
Abstract
Objectives:
To compare the short-term and 1-year follow-up functional outcomes of modified anatomical structure preserving and Retzius-repairing robot-assisted radical prostatectomy (APR-RARP) compared with Retzius-sparing (RS) RARP.
Methods:
Eighty consecutive patients 40–75 years of age with low-intermediate risk prostate cancer were prospectively randomized to APR-RARP or RS-RARP. Urinary continence (UC) recovery rates were evaluated from catheter removal up to 1 year follow-up. Postoperative UC was defined as 0 pads/one security pad per day. UC recovery rates from catheter removal to 1 year were calculated by Kaplan–Meier curve; log-rank test was used for the curve comparison. Postoperative potency was evaluated at 3 and 12 months after surgeries. Perioperative complications, positive surgical margin (PSM), and biochemical recurrence rates represent secondary outcomes reported in the study.
Results:
At the catheter removal, 1, 3, 6, and 12 months after operation, 52.5% (confidence interval [CI] 95%: 37.6–67), 82.5% (CI 95%: 70.8–94), 95% (CI 95%: 88.3–99.1), 97.5% (CI 95%: 92.5–99.9), and 97.5% (CI 95%: 92.5–99.9) of men undergoing the APR-RARP were continent (0 pads/one security pad per day), compared with 61.5% (CI 95%: 46.5–76.6), 89.7% (CI 95%: 80.3–98.1), 97.5% (CI 95%: 92.6–99.9), 97.5% (CI 95%: 92.6–99.9), and 97.5% (CI 95%: 92.6–99.9) undergoing the RS-RARP, respectively, and the Kaplan Meier curve showed no statistically significant difference for both technique at any time point (log-rank p = 0.556). The median (95% CI) time to UC recovery was 9.8 (5.2–14.4) days for the APR-RARP vs 6.7 (3.2–10.2) days for the RS-RARP group. Potency rates were similar in both groups at 3 and 12 months after surgeries. The two compared approaches; in terms of rate of complications, PSM was similar.
Conclusions:
Surgeons can achieve functional results comparable to the RS technique with the modified reconstructive anterior approach, without changing the surgical technique they are used to.
Introduction
Radical prostatectomy (RP) is the standard treatment method widely used in clinically localized and locally advanced prostate cancer (PCa). The main purpose of RP is to completely remove the tumor tissue and provide the best oncological result, as well as recovery postoperative urinary continence (UC) and erectile functions. 1 Depending on the severity of urinary leakage, incontinence is one of the important complications that seriously affect the quality of life after RP. 2 The effort to improve functional results has led to the continuous development and evolution of the robotic technique and different approaches have been tried to achieve the best. 1
In standard robot-assisted radical prostatectomy (RARP), there may be a risk of deterioration of anatomical structures that contribute to the UC mechanism because of the need for access to the Retzius space. 3 For this purpose, in 2010, Galfano et al. described a surgical technique performed through the douglas space in RP that preserves the Retzius and the structures involved in the continence mechanism. 3 In addition, it was supported by other studies that early UC recovery rates are higher with the Retzius-sparing (RS) technique, 4 and in some series, immediate UC rates at the catheter removal were reported to be higher in the RS technique. 5 However, it was stated that there was no significant difference in 1-year results between the standard technique and the RS technique. 4,5
When the current literature is reviewed, the early continence advantages of the RS technique compared to the standard technique are emphasized. On the other hand, most surgeons still have not abandoned the standard technique, and a recent questionnaire of 250 participants showed that only 11% of RARP was performed using the RS-RARP approach. 6 Although various continence preserving techniques have been tried in the standard RARP procedure, the high-quality evidence for these techniques in the literature is limited. 7 –10
The focus of our study is lack of a randomized prospective study comparing the modified reconstructive anterior approach, which we define as modified anatomical structure preserving and Retzius repairing (APR), and the RS technique in the evaluation of postoperative functional outcomes. Differerent from the current literature, the aim of this study is to evaluate the results of a single-surgeon prospective randomized comparative study on functional outcomes at 1-year follow-up between APR-RARP and RS-RARP for clinically localized prostate cancer (PCa) treatment.
