
Abstract
Purpose:
To investigate the incidence, predictive factors, and health care utilization of sepsis post-ureteroscopy (URS) in patients enrolled in commercial insurance plans.
Materials and Methods:
A retrospective claims analysis was conducted using the IBM® MarketScan® commercial database. Patients ≥18 years were included if they had URS between January 2015 and October 2019 and developed sepsis within 30 days of URS. Multivariate logistic regression was used to identify various clinical and demographic predictors of sepsis post-URS. All-cause health care utilization (i.e., inpatient admissions and intensive care unit [ICU] stays) and all-cause health care costs up to 1 month post-septic event were measured.
Results:
Among the 104,100 URS patients meeting the inclusion criteria, 5.5% developed sepsis. Patients with diabetes (odds ratio [OR] = 1.52; p < 0.0001), older age (age 55–64 vs 18–34; OR = 1.35; p < 0.0001), baseline sepsis (OR = 3.51; p < 0.0001), baseline inpatient visits (OR = 1.17; p = 0.0012), and higher Elixhauser comorbidity scores (OR = 1.09; p < 0.0001) had a significantly higher likelihood of developing sepsis post-URS. In septic patients, 94.8% required inpatient care and 35% were admitted to the ICU. Mean hospital stay for septic patients was 6.86 days. Average all-cause health care cost per patient at 1 month in the septic cohort was $49,625 vs $17,782 in the nonseptic cohort indicating an incremental all-cause cost of $31,843 (p < 0.0001).
Conclusions:
A total of 5.5% of commercially insured patients undergoing URS developed sepsis post-URS. Diabetes, older age, baseline sepsis, baseline inpatient visit, and higher comorbidity score were all found to be independent predictors of post-URS sepsis. Patients with sepsis post-URS had higher health care utilization and costs indicating that sepsis is both a significant clinical and economic event.
Introduction
The prevalence of stone disease in the United States is ∼10.9% in men and 9.5% in women. 1 For the past four decades, the prevalence of stone disease has more than tripled in the U.S. population. 2 Patients with stone disease often experience debilitating pain, nausea, and renal insufficiency. 3 There are many factors associated with the high prevalence of stone disease including diabetes, gout, obesity, metabolic syndrome, environmental hazards, poor diet, and familial history. 1,4,5 In 2000, the total estimated cost for treating kidney stone disease was $4.5 billion annually in the United States ($9 billion in 2021 USD). 6
There are a number of surgical options available for patients with stone disease, including shockwave lithotripsy, percutaneous nephrolithotomy, and ureteroscopy (URS). One of the most common surgical treatments for stone disease is URS. 7 Although URS has a high success rate, there are a number of common complications associated with its use, including ureteral wall injury, ureteral stent discomfort, and urinary tract infection. 7
More severe complications include sepsis, multiorgan failure, and death. 7 Sepsis is a clinical syndrome caused by a host response to an infection that may potentially lead to organ failure or death. 8 Our recent meta-analysis found that the rates of sepsis originating from the urogenital tract varies substantially between studies (0.5%–17.8%) and the pooled incidence of urosepsis after URS was found to be 5%. 3 Although stone disease primarily affects working-age adults between 20 and 60 years, 4,6 no previous studies have examined the predictive factors and health care utilization of sepsis post-URS in a real-world setting using a large-scale database of patients with employer-sponsored health insurance.
The objectives of this study were to investigate the incidence, predictive factors, health care utilization, and all-cause costs of sepsis post-URS in patients enrolled in U.S. commercial insurance plans.
Materials and Methods
Study population
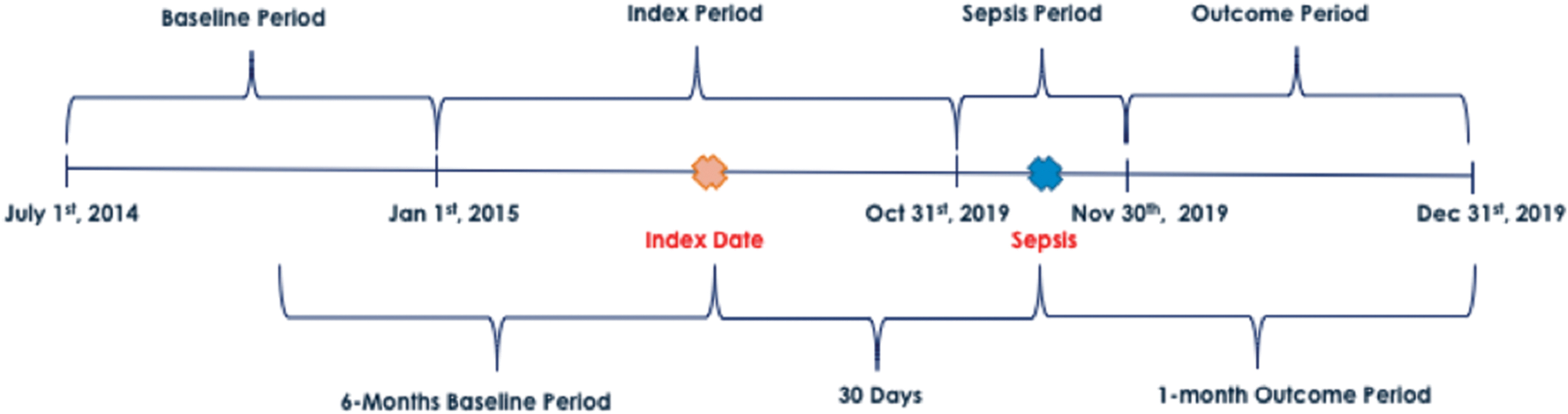
A retrospective claims data analysis was conducted using the IBM® MarketScan® commercial insurance database to identify patients who had a URS (index surgery) between January 2015 and October 2019 (Fig. 1). The IBM MarketScan commercial database is a nationally representative data sample of the U.S. population with employer-sponsored health insurance. 9 This database includes ∼40 million covered individuals from 160 contributing employers and 40 contributing health plans. 9 Since this database contains de-identified individual patient-level data and medical services claims data for all settings of care, no IRB approval was needed for this study.
Patient identification. Color images are available online.
The index URS procedure was defined using International Classification of Diseases-9th Revision (ICD-9) and ICD-10 procedure codes and Current Procedural Terminology (CPT) codes. A sepsis event was defined as the first septic event within 30 days following the index URS (including the date of the URS) using ICD-9 and ICD-10 diagnosis codes (Supplementary Tables S1 and S2). Events were analyzed as overall septic events and then subcategorized into severe septic events. Septic and severe septic events were examined together and separately. Patients ≥18 years were included if they had a URS procedure during the index period and had continuous enrollment in the health plan 6 months pre- and 2 months post-index date (Figs. 1 and 2). Patients were excluded if they had a septic event post-second URS procedure within 30 days of the index procedure or had health care utilization costs ≤$0.

Inclusion and exclusion criteria. URS = ureteroscopy. Color images are available online.
Patient characteristics and outcomes
The predictive factors of postoperative sepsis that were assessed included patient demographics (age, gender, and geographic region), comorbidities and Elixhauser comorbidity score, and clinical characteristics such as baseline sepsis, baseline inpatient visits, and baseline surgery for stone disease (i.e., lithotripsy, percutaneous nephrolithotomy, and URS) that occurred 6 months before the index URS (baseline period). Comorbidities examined included diabetes, hyperlipidemia, severe obesity, nonsevere obesity, and ischemic heart disease as defined by Quan et al. 10
Comorbidities were defined based on ICD-9 and ICD-10 diagnostic codes that the patient had during the 6-month baseline period before the index surgery (Fig. 1). Patients undergoing URS were categorized into two cohorts: septic patients and nonseptic patients. The outcome period (Fig. 1) was defined as follows: 1-month post-septic event (including the date of sepsis); 1-month post-URS for the nonseptic cohort (including the date of URS). Time to sepsis was calculated using the number of days from the index surgery date to the septic event date.
All-cause health care utilization was measured for both the septic cohort and nonseptic cohort in the outcome period. Further subanalysis compared the septic group with the severe septic group. Evaluation of health care resources included number of hospital inpatient stays, intensive care unit (ICU) visits, and length of hospital inpatient stay. The inpatient stays or ICU visits could have occurred any time during the outcome period. All-cause health care costs (medical costs and medication costs) were also measured for both cohorts during the outcome period.
Health care costs are the sum of the amount paid by the commercial insurer and the patient and include all costs such as inpatient, outpatient, and emergency department visits. Since stone disease is common among the working-age population, this analysis focused on the direct medical costs of patients with sepsis or without sepsis in working-age adults enrolled in employer-sponsored private health insurance plans. 4,6 Direct medical costs paid by other types of insurers, such as Medicare, were not included in this analysis. Indirect costs, such as time missed from work, were also excluded from the analysis.
Statistical analyses
We compared the patient characteristics and comorbidities of septic patients vs nonseptic patients using chi-square tests for categorical variables and t-tests for continuous variables. Multivariate logistic regression analysis was used to evaluate the clinical and demographic predictors of sepsis post-URS adjusting for all other covariates. Descriptive statistics were analyzed in the septic and nonseptic cohorts comparing health care utilization and costs.
Furthermore, descriptive statistics were also analyzed in the sepsis and severe sepsis cohorts comparing health care utilization and costs. The generalized linear model (GLM) with gamma distribution and log link was used to evaluate the effect of sepsis on medical costs adjusting for all other covariates. All medical costs were adjusted to 2020 USD using the medical component of the consumer price index. 11 The Instant Health Data software (Panalgo, Boston, MA) and R, version 3.2.1 (R Foundation for Statistical Computing, Vienna, Austria) were used to perform the analyses of this study at a priori significance of 0.05.
Results
Patient characteristics
Patient characteristics and comorbidities are presented in Table 1. The overall incidence of sepsis post-URS was 5.5% (5706/104,100) including 1.4% (1448/104,100) who developed severe sepsis as defined by their diagnosis code. Among the sepsis cohort, 82.3% of patients developed sepsis on the day of their URS. The average time to a sepsis diagnosis was 1.9 days (standard deviation ±5.2 days). In the sepsis cohort, 44.7% were aged 55 to 64 years, 71.6% were women, and the mean Elixhauser comorbidity score was 2.2 (±2.4).
Characteristics of Patients with Sepsis and Nonsepsis Post-Ureteroscopy
SD = standard deviation.
Predictive factors of sepsis post-URS
The results of the multivariate logistic regression showed that patients with diabetes (odds ratio [OR] = 1.52; p < 0.0001), older age (age 55–64 vs 18–34; OR = 1.35; p < 0.0001), baseline sepsis (OR = 3.51; p < 0.0001), baseline inpatient visits (OR = 1.17; p = 0.0012), and higher Elixhauser comorbidity score (OR = 1.09; p < 0.0001) had significantly higher odds of developing sepsis post-URS (Table 2). In contrast, males (OR = 0.36; p < 0.0001), patients with hyperlipidemia (OR = 0.75; p < 0.0001), nonsevere obesity (OR = 0.82; p < 0.0001), and baseline surgery (OR = 0.46; p < 0.0001) had a significantly lower likelihood of developing sepsis post-URS.
Predictive Factors of Sepsis Post-Ureteroscopy
Statistically significant.
CI = confidence interval.
Health care utilization and costs of sepsis post-URS
Patients who developed sepsis required significantly more inpatient care, had higher ICU utilization, and experienced longer inpatient stays compared with the nonseptic patients (Table 3 and Fig. 3). The small percentage of patients in the nonseptic cohort who were hospitalized (23.3%) had approximately half the length of stay as hospitalized septic patients. In addition, among those patients that were hospitalized, the percentage of patients requiring an ICU stay was ∼17 times higher in the septic cohort compared with the nonseptic cohort (35.3% vs 2.1%; p < 0.0001).
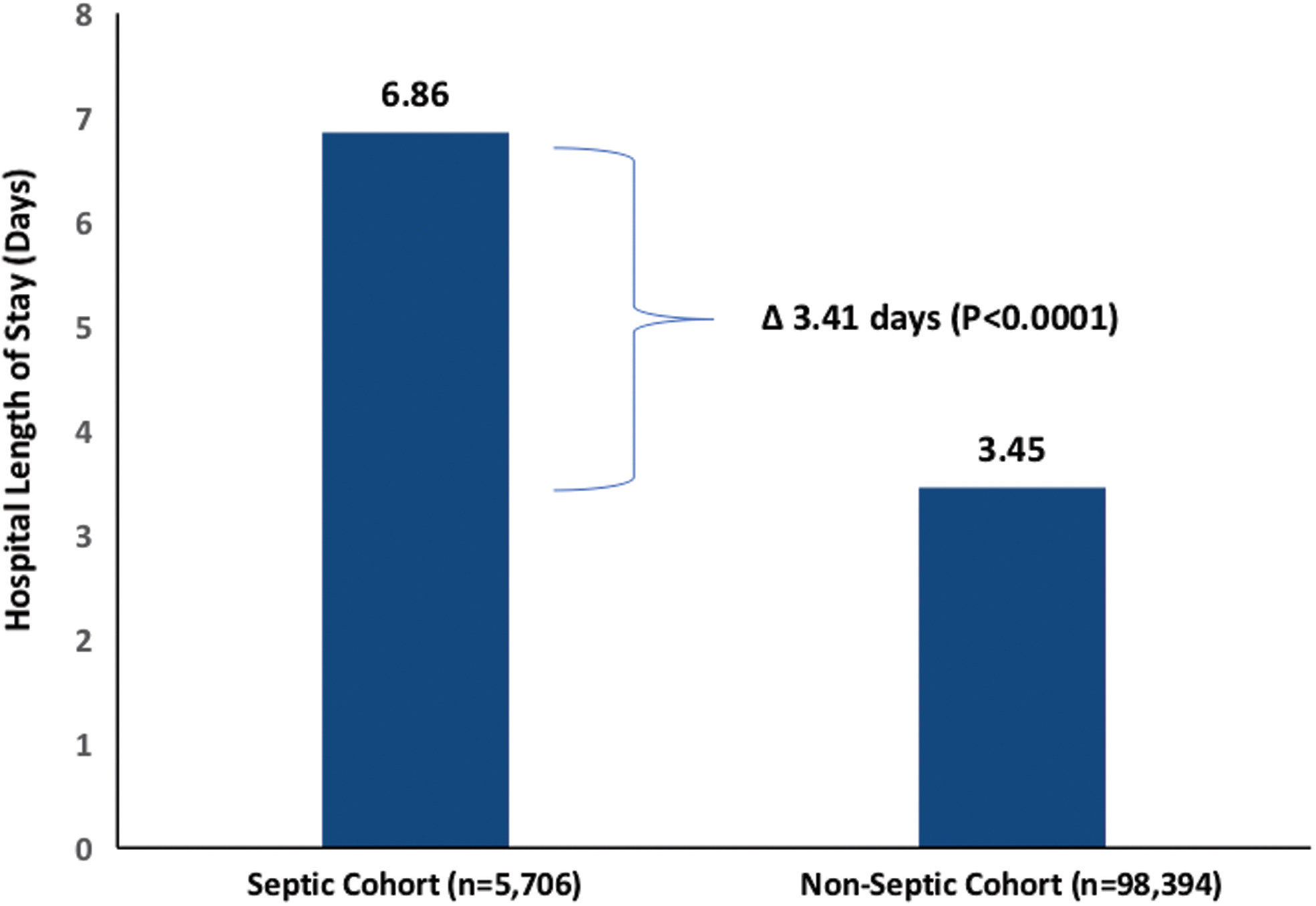
Hospital length of stay for septic patients (n = 5706) vs nonseptic patients (n = 98,394) post-URS. Color images are available online.
Health Care Utilization and Costs of Septic Cohort vs Nonseptic Cohort
The average all-cause health care costs at 1 month in the septic cohort were significantly higher than the average all-cause health care costs at 1 month in the nonseptic cohort ($49,625 vs $17,782; p < 0.0001) representing an incremental all-cause cost of $31,843 (Fig. 4). For those found to have severe sepsis, the average all-cause health care costs at 1 month were significantly higher than less severe septic patients ($68,892 vs $43,073) because of a longer inpatient stay (9.32 days vs 5.98 days) and a greater frequency of ICU admissions (66.3% vs 24.7%). The results of the GLM model evaluating the effect of sepsis on health care costs adjusting for all other covariates showed that the septic cohort was significantly associated with higher all-cause health care costs at 1 month compared with the nonseptic cohort (OR: 2.5; 95% confidence interval: 2.44–2.6; p < 0.0001).
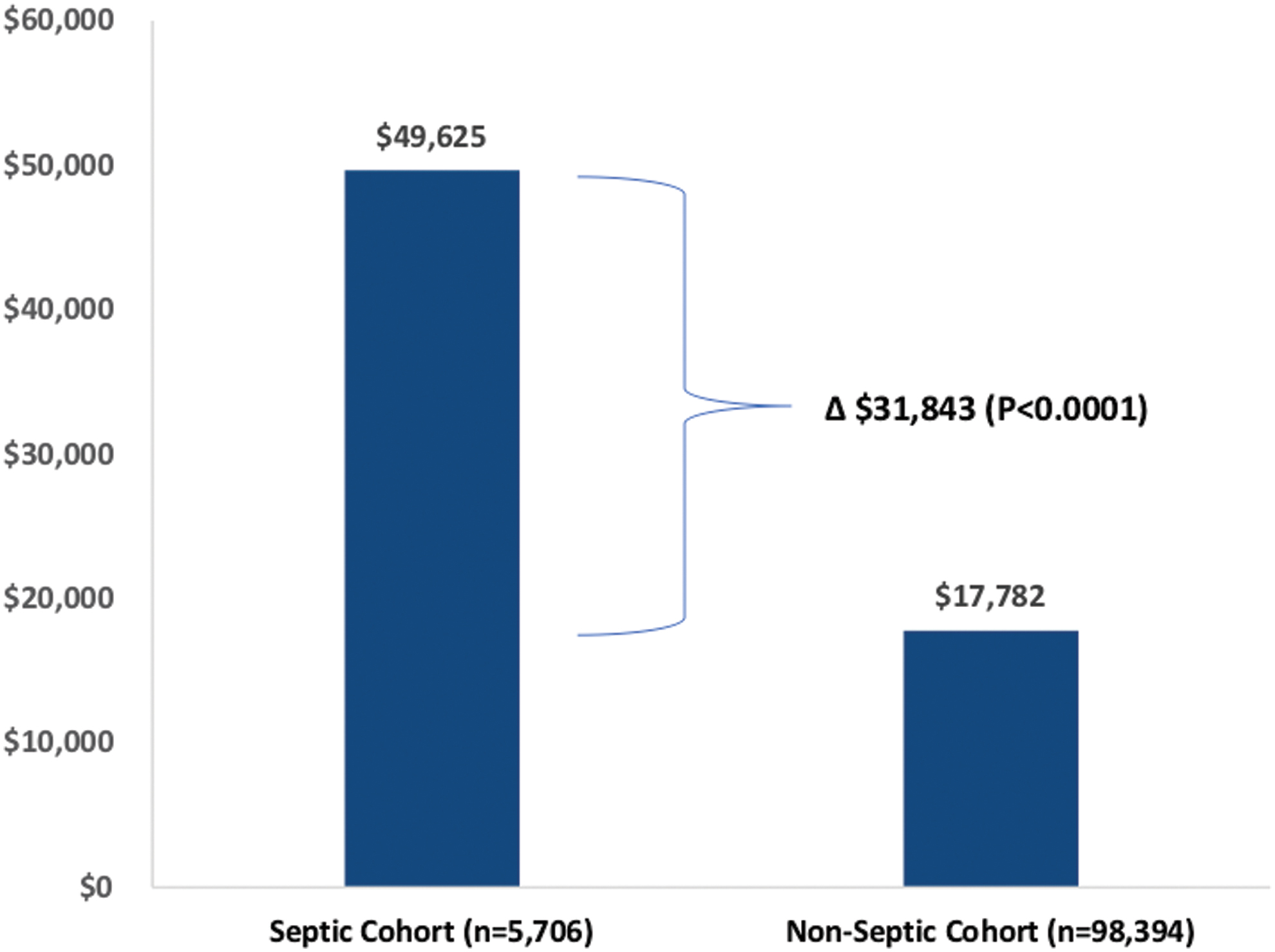
Average all-cause health care costs* at 1 month for septic patients (n = 5706) vs nonseptic patients (n = 98,394) post-URS. *Costs in 2020 USD. Color images are available online.
Discussion
This was the first study to examine the predictive factors and health care utilization of sepsis post-URS in a real-world setting using a large-scale database of patients with employer-sponsored health insurance. Overall, we found that diabetes, older age, baseline sepsis, baseline inpatient visit, and higher comorbidity score were independent predictors of post-URS sepsis. We also found that patients with sepsis post-URS had substantially higher health care utilization and costs than nonseptic patients.
Our study's findings on the incidence rate of sepsis post-URS in a large U.S. commercial insurance population of >100,000 patients are consistent with those of previously published studies. 3,12 –14 We previously conducted a meta-analysis to quantify the risk of postoperative sepsis after URS from 13 studies with 5597 patients and found that the pooled incidence of postoperative sepsis was 5.0%. 3 In addition, the meta-analysis showed that the incidence rates for sepsis varied extensively between studies. This variance in the rate of sepsis between studies may be caused by a lack of standardized reporting systems between institutions, differing settings of care for postoperative management of this condition (i.e., since onset of the condition may occur between 1 and 2 days later), and potential misdiagnosis of this condition (i.e., cystitis). 3
Lu and colleagues examined the rate of sepsis after flexible URS (n = 759 patients) and found that sepsis occurred in 43 patients (5.7%) and 6 patients (0.8%) developed septic shock. 12 Wood and colleagues examined ureteral stent cultures in 227 patients receiving ureteral stents at a single center and found a 5.7% postoperative sepsis rate. 13 A recent literature review (n = 187 studies) by De Coninck et al found that severe complications of URS such as sepsis may be underreported worldwide thus providing urologists with an “unwarranted sense of security” when performing URS. 7 Finally, although 82.3% of the patients were found to be septic on the day of the procedure, the average time to sepsis was 1.9 days. This might potentially indicate a second peak moment for developing sepsis and future studies can investigate any plausible differences between the immediate and delayed cohorts.
Our study's findings on the predictive factors of sepsis post-URS are also consistent with those of previously published studies. 14 –16 Chugh and coworkers conducted a systematic review to quantify the predictors of infectious complications (including sepsis) after URS for stone disease from 14 studies with 24,373 ureteroscopies and found that risk for infectious complications was higher in elderly patients, patients with a higher Charlson comorbidity index, female patients, and patients with longer stent indwelling time. 15 Bloom et al examined risk factors for sepsis after elective URS in 345 patients and found that multiple comorbidities, prior endoscopic procedures, and longer operative times were associated with sepsis. 14 Blackmur and associates investigated the risk factors associated with postoperative sepsis in 462 patients at a single institution and found that the presence of diabetes mellitus, the presence of ischemic heart disease, and same-session bilateral URS were some of the factors associated with postoperative infection. 16
Finally, our study's findings on the health care utilization and all-cause costs of sepsis post-URS were similar to those of previously published studies. 14,17,18 Arefian and colleagues undertook a systematic review to examine the hospital-related costs of sepsis from 37 studies and found that the hospital cost of sepsis per patient was $32,421 and the ICU cost of sepsis per patient was $27,461 per patient (costs in 2014 U.S. dollars). 17 Bloom and colleagues examined medical resource utilization associated with sepsis after elective URS in 345 patients and found that septic patients required an additional 5.33 days of hospitalization per patient. 14 Cole and coworkers investigated the length of infection-related hospitalizations after 1817 URS procedures in 11 practices and found that the median time to admission caused by an infection-related complication was 4 days after the index URS procedure and the median length of stay was 3 days. 18
Study limitations and strengths
Although our population of interest was anyone who had an index URS procedure, most of the patients undergoing the procedure were treated for stone; therefore, our results remain generalizable to the stone population. This analysis was limited to examining the predictive factors and health care utilization of septic patients post-URS only in working-age adults enrolled in commercial insurance plans. The analysis did not include an examination of the predictive factors or costs in older patients paid by other types of insurers such as Medicare.
Although stone disease is common among working-age adults, the prevalence is increasing in older patients. 2 Costs in this elderly population may be even higher than in working-age adults and should be investigated further. The study included all-cause health care costs and not costs solely associated with sepsis; however, we showed a difference between all-cause costs between those without sepsis compared with patients who became septic. Future studies should investigate costs exclusively associated with sepsis. Furthermore, the present analysis did not include indirect costs such as missed work, which can be significant.
Future research examining the costs of sepsis post-URS should include both direct and indirect costs among patients of all age groups, regardless of payor status. Singer et al defined sepsis as a life-threatening organ dysfunction caused by a dysregulated host response to infection. 19 Future studies can evaluate health care utilization and costs using the new definition. Finally, since this is a claims-based analysis, we cannot confirm if patients coded to have had sepsis also clinically had sepsis according to sequential organ failure assessment (qSOFA) or Systemic Inflammatory Response Syndrome (SIRS). Also, since laboratory-based data such as preoperative urine culture was not available, we could not assess if guideline recommendations were followed or not. Many of these limitations are inherent to private payor claims database analyses and do not preclude the development of clinically relevant conclusions.
Despite these limitations, this study has a number of strengths. This was the first study that examined health care utilization and costs of sepsis post-URS from the perspective of commercial insurers in the United States using a large-scale database. More specifically, this study employed a longitudinal comparative approach that followed septic and nonseptic patients for a 30-day period to comprehensively capture the health care utilization and costs of >100,000 working-age adults undergoing URS.
This large data set comprises a representative sample of working adults in all regions of the United States and in multiple settings of care, which improves the generalizability and validity of the findings. In addition, this analysis identified the key predictive factors associated with sepsis in a real-world setting and was the first to examine health care utilization associated with ICU care among sepsis cohorts post-URS. Furthermore, this study validates the key finding from the Bhojani et al. meta-analysis of a pooled incidence of post-URS sepsis rate of 5% but in a large working-age population and using a unique claims analysis study design. 3
Conclusions
This study showed that 5.5% of U.S. commercially insured patients undergoing URS developed sepsis. Diabetes, older age, baseline sepsis, baseline inpatient visits, and higher comorbidity score were all associated with higher rates of sepsis. Patients with sepsis post-URS had substantially higher health care utilization and costs compared with nonseptic patients indicating that sepsis is both a significant clinical and economic event. The findings from this study underscore the importance of risk stratification of patients in the preoperative setting and surveillance of patients in the postoperative setting to reduce sepsis-associated morbidity and costs. Finally, results of this study are generalizable to similar populations.
Footnotes
Authors' Contributions
All of the authors met the following criteria: made substantial contributions to the conception or design of the study; or the acquisition, analysis, or interpretation of data for the study; and drafted the article or revised it critically for important intellectual content; and approved the final version to be published; and agreed to be accountable for all aspects of the study in ensuring that questions related to the accuracy or integrity of any part of the study are appropriately investigated and resolved.
Acknowledgment
We thank Michael Mafilios at Health Economics Associates, San Diego, CA for the medical writing assistance provided.
Author Disclosure Statement
N.B. is a board-certified urologist and associate professor of urology at the University of Montreal and was engaged by Boston Scientific as a clinical expert and scientific advisor for this research. B.H.C. is a urologist and associate professor of urology at the University of British Columbia and was engaged by Boston Scientific as a clinical expert and scientific advisor for this research. N.B. and B.H.C. were not compensated for their participation in this study. R.P., B.C., and S.R. are employees of Boston Scientific.
Funding Information
Support for this research was provided by Boston Scientific, Marlborough, MA.
Supplementary Material
Supplementary Table S1
Supplementary Table S2
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.