
Abstract
Background:
Urethral stricture is a well-known complication after transurethral prostate surgery (TPS) and it is usually considered an easy-to-treat condition. We aimed to examine characteristics of post-TPS urethral stricture cases that were referred for urethroplasty at our tertiary center.
Methods:
We identified 201 patients with TPS-induced stricture treated with urethroplasty at our institution from 2017 to 2021. First, stricture length and location were evaluated during preoperative assessment. Second, multiple sets of multivariable logistic regression (MLR) analyses were run to assess whether clinical variables were associated with the location of the stricture.
Results:
Median stricture length was 5 cm (4–7). One hundred forty-one (70.1%) patients received previous no-invasive treatments (dilatation and/or direct visual internal urethrotomy). Proximal bulbar urethra was the commonest site for stricture, whereas panurethral stricture (≥10 cm) was diagnosed in 41 (20.4%) patients. Lichen sclerosus was more common in patients with penile stricture location, compared with patients with other involved segments (26% vs 19%, p = 0.03), and it was the only predictor of penile and midbulbar urethra location at MLR. Surgical approaches were augmented urethroplasty in 94% of patients, especially for patients with previous treatment including urethroplasty (95.8% vs 82.5% for naive, p = 0.004). Dorsal onlay was the preferred approach for bulbar (53.4%) and penile urethra (90.7%), whereas ventral onlay (38.2%) and double face augmentation (20.6%) were the preferred approaches in membranous strictures.
Conclusions:
Most patients who were referred for TPS-induced stricture attempted previous noninvasive managements. Referred TPS-induced urethral strictures were long and frequently involving multiple segments of urethra. Augmentation urethroplasty was our preferred surgical approach because of the characteristics and complexity of these strictures. The presence of lichen may increase the risk of post-TPS stricture in a specific segment of urethra, namely the penile and midbulbar urethra.
Introduction
Urethral stricture is a well-known and dreadful complication after transurethral prostate surgery (TPS). According to a systematic review, the incidence of urethral stricture after TPS ranges from 4.5% to 13%. 1 The suggested etiologic factors linked to the stricture formations are mechanical trauma, prolonged indwelling catheter time, infection, the temperature of the irrigation solution, mucosal rupture during preliminary cystoscopy, and electrical injury by a stray current. 2 –4 The majority of available studies agree that the commonest sites for stricture formation are the junction between the bulbar and the membranous urethra or the fossa navicularis. 5
The management of post-TPS urethral stricture is generally faced by the treating endourologist who performed the TPS. Thus, lack of expertise in urethral surgery and refusing to acknowledge one's own mistake frequently lead endourologists to minimize this pathologic condition preferring endoscopic managements such as direct visual internal urethrotomy (DVIU) or dilatation over urethroplasty. However, these techniques are valuable options only for short bulbar urethral stricture (<2 cm), and they should not be repeated after previous failure.
Given the success rate of 8% of DVIU or dilatation as reported by Santucci and Eisenberg, 6 the largest number of patients with post-TPS stricture, treated with endoscopic procedures, will end up with a recurrent stricture that is frequently more complex than right after TPS. 7 From a referral center perspective, the characteristics of post-TPS urethral stricture are frequently different from those commonly reported in the literature of a short urethral stricture located either at the bulbomembranous junction or at the fossa navicularis. In our experience, patients referred for post-TPS urethral stricture frequently present long strictures involving different segments of the urethra.
Thus, the aim of this study was to evaluate post-TPS urethral stricture according to location and characteristics based on our large case series of patients referred for urethroplasty. In addition, we assessed possible etiologic factors that might be involved and favoring stricture formation in TPS patients worsening the characteristics and location of the stricture. Finally, we described the surgical techniques for stricture repair adopted at our center in view of the location of the stricture.
Materials and Methods
Study population
We retrospectively collected data on patients who underwent urethroplasty for TPS-induced urethral stricture, between January 2017 and December 2021 at our center. Local committee approved this retrospective study. For TPS we considered transurethral resection or transurethral enucleation of the prostate. As per our internal protocol, all patients with urethral stricture underwent an extensive work-up 8 : (1) physical examination to assess the status of the external genitalia, the status of the penile and preputial skin, and the status of the buccal or lingual mucosa; (2) uroflowmetry, retrograde and voiding urethrography, and urethroscopy with small caliber ureteroscope (4.5F/6.5F) to assess the severity of the stricture 9 ; and (3) urodynamic test for those with suspected underactive bladder.
Eligible patients were treated at our institution with urethroplasty, those receiving only endoscopic or conservative management were excluded (N = 12). Patients with known stricture at the time of TPS were excluded from the study as TPS was not the etiologic factor (N = 7). Moreover, lack of retrograde/voiding urethrography or recorded video of urethroscopy performed at our center was also considered reason for exclusion (N = 13). Finally, patients with isolated bladder neck stenosis were also excluded (N = 9), even if we recognize that bladder neck stenosis is also a common complication after TPS. 10 Overall, we identified 201 patients with TPS-induced stricture (Fig. 1).

Flow chart depicting inclusion and exclusion criteria of the cohort study. TPS = transurethral prostate surgery. Color images are available online.