Methods
Study design
This prospective randomized study was carried out between January 2018 and January 2020, after achieving the ethics committee approval. Eligible patients were randomized in a 1:1 allocation ratio and 80 consecutive patients with clinically localized PCa underwent RARP by APR (40 patients) and RS (40 patients) approach by a single surgeon (K.T.) and surgical team at a tertiary care institution, according to a parallel design. The assignment of each patient to the first or second treatment group was randomized with a computer-based randomization table.
The study included patients between the ages of 40 and 75 years, life expectancy >10 years, clinically organ-confined disease (cT1–cT2), biopsy Gleason score ≤7, total serum prostate-specific antigen (PSA) ≤10 ng/mL, and normal preoperative continence and potency. Men with a high-risk, cN1 or M1 prostate cancer (according to the National Comprehensive Cancer Network [NCCN]), pre-existing urinary incontinence, any previous prostatic, urethral, or bladder neck procedure, or neoadjuvant therapy were excluded.
Based on the observed treatment effect of a 30% higher UC rate in the APR vs RS approach, at power 0.80, alpha level 0.05, and cohen d (above 0.50), the sample size for our study was calculated to be 80 patients (40 patients in each arm). The sample size was obtained by means of G Power software (verison 3.1.9.7).
Outcome assesment
The CONSORT-PRO were followed guidelines for patient-reported outcomes. 11 The main goal of the study was to compare functional outcomes. The UC recovery rates were evaluated at the catheter removal, and subsequently at 1, 3, 6, and 12 months after operation. Postoperative potency was evaluated at 3 and 12 months after surgeries. Secondary outcomes were the comparisons of postoperative complication rates, positive surgical margin (PSM), and 1-year oncological outcomes.
Preoperative UC was assessed as documented by the International Continence Society male short-form questionnaire, 12 and postoperative UC was assessed by International Consultation on Urinary Incontinence on Male Lower Urinary Tract Symptoms and International questionnaire. Beginning the day after removal of the catheter, the number of pads per day of all patients was recorded. Postoperative continence was defined as patient-reported use of 0 pads/one security pad per day. All patients were routinely given tadalafil 5 mg during the first 2 months after operation. Afterward, the use of tadalafil was administered on demand. Potency was defined as an erection sufficient for penetrative intercourse and was also assessed by the International Index of Erectile Function-5 (IIEF-5) questionnaire.
Procedure-specific postoperative complications occurring both in the inpatient and outpatient setting were recorded. Oncological outcomes were the presence of a PSM and the rates of a biochemical recurrence at 1-year follow-up. The data were collected and stored by an independent database manager, and the surgeon, surgical team, and postoperative care team were unaware of the data files.
Surgical technique
The primary surgeon (K.T.) had experience of over 500 urological robotic procedure cases at a high-volume reference center. The study compares the cases performed with each technique in the initial experience of the surgeon (i.e., after <50 cases for each technique). Bilateral nerve-sparing approach was performed in all patients in both groups. The key steps of the RS-RARP approach were similar to those described by Galfano et al. 3,13
In the APR-RARP approach, the extraperitoneal space was entered through an inverted, U-shaped incision on the parietal peritoneum, superior to the dome of the bladder and lateral to the medial umbilical ligaments. Then the bladder was dissected off the anterior abdominal wall to enter into the space of Retzius. Both endopelvic fascia were opened. Before the urethravesical anastomosis and reconstructive phase, the anterior supporting structures such as the puboprostatic ligament complex, the arcus tendineus, and detrusor apron, and the bladder neck were preserved (Fig. 1). The urethral length was also maximized during apical dissection of the urethra.

