articles for review of stones and hydronephrosis in pregnancy.
Inclusion/exclusion criteria
Articles in the English language and articles from the last decade (2010 onward) were selected to provide contemporaneous evidence. All published peer-reviewed studies or articles on optimal care of pregnant patients with urolithiasis or symptomatic hydronephrosis were considered for inclusion with the exception of review articles. Each eligible publication's reference section was reviewed for further appropriate inclusions.
Data extraction
The initial search yield 5636 articles with 111 articles included for assessment of eligibility. All titles and abstracts were reviewed independently by two authors (R.A.K. and N.F.D.) to exclude duplicates and to limit selection bias. Twenty-four suitable full-text articles pertaining to the epidemiology, diagnosis, management, and outcomes of symptomatic hydronephrosis or urolithiasis in pregnancy were retrieved and analyzed, after exclusions. Study characteristics are summarized in Table 1.
Studies Used in Review of Investigations and Management of Urolithiasis and Gestational Hydronephrosis in Pregnancy
CD = Clavien–Dindo; DJS = Double-J stent; CRP = C-reactive protein; (F)URS = (flexible) ureteroscopy; GA = general anesthetic; HASTE = half Fourier single-shot turbo spin-echo; KUB = kidney, ureter, and bladder radiograph; LDCT = low-dose computed tomography; LOS = length of stay; MAPD = maximal anterior–posterior diameter; MET = medical expulsive therapy; MR = magnetic resonance; MR(I/U) = magnetic resonance (imaging/urogram); MRU = magnetic resonance urography; NST = nephrostomy; PCN = percutaneous nephrostomy; PCNL = percutaneous nephrolithotomy; PPV = positive predictive value; QoL = quality of life; SFR = stone free rates; TA = transabdominal; TAUS = trans abdominal ultrasound; TV = transvaginal; TVUS = transvaginal ultrasound; USS = ultrasound scan; VAS = visual analog scale; WCC = white cell count.
Discussion
In this study we summarize the body of evidence made available in the last 10 years with respect to the various means of imaging the pregnant patient with flank pain to confirm the diagnosis. After this, options and evidence of management in a stepwise manner culminating in a proposed management flowchart are presented.
Diagnostic imaging during pregnancy
Ultrasonography
Patients with symptomatic hydronephrosis or renal colic will typically present with flank, loin, or back pain with vomiting, hematuria, and fevers/rigors if there is associated infection. Ultrasonography is the first-line imaging modality in a pregnant patient with such symptoms. Ultrasonography is safe as there is no ionizing radiation or contrast media required, as well as being inexpensive and reproducible. Ultrasonography is particularly useful for identifying hydronephrosis, renal calculi, pelviureteral or proximal ureteral stones, as given in Figure 2. The grade of hydronephrosis does not appear to have a significant association with the severity of pain. 9 Ultrasound has an estimated 45% and 94% sensitivity and specificity, respectively, for ureteral stones, whereas White et al. found a 77% positive predictive value (PPV) for ultrasonography in pregnant patients who subsequently underwent ureteroscopy. 10,11
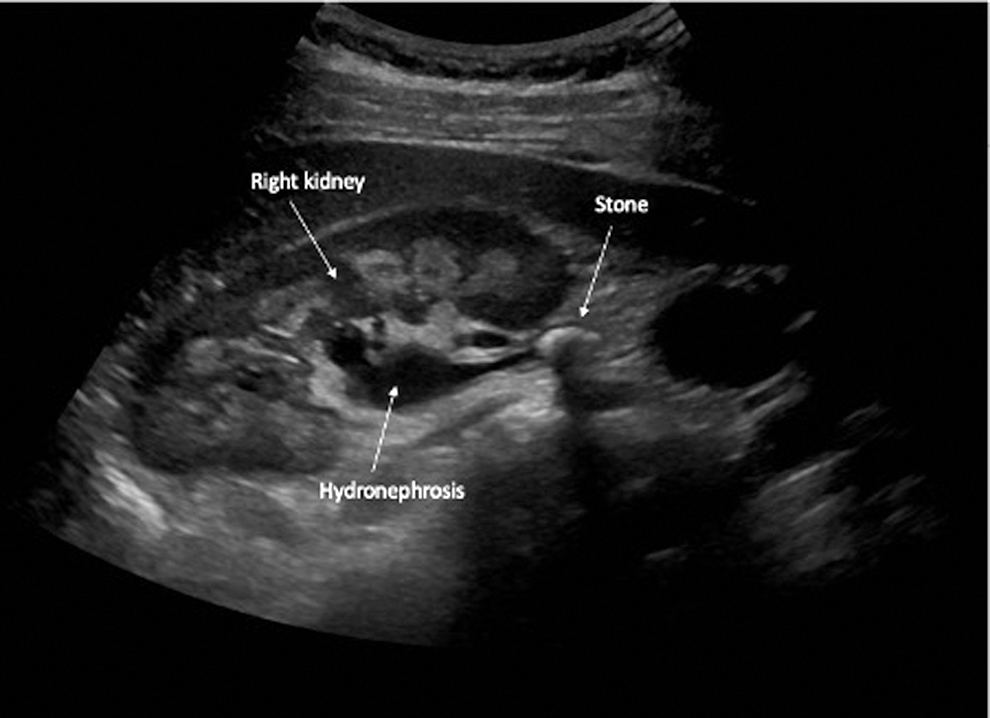
Right proximal ureteral stone and hydronephrosis in a patient of 10 weeks' gestation.
Sensitivity of ultrasonography in differentiating physiological hydronephrosis from an obstructive cause can be aided by calculating resistive indices (RI) (peak systolic blood flow of intrarenal blood flow minus the end diastolic blood velocity divided by the peak systolic velocity). Resistive index is typically maintained in physiological hydronephrosis, therefore RI >0.7 should be considered as pathological. 5 Transvaginal ultrasonography can be used to adjunctively identify distal ureteral stones, ureterectasis, as well as assessing for the presence of ureteral jets, the absence of which may indicate complete ureteral obstruction although other authors have found no statistically significant difference. 12,13 Ureteral jets may be absent in up to 15% of asymptomatic pregnant women. 5 Absence, however, should only be confirmed when the patient has been assessed in the contralateral decubitus position also. 14
Considerable variability may be seen between patients owing to factors such as patient's body mass index, trimester of pregnancy, and sonographer experience. Bladder filling can also alter image interpretation; therefore, patients should be encouraged to be hydrated. 14 Transvaginal and transabdominal ultrasound, when combined, can yield 85% sensitivity for distal ureteral stones, 100% specificity as well as a negative predictive value of 98% when no distal stone and no hydronephrosis are identified. 13 Use of a systematic approach using a combination of transabdominal and transvaginal imaging, calculation of RI, and thorough assessment of ureteral jects in the hydrated patient can optimize diagnostic scanning and minimize interuser variability. 14
Magnetic resonance urography
The European Association of Urology (EAU) have recommended magnetic resonance urography (MRU) as the appropriate second-line diagnostic investigation in pregnancy to identify ureteral calculi where ultrasonography is inconclusive. 10 1.5 Tesla MRI has been evaluated for use in pregnancy, although 3 Tesla has not and is therefore not recommended during pregnancy. 10 The use of intravenous gadolinium is not recommended owing to potential teratogenic side effects. 10 The American College of Obstetrics and Gynecology (ACOG) in conjunction with the American College of Radiology have advised that MRI is safe in all trimesters of pregnancy, with no evidence of harm arising from tissue/amniotic fluid heating, acoustic effects, or teratogenic effects. 15 MR urogram remains safe because of the absence of radiation exposure while providing cross-sectional imaging, allowing confirmation of hydronephrosis as well as severity and location of transition point or filling defect. Features such as gradual tapering of the ureter to the middle third owing to external uterine compression, as given in Figure 3, favors physiological causes, compared with the presence of perirenal fluid, renal enlargement, and abrupt ureteral ending as seen in calculi. 16,17 A “double kink” sign, a standing column of urine below the pelvic brim with proximal ureteral dilation favors an obstructing ureteral calculus, with loss of the India ink artifact helpful in differentiating obstructive from physiological hydronephrosis. 16,18 Should a nephrostomy be placed for therapeutic intervention as discussed later in this article, water-enhanced MR nephrostogram has been described to delineate and characterize distal ureteral obstruction in the pregnant patient. 19

Left: Left hydronephrosis with gravid uterus. Right: Tapering of mid-distal left ureter owing to uterine compression.
Noncontrast computed tomography
Noncontrast computed tomography (NCCT) is more sensitive for diagnosing ureteral calculi compared with ultrasonography and MRI (97% PPV). However, significant radiation exposure to the fetus precludes its routine use. White et al. used low-dose CT imaging in 24 pregnant patients with inconclusive ultrasound scans, which confirmed presence of a stone in all patients with mean radiation dose of 645 mrad (equivalent to 6.5 mGy) per patient. 11 Intrauterine death, growth retardation, carcinogenesis, and mutagenesis can occur with ionizing radiation, although this is felt to be negligible at <50 mGy. 15,20 Ultra-low dose CT scans for calculi can achieve sensitivities and specificities ranging from 72% to 99% and 86% to 100%, respectively, while delivering an average dose of <1.7 mSv (equivalent to 1.7 mGy), permitting more accurate diagnoses while delivering even lower radiation exposure to the fetus. 21 Guidelines, such as those adopted by the ACOG and EAU, recommend that no investigation, including CT, is withheld in pregnancy if it will contribute to the decision-making process in their care, such as emergencies of persistent symptoms despite a “normal MRI,” although judicious use of radiation is advised. 10,15 CT should therefore be reserved as a third-line radiological investigation if a diagnosis is required and ultrasound and MRI have proven inconclusive. Figure 4 provides the CT kidney, ureter, and bladder radiograph of a patient of 27 weeks gestation with an obstructing right mid-ureteral stone.
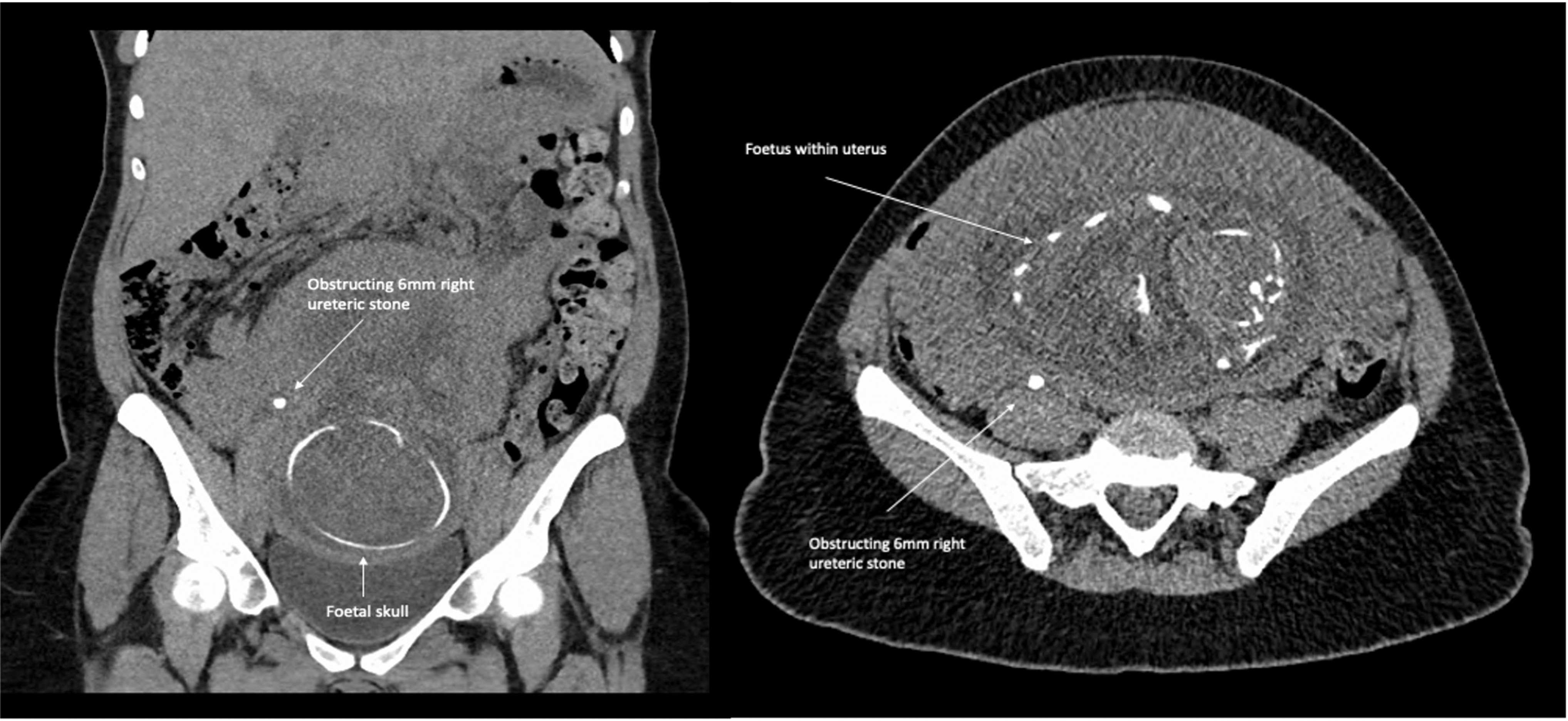
CT KUB coronal (left) and axial (right) sections showing 6 mm right mid-ureteral obstructing stone. KUB = kidney, ureter, and bladder radiograph.
Management of stones in pregnancy
Management of symptomatic ureteral calculi should involve a multidisciplinary team including a urologist, obstetrician, radiologist, and anesthetist if operative intervention is being considered. Most cases of uncomplicated ureteral calculi in pregnancy can be managed conservatively, with up to 94% of patients not necessitating intervention according to Spralding et al., although the true figure of confirmed stone passage is felt to be much lower at 48%. 22,23 Indications for procedural intervention include intractable or severe symptoms, evidence of infection, worsening renal impairment, or fetal distress/premature labor.
Conservative management of stones should be encouraged where possible, with adequate hydration and analgesia safe for use in pregnancy. Nonsteroidal anti-inflammatory drugs (NSAIDs), typically used in to treat renal colic, are not recommended for routine use in pregnancy owing to risk of closure of fetal ductus arteriosus in utero, persistent pulmonary hypertension of the newborn, and they may delay the onset of labor. 24 Medical expulsive therapy with an alpha blocker such as tamsulosin has been shown to be safe in pregnancy for both mother and fetus, although tamsulosin does not demonstrate a statistically significant difference in likelihood for stone passage. 25,26
Overview of interventional procedures
Intervention in the unwell, persistently symptomatic (>24 hours despite analgesia) or deteriorating patient with symptomatic hydronephrosis involves cystoscopy stent insertion or percutaneous nephrostomy insertion, with ureteroscopy also an option if ureteral stones are diagnosed. The choice of procedure should reflect the capabilities of the treating center as well as availability of, and access to, experienced urologists, anesthetists, and interventional radiologists. In one review of >14,000 patients in the United States with ureteral calculi during pregnancy, of those who underwent intervention (5.2%), most patients (3.3%) underwent stent insertion only, with 0.6% undergoing nephrostomy insertion and the remaining 1.3% of patients undergoing definitive ureteroscopy and stone treatment. 22
Retrograde ureteral stenting
Retrograde ureteral stents can be inserted using general anesthetic, spinal/epidural, or local anesthetic. Preterm delivery and low birth weight have been associated with pregnant patients receiving nonobstetric anesthesia, particularly during the third trimester; therefore, the patients must be fully informed of the potential associated risks. 27 There is level 1b evidence to suggest that ureteral stents are better than conservative management in symptomatic moderate to severe hydronephrosis in pregnancy, although conservative measures should still be trialed first owing to irritative stent-associated symptoms. 28 An advantage of ureteral stents is that they are internalized and less likely to become dislodged. Disadvantages include requirement for an anesthetic as well as discomfort and symptoms because of the stent itself. Stent symptoms should not be underestimated, with one study demonstrating that 42% of pregnant patients undergoing early induction of labor owing to intolerable stent pain, compared with 0% after ureteroscopy. 23 Ureteral stents may also hinder stone passage and have been shown to rapidly encrust in pregnancy, necessitating repeat exchanges. One comparative study assessing ureteral stents to ureteroscopy and nephrostomy in 54 patients showed stents to have the lowest rate of success and highest rate of complications and recommend change every 4–6 weeks owing to risk of encrustation. 29
Percutaneous nephrostomy
Percutaneous nephrostomy insertion for symptomatic hydronephrosis in pregnancy was first described in 1992. 30 It can be performed with local anesthetic under ultrasound guidance, obviating the need for general anesthetic and its associated risks. Additional advantages include higher stone passage rate, better tolerance, and less urinary symptoms compared with ureteral stents. 31 Nephrostomies however are externalized and are therefore uncomfortable and may dislodge. Overall, percutaneous nephrostomy has not been proven to have any overall benefit in the febrile obstructed kidney compared with ureteral stenting in all populations, with a 4% complication rate in one meta-analysis. 32 Similar to ureteral stents, percutaneous nephrostomies can rapidly encrust, often necessitating repeated changes for the duration of pregnancy. 33 Requirement for changes averages 1.6 times per pregnancy every 21–33 days. 33,34
Ureteroscopy
Ureteroscopy was traditionally considered as the last line for surgical intervention; however a growing body of evidence suggests that ureteroscopy is a reasonable and safe alternative to ureteral stenting or nephrostomy with less symptomatic side effects. 35,36 Ureteroscopy confers the advantage as being diagnostic as well as therapeutic with the additional benefit of obviating the need for ureteral stenting in uncomplicated cases as described in one study that reported a 45% stent-free rate among 116 ureteroscopy procedures. 37 –39 Stone-free rates of 85% have been reported in one systematic review on >270 cases with no maternal or fetal deaths. 37 Ureteroscopy has been performed in all trimesters of pregnancy although nonurgent cases are safest in the second trimester by an experienced endourologist. 10,40 As with ureteral stent insertion, ureteroscopy may be performed under spinal or general anesthetic. No significant difference in anesthetic time or anesthetic events has been seen between those necessitating ureteroscopy compared with those with indwelling stents, although the stented patients are more likely to require induction of labor owing to intractable symptoms. 41 It must be emphasized that any pregnant patient with an obstructed collecting system with features of sepsis should not have primary ureteroscopy performed and should be urgently decompressed by ureteral stent or nephrostomy. Definitive stone management should be deferred until the patient is clinically well and sepsis resolved 42
Ureteroscopy guidance with ultrasound is feasible and safe with minimal associated complications and allows avoidance of radiation compared with fluoroscopy. 43 Figure 5 provides confirmation of correct stent placement after ureteroscopy. Fluoroscopy may be used and was found in systemic review to have been used in 20%–25% of 271 ureteroscopies in pregnancy from 1990 to 2012. 44 Measures to minimize maternal and particularly fetal exposure should be undertaken such as lead shielding, c-arm inversion, image acquisition with a dose as low as reasonably possible, collimated fields and pulsed imaging. 45 The typical armament of instruments available to assist in stone fragmentation such as holmium lasers, pneumatic lithotriptors (e.g., Lithoclast®), and endoscopy stone baskets have all been reported safely and successfully in pregnancy. 37 Reported complications arising from ureteroscopy during pregnancy range from 7% to 13% and include minor complications such as hematuria, pain, and urinary tract infections. Major complications including ureteral perforation and urosepsis have also been described. 37,46 Specific obstetric complications include premature uterine contractions, premature labor, and premature delivery. 37,46,47 Premature uterine contractions and risk of urosepsis have been shown to be directly correlated to delay in timing to operation as well as to the presence of fevers at presentation. 38 No maternal or fetal mortalities have been documented to date with ureteroscopy.
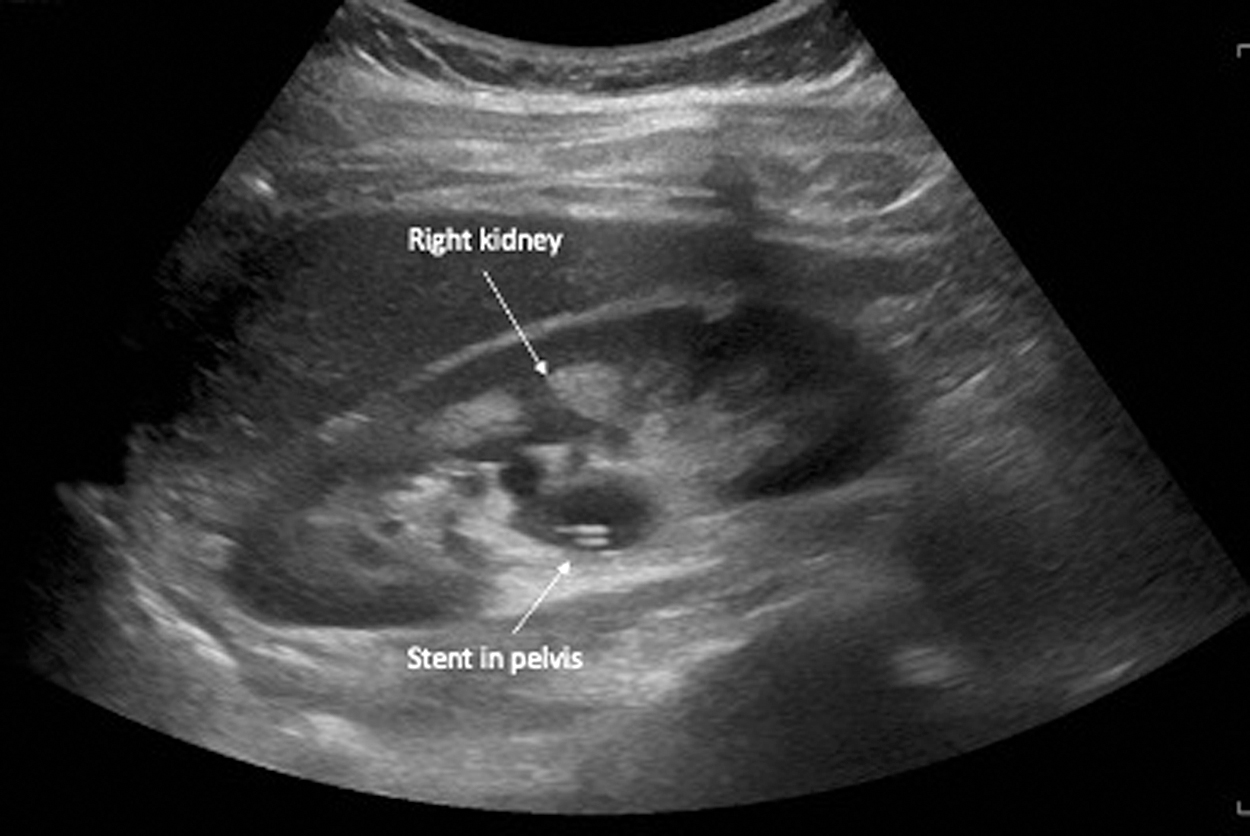
Resolution of hydronephrosis and confirmation of stent position after ureteroscopy for proximal ureteral stone.
Extracorporeal shock wave lithotripsy and percutaneous nephrolithotomy
Owing to the shock waves and ionizing radiation used during treatment, extracorporeal shockwave lithotripsy (ESWL) remains an absolute contraindication in the pregnant female although any pregnant patients inadvertently undergoing ESWL have not had any reported detrimental effects. 10,48,49 Percutaneous nephrolithotomy (PCNL) remains a last option; however, it should only be performed in experienced centers on a case-by-case basis when nephrostomy or ureteral stents fail to control the patient's symptoms, and ureteroscopy is unlikely to alleviate symptoms. One review of 16 cases achieved stone-free status in all with 14 completed with ultrasound guidance under spinal or general anesthesia. All cases with the exception of five were performed prone, which becomes more difficult as pregnancies progress, although no cases had any associated perioperative complications. 50
Management of Symptomatic Hydronephrosis in Pregnancy
In patients with symptomatic hydronephrosis of pregnancy, similar therapeutic options including conservative management, ureteral stent insertion, and percutaneous nephrostomy insertion also apply. The majority (80%–94%) of the patient's symptoms will settle with conservative management. 51 Raised C-reactive protein (CRP), white cell count (WCC), pretreatment visual analog scale (VAS) of pain, preterm labor rate, and maximal anterior–posterior renal pelvis diameter (MAPD) have all been identified as predictors of patients who will fail conservative treatment and required intervention in second and third trimester patients. 2
For patients who require intervention, percutaneous nephrostomy insertion, as given in Figure 6, is associated with significantly less secondary and tertiary reinterventions and at less intervals compared with ureteral stents. 34 Ureteral stents have a lower failure rate compared with conservative management; however, they should still remain as second-line intervention owing to the risks and symptoms associated with stent insertion. 28 Complications typically occur when stents are left for more than 3 months; therefore, changes should occur before this time. 28 Patients with pain-persistent ureteral stent pain can proceed to percutaneous nephrostomy insertion, although symptomatic improvement appears better who have nephrostomy insertion in an unstented kidney. 33 With regard to nephrostomy exchanges, some institutions recommend changes as often as every 2 weeks owing to the rapid encrustation seen in pregnancy, making subsequent exchanges more difficult. 33
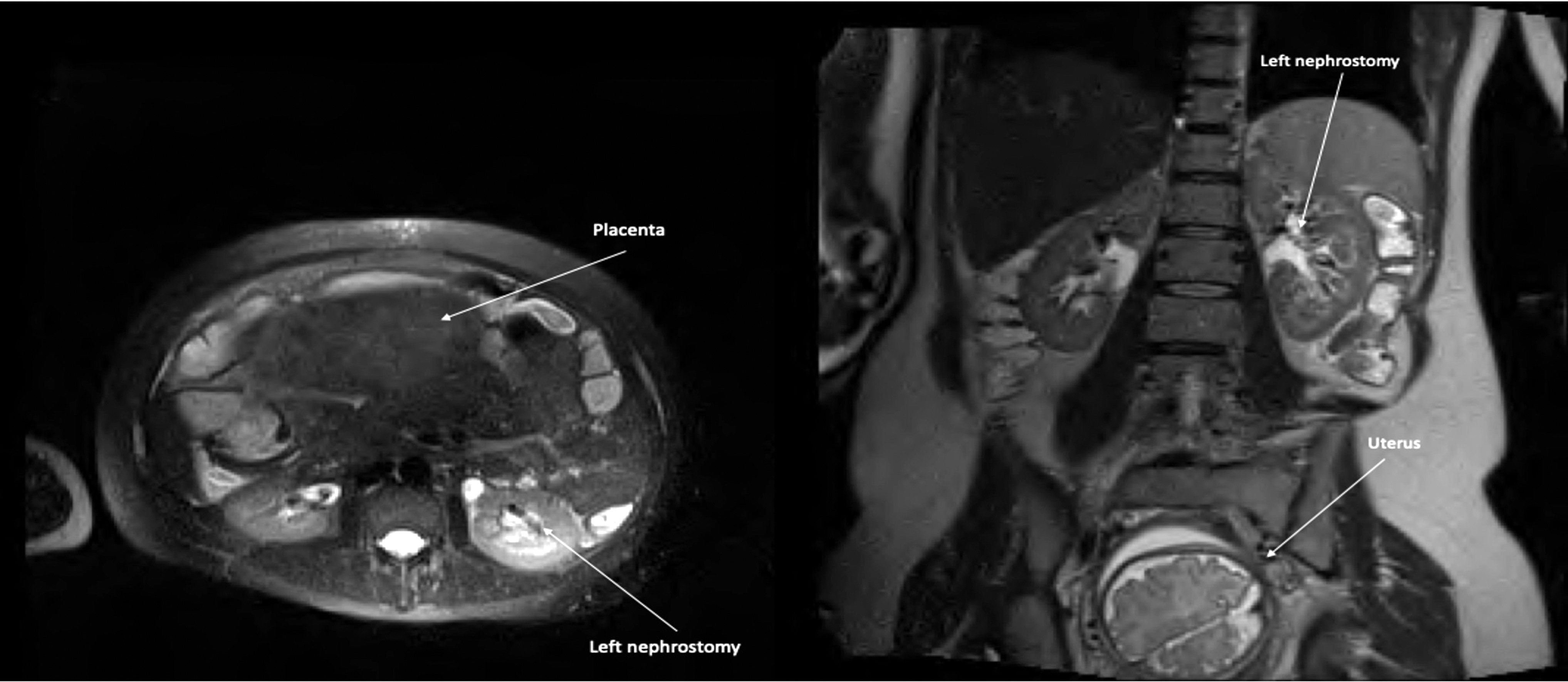
Axial and coronal images of left nephrostomy inserted for symptomatic gestational hydronephrosis.
Summary of Evidence and Management Algorithm
Figure 7 provides a proposed algorithm based on the summary of evidence presented herein. Pregnant patients presenting with abdominal pain should be initially assessed by an obstetrician. For persisting nonobstetric abdominal or flank pain, basic investigations should include blood tests including WCC, CRP, and renal function with urinary dipstick/culture and sensitivity.
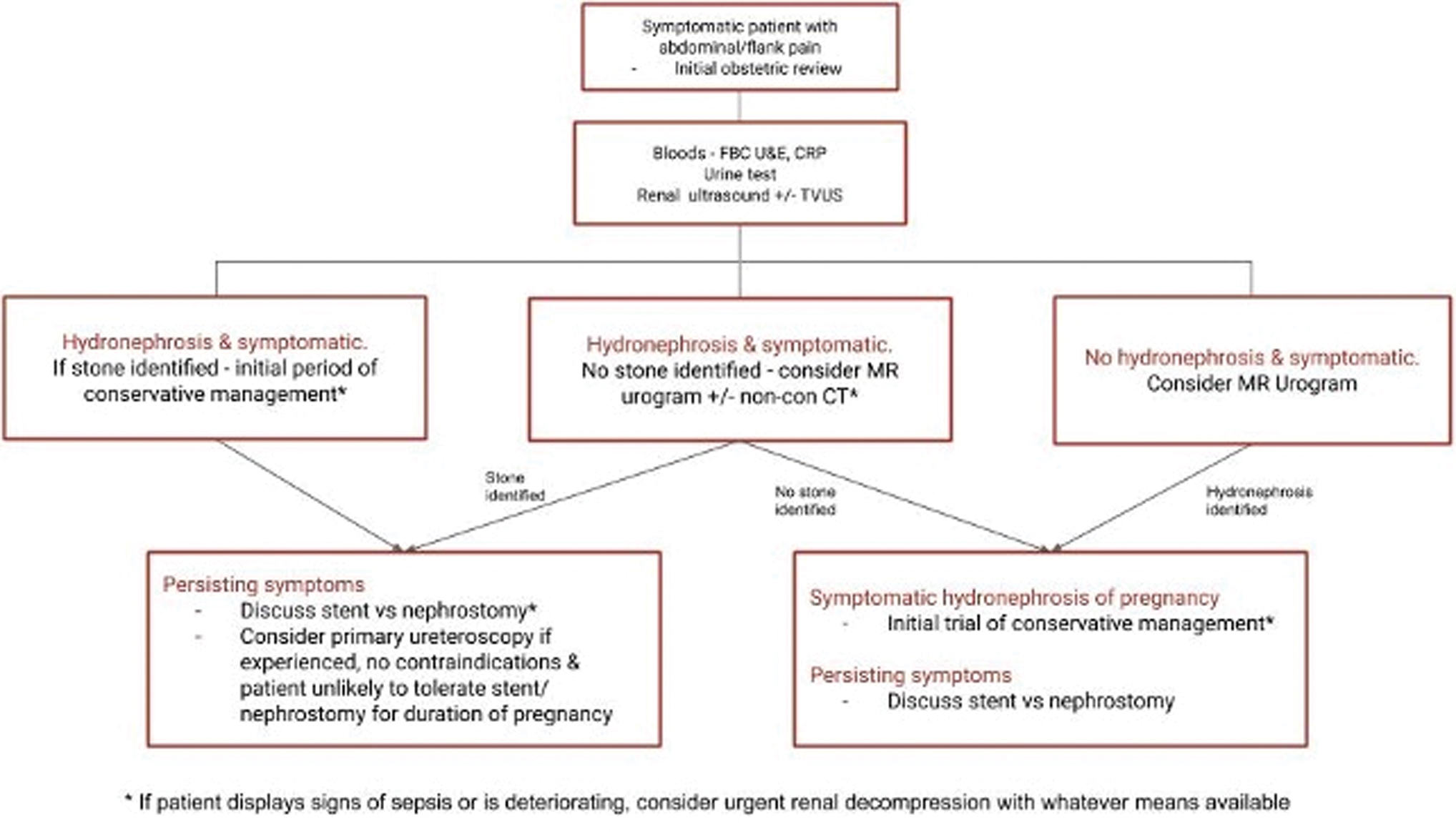
Proposed workflow of managing flank pain in obstetric patients. CRP = C-reactive protein; FBC = full blood count; MR = magnetic resonance TVUS = transvaginal ultrasound; U&E = urea and electrolytes. Color images are available online.
Initial radiological imaging aims to assess for hydronephrosis and, if present, the patient should be interrogated further for the presence of an obstructing ureteral stone. A focused renal ultrasound assessing for the presence of hydronephrosis with calculated resistive index should be performed. Further transvaginal images with a full bladder assessing for ureteral jets or identification of a distal ureteral stone can also be obtained. If this remains inconclusive, 1.5 Tesla MRI without the use of gadolinium can identify the presence or absence of a specific filling defect or differentiate physiological from pathological hydronephrosis. Low-dose CT imaging can be used as a last line noninvasive investigation in an unwell or persistently symptomatic patient without a diagnosis.
First-line treatment for both ureteral calculi and symptomatic hydronephrosis of pregnancy in the majority of patients is conservative management. Failing this, both ureteral stents under sedation, local or general anesthetic and percutaneous nephrostomy insertion can be utilized depending on availability and access for each interventional modality. Nephrostomies have less patient-reported side-effects and need fewer reinterventions; however, no significant difference between both interventions has been observed. For confirmed ureteral calculi, ureteroscopy can be performed safely in experienced centers under ultrasound guidance with excellent stone-free rates and symptomatic improvement. PCNL is feasible in select cases and ESWL remains contraindicated. At all stages of management, the treating obstetrician, surgeon, anesthetist, and patient should be involved in a shared decision-making process.
Footnotes
Authors' Contributions
R.A.K: concept, design, literature review, manuscript draft, manuscript proof and submission. N.J.H.: concept and design. N.F.D.: Literature review, article draft, article proof.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.