Variables of interest
For each included patient, retrograde and voiding urethrography and recorded video of urethroscopy were independently examined by three reconstructive urology fellows (M.B., C.Y., D.N.) to assess the exact location of the stricture. Discordant interpretations were jointly reviewed with an experienced reconstructive urology (P.M.J.). For representation purpose, the urethra was classified into seven segments: meatus and fossa navicularis, penile urethra, distal bulbar urethra, midbulbar urethra, proximal bulbar urethra, membranous urethra (including the bulbomembranous junction), and bladder neck.
The length and location of the stricture were established based on retrograde/voiding urethrography (Fig. 2) and recorded urethroscopy. Stricture features and patient characteristics such as age at the time of surgery, history of diabetes, history of cardiovascular disease (CVD), use of tobacco, presence of lichen sclerosus, previous treatment for urethral stricture (DVIU, dilatation or urethroplasty), time from TPS to urethroplasty, and radiologic length of the stricture were collected. The surgical technique for urethroplasty, as well as the use of graft or flap, was also annotated for each patient and compared according to the location of the stricture.
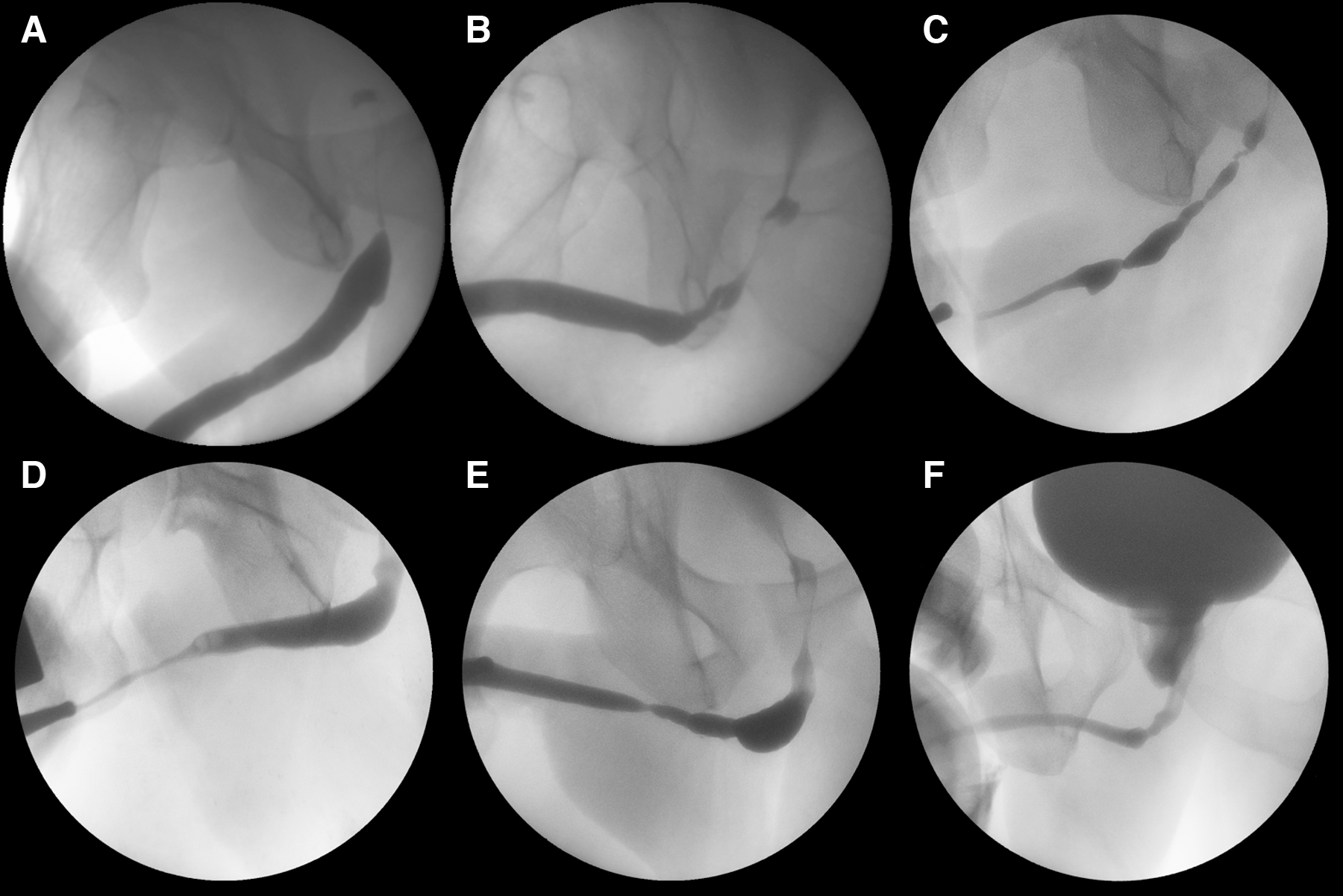
Examples of stricture location:
Surgical techniques for augmented urethroplasty were previously described. 11 –15 We also defined two additional variables, such as panurethral stricture and multiple segments of urethra involved. For panurethral stricture, we considered those strictures longer than 10 cm according to the European Association of Urology definition. 16 When two or more of the seven urethral segments were involved, we defined that stricture as involving multiple segments.