Before the reconstructive phase, preservation of anterior supporting structures such as puboprostatic ligaments and arcus tendineus, and bilateral neurovascular bundle
The posterior reconstruction was performed in a single layer by using a 2/0 “vicryl” suture. The supporting structures lying in the dorsal to the bladder neck and urethra were approximated and a posterior support was recreated for urethra and the urethrosphincteric complex. The layer involved the bladder neck (excluding the mucosa of the bladder) and the posterior aspect of the rhabdosphincter (Fig. 2).
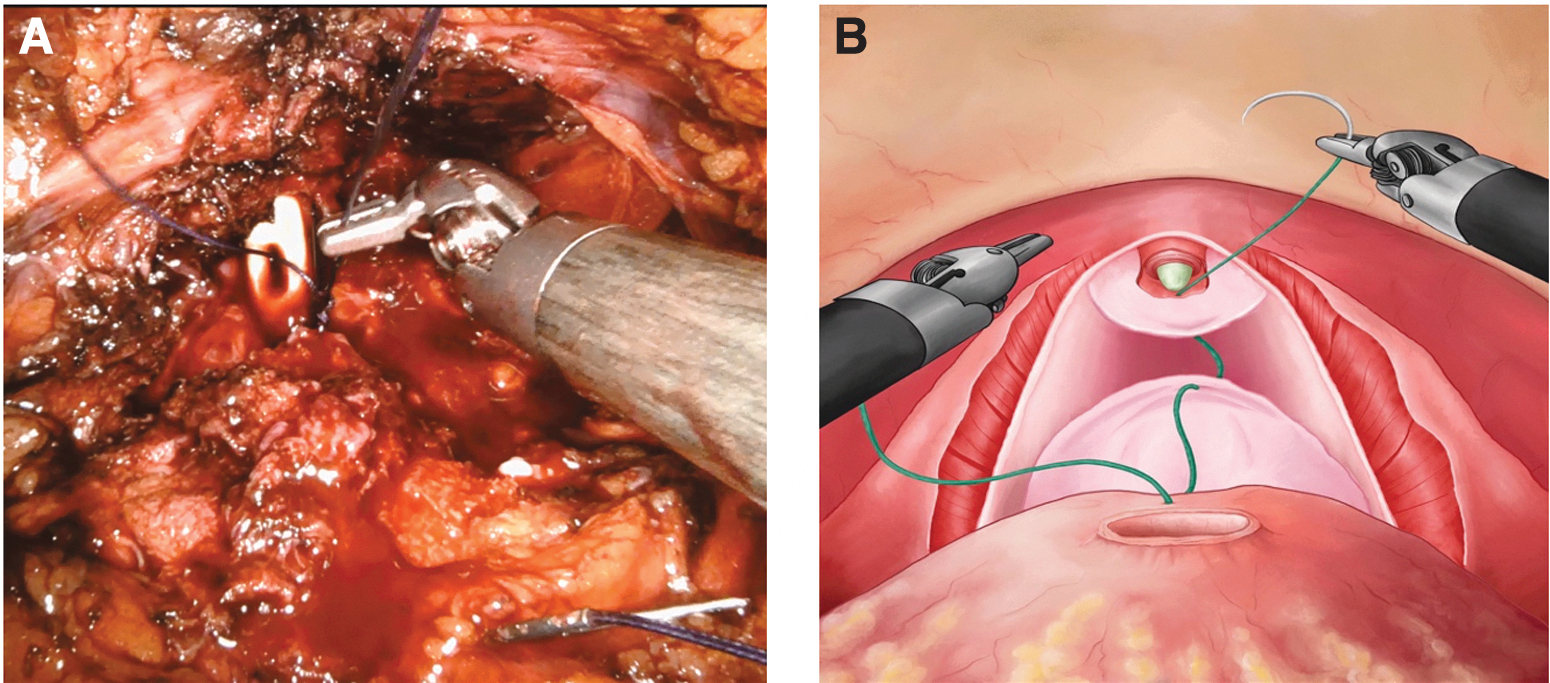
The posterior reconstruction is performed in a single layer by using a 2/0 “vicryl” suture. The layer involves the bladder neck (excluding the mucosa of the bladder) and the posterior aspect of the rhabdosphincter.
After this posterior reconstruction, vesicourethral anastomosis was performed by using a 3/0 “barbed” running suture and was followed by anterior reconstruction.
After preservation of the anterior supporting structures such as the puboprostatic ligaments and the arcus tendineus, and after performing a posterior reconstruction, the arcus tendineus and the puboprostatic ligaments were reattached to the anterolateral distal bladder (Fig. 3A, B), and the bladder was realigned to the pelvic sidewalls to recreate the endopelvic fascia. The original anatomy was restored as much as possible and anterior reconstruction was completed (Fig. 3C, D).

Anterior reconstruction.
Statistical analysis
IBM SPSS® Statistics version 25 was used for statistical analysis. Independent samples t test for normal distribution independent variables, Mann–Whitney U test for independent variable non-normal distribution, and Chi-square and Fisher's exact test to compare categorical data were used between the two study arms. Continence rates were calculated by Kaplan–Meier curves; log-rank test was used for the curve comparison. Patients who did not achieve continence at the end of their observation were considered censored. p Values of <0.05 in the 95% confidence interval (CI) were considered statistically significant.
Compliance with ethical standards
Ethical approval: the study protocol of this prospective study is approved by our institutional ethics committee (registration number; I1-53-21) and is in accordance with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Informed consent: all participants have given informed consent before inclusion in this study.
Clinical Trials Identifier: NCT05224024.
Results
Totally, 89 patients were enrolled to the study, and data of 80 consecutive and eligible patients were randomized. The flow chart displaying the progress of all participants through the trial (according to the CONSORT statement 11 ) is given in Figure 4.
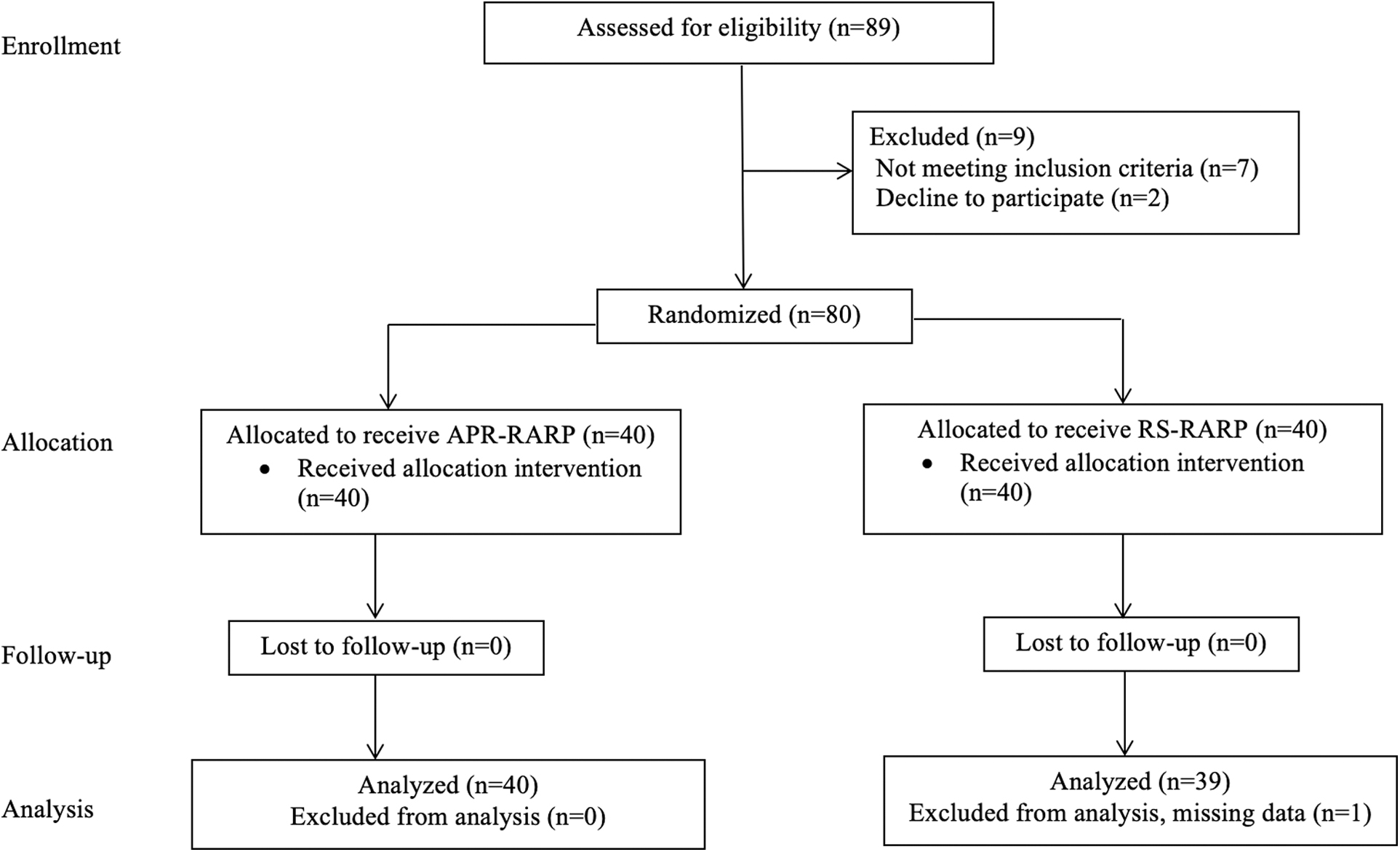
Flow chart illustrating the patient selection process through the trial according to the CONSORT statement. APR-RARP = modified anatomical structure preserving and Retzius-repairing robotic-assisted radical prostatectomy; RS-RARP = Retzius-sparing robotic-assisted radical prostatectomy.
As shown in Table 1, no statistically significant difference was observed between the two groups in terms of preoperative age, PSA, biopsy Gleason score, and clinical stage. As shown in Table 2, the two compared approaches, in terms of rate of complications, PSM, pathologic data (Gleason score and stage), and biochemical recurrence rates, were similar. The mean operation time was slightly longer in the RS-RARP group compared to ARP-RARP, but it was not statistically significant (p = 0.066). The postoperative potency was also similar between the two techniques at 3 months and 1 year.
Demographic and Clinical Variables for Patients Undergoing Modified Anatomical Structure Preserving and Retzius-Repairing or Retzius-Sparing Robot-Assisted Radical Prostatectomy
Student's t, Mann–Whitney UI, and Chi-square tests.
APR-RARP = modified anatomical structure preserving and Retzius-repairing robot-assisted radical prostatectomy; IQR = interquartile range; PSA = prostate-specific antigen; RS-RARP = Retzius-sparing robot-assisted radical prostatectomy; SD = standard deviation.
Perioperative, Postoperative Outcome, and Pathological Data for Patients Undergoing Modified Anatomical Structure Preserving and Retzius-Repairing or Retzius-Sparing Robot-Assisted Radical Prostatectomy
Student's t, Mann–Whitney U, Chi-square, and Fisher's exact tests.
PSM = positive surgical margin; UC = urinary continence.
Comparison of UC rates
No urinary fistula was observed in any patient, and urinary catheters were removed at 7–9 days after operation in all patients. UC recovery in function of time is demonstrated for both groups in Figure 5 from the catheter removal to 360 days after RARP.

Kaplan–Meier curve showing the recovery of UC (defined as 0 pads/one security pad per day) in patients undergoing APR-RARP and RS-RARP. CI = confidence interval; UC = urinary continence.
At the catheter removal and 1, 3, and 6 months after operation, 21/40 (52.5%) ([CI]95% 37.6–67%), 33/40 (82.5%) ([CI]95% 70.8–94%), 38/40 (95%) ([CI]95% 88.3–99.1%), and 39/40 (97.5%) ([CI]95% 92.5–99.9%) of men undergoing the APR-RARP were continent compared with 24/39 (61.5%) ([CI]95% 46.5–76.6%), 35/39 (89.7%) ([CI]95% 80.3–98.1%), 38/39 (97.5%) ([CI]95% 92.6–99.9%), and 38/39 (97.5%) ([CI]95% 92.6–99.9%) undergoing the RS-RARP, respectively, and the comparison of the two curves showed no statistically significant difference for both technique at any time point (log-rank test p = 0.556). The median (95% CI) time to UC recovery was 9.8 (5.2–14.4) days for the APR-RARP vs 6.7 (3.2–10.2) days for the RS-RARP group.
Discussion
One of the major functional problems after RARP is urinary incontinence and the time until complete dryness is an important problem for men. 14 Early postoperative urinary incontinence is the challenging period with the highest rates of urinary incontinence-associated discomfort for men after RARP. 15,16 Owing to that, the quality of life of men is prominently adversely affected because of the early postoperative UC. 17
In pathophysiology of postprostatectomic incontinence, biological factors such as age, BMI, preoperative LUTS, and prostate size, as well as anatomical factors such as external sphincter complex integrity, bladder neck, and stability of membranous urethral support structures are important. 18 The anatomical and functional mechanisms that cause urinary incontinence after RARP are not completely known. Urinary incontinence is thought to occur as a result of changes in structures supporting continence such as the bladder neck, urethra, and sphincter complex after operation, inability to resist intra-abdominal pressure. Therefore, surgical reconstruction of the pelvic floor structures is aimed to provide UC support similar to the presurgical state.
In the last 10–15 years, different surgical techniques have been defined in RARP to recovery UC and increase the quality of life of patients. The most important technique defined in this process is RS-RARP, which is defined by Galfano et al., in which the Retzius is anatomically preserved. 3 In this technique, it is approached exclusively through the douglas space and anatomical integrity, including the neurovascular bundles, is comletely preserved. Since the significant advantage of RS-RARP on early postoperative UC recovery has been demonstrated, many studies in the literature focused on the comparison of the standard and RS-RARP technique. 19
However, most surgeons have not changed their habits regarding the RARP and therefore many different standard-modified approaches have been defined to enhance urinary function recovery. 7 –9,20 –22 These techniques that can be summarized in three categories are preservation (bladder neck, neurovascular bundles, puboprostatic ligaments, functional urethral length etc.), reconstruction (total, anterior, and posterior), and reinforcement. 23 Although different standard-modified approaches have been described, their common goal was to recovery early postoperative UC and urinary function.
The modified anterior approach we used in our study has a similar procedure to the technique described by Tewari. 8 These techniques, characterized by the reconstructive strategy of the anterior and posterior compartment structures of the Retzius space, which plays an important role in UC mechanism, are associated with an enhanced UC and urinary function recovery. 24 In the recently described hood technique, the detrusor apron, puboprostatic ligament complex, arcus tendineus, and endopelvic fascia tissues are preserved after prostate removal. 25 The only difference in our technique from the hood technique is that the endopelvic fascia is incised. Incision of the endopelvic fascia may be preferred owing to the ease of surgical field it provides in lateral access to the prostate. The endopelvic fascia has an indirect positive effect on the UC mechanism owing to its fascial continuity.
Therefore, we opinion that if the endopelvic fascia is opened, it should be repaired after prostate removal. Certainly, performing a prostatectomy with preservation of the endopelvic fascia provides better outcomes for postoperative UC recovery. But, if the endopelvic fascia is opened, its fixation to the preserved puboprostatic complex by reconstruction and ensuring continuity with the puboprostatic complex can restore the original anatomy of the pelvic floor and vesicourethral angle, and this makes a significant contribution to early UC.
However, the main limitation of these prospective studies is the lack of direct comparison between standard-modified approaches and RS-RARP and the lack of high-evidence studies with a randomized design. Therefore, we designed an RCT to compare the urinary function outcomes of both techniques and we think that our current analysis generates important findings worth discussing. To our knowledge, this is the first study to represent level 1 evidence comparing the APR-RARP vs RS-RARP approach.
In our study, UC rates at the catheter removal were 52.5% and 61.5% for APR-RARP and RS-RARP, respectively, and these rates increased to around 85% and 95% at 1 and 3 months, respectively, in both techniques. Although there was a slight advantage in RS-RARP at the catheter removal, there was no difference in UC rates between the two approaches, neither early nor at 1-year follow-up. The comparison of Kaplan-Meier curves regarding postoperative UC rates showed no statistically significant difference at all time points after RARP for both techniques. However, the standard approach is inferior to the RS regarding early continence recovery, 26,27 with the Retzius-repairing technique continence rates similar to RS being achieved, including in the early postoperative period. This is an outcome that should not be ignored for surgeons.
Our overall urinary function results were comparable in both arms and results were similar. It has been shown that the most important criteria of reduction in urinary bother symptoms after RARP is UC recovery and UC recovery time. 15,16,27 Therefore, the primary goal of the surgical approach should be to achieve UC to provide the better urinary function. Although RS-RARP is a more natural and complete preservation of bladder neck, our findings demonstrated that APR-RARP performed with the Retzius reconstruction strategy had similar UC rates. This result offers an important alternative for surgeons who have difficulties in the RS-RARP technique.
In our study, there was no significant difference in erectile function results at 3 and 12 months in both arms. The current literature lacks comparative data regarding sexual function recovery, and cumulative analysis is not feasible. Only Menon et al. reported in their study, 28 comparing the standard approach and RS-RARP, that there was no difference between the two techniques in erectile function results at 3 and 12 months, and potency rates in our study were consistent with data published by the Menon et al.
Postoperative complication rates were similar in both arms (10% in APR-RARP and 10.4% in RS-RARP) and lymphocele was the most common complication (6/80; 7.5%). These rates were similar to the results previously reported in other studies. 29,30 Although the overall PSM ratio was higher in the RS-RARP arm, there was no statistically significant difference (12.8% vs 10%). As a matter of fact, the probability of biochemical recurrence rates were similar between the two arms at 1-year follow-up. However, a longer follow-up is required in both arms to determine whether PSM rates will transform to worse oncological outcomes.
However, this study is not without limitations. First, the number of patients in our study was relatively small and consisted of highly selected patients. Second, the study was limited by subjective assessment of the number of pads. Third, this was a single surgical team study performed at an academic institution and the results should be interpreted in this context. Finally, it should be borne in mind that the most important critical step during prostatectomy for early UC is the preservation of critical anatomical and neurological structures such as the membranous urethra and bladder neck, rather than the preservation of anterior anatomical structures. 31,32
On the other hand, our study is remarkable in terms of methodology. In our study, we focused on the results reported by the patient and adhered to the CONSORT-PRO statement, adding more validity to our results. To our knowledge, this study is the first randomized study comparing APR-RARP vs RS-RARP and provides level-1 evidence supporting comparable urinary function results for both approaches.
Conclusion
This analysis confirms that APR-RARP is a safe and feasible alternative to RS-RARP. In selected, eligible, low-intermediate risk PCa patients, surgeons can achieve functional results comparable to the RS technique with the modified reconstructive anterior approach without changing the surgical technique they are used to.
Footnotes
Authors' Contributions
K.T.: project development and article editing. C.A.: data collection, data analysis, and article writing. E.K.: data collection. E.S.: article writing—reviewing and editing.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.