Statistical analyses
Descriptive analyses were based on standard methods. For comparisons between the groups, chi-square test, Fisher's exact test, and Kruskal–Wallis test were employed, as appropriate. Multiple sets of multivariable logistic regression (MLR) analyses were run to assess whether clinical variables (diabetes, tobacco, CVD, lichen sclerosus, previous treatment, time from TPS surgery, and age) were associated with the location of the stricture. All statistical tests were two sided with a level of significance set at p < 0.05. Analyses were performed using the R software (version 3.6.1; R Foundation for Statistical Computing, Vienna, Austria).
Results
In the past 5 years, we performed 201 urethroplasty for post-TPS urethral stricture (Table 1). No patients received radiation. Median (interquartile range) age at surgery was 67 years (62–73). One hundred ninety-two patients received transurethral resection of prostate and nine received holmiun laser enucleation of prostate. Time from TPS to urethroplasty was 23 months (11–48). Patients presenting with diabetes, CVD, and lichen sclerosus at the time of urethroplasty were 71 (35.3%), 33 (16.4%), and 45 (22.4%) patients, respectively. Median stricture length was 5 cm (4–7).
Preoperative Characteristics of Patients Who Underwent Urethroplasty for Transurethral Prostate Surgery Induced Urethral Stricture at Our Tertiary Center
CVD = cardiovascular disease; IQR = interquartile range; TPS = transurethral prostate surgery.
Before urethroplasty, 144 (71.6%) patients received previous treatments, of those 141 (70.1%) received noninvasive (DVIU or dilatation) treatment. In detail, 66 (32.8%) received dilatation, 51 (25.4%) were on regular clean intermitted catheterization, 90 (44.8%) received DVIU, and 10 (5%) attempted urethroplasty (Table 2). Suprapubic or transurethral catheter was present in 34 (16.9%) patients. Proximal bulbar urethra (65.7%) was the commonest site for stricture in our cohort, followed by penile (42.8%), mid- (41.3%), and distal bulbar location (41.8%) (Fig. 3). Panurethral stricture was diagnosed in 41 (20.4%) patients.

Radar plot depicting location distribution of urethral strictures in our cohort. Color images are available online.
Type of Previous Treatment in the Overall Cohort of Patients Treated with Urethroplasty for Post-Transurethral Prostate Surgery Urethral Stricture
Previous treatments included DVIU, urethroplasty, and dilatation.
CIC = clean intermitted catheterization; DVIU = direct visual internal urethrotomy.
When considering association between stricture length and location, we found that the involvement of the meatus/fossa navicularis, penile urethra, distal, and midbulbar urethra were more common in patients with considerably longer strictures (median length: 12, 8.5, 7.5, and 7 cm, respectively; Table 3), as compared with proximal bulbar (5 cm) and bulbomembranous (5 cm) segments. Rate of penile stricture was higher in patients with lichen sclerosus than with other segments (26% vs 19%, p = 0.03). No significant differences were noticed for patients with or without previous treatment according to stricture location (all p > 0.05).
Association Between Urethral Stricture Length and Location of the Stricture
Values in bold are those statistically significant.
On MLR analyses, presence of lichen sclerosus was associated with a higher risk of urethral stricture location in penile [odds ratio (OR) 2.24, 95% confidence interval (CI) 1.11–4.63, p = 0.03] and midbulbar urethra (OR 1.19, 95% CI 0.61–2.34, p = 0.02) after TPS. None of the other clinical variables was associated with particular stricture location (Table 4). Surgical approaches were augmented urethroplasty in 189 (94%), anastomotic urethroplasty in 2 (1%), Johannson urethroplasty in 5 (2.5%), nontransecting anastomotic urethroplasty in 3 (1.5%), and perineal urethrostomy in 2 (1%) patients.
Multivariable Logistic Regression Analyses Assessing Predictors of Urethral Stricture Location After Transurethral Prostate Surgery
Values in bold are those statistically significant.
CI = confidence interval; OR = odds ratio.
Augmented urethroplasty was also the preferred approach in patients with previous treatment as compared with patients without previous treatments (95.8% vs 82.5%, p = 0.004). Dorsal onlay was the preferred approach for bulbar (87, 53.4%) and penile urethra (78, 90.7%). Ventral onlay was the preferred approach in membranous urethra (26, 38.2%). Double face augmentation was more frequently required in membranous strictures (14, 20.6%). Examples of reconstruction are shown in Figure 4A to C.

Discussion
Urethral stricture is potential complication of TPS surgery, which requires an accurate diagnostic and therapeutic pathway to reach the best functional outcome, while reducing its recurrence after initial treatment. In this context, the findings observed in this study provide an objective and evidence-based foundation for clinical and surgical management of patients with urethral stricture after TPS referred to a tertiary care center.
First, we highlighted that the assessment of stricture location and severity is mandatory during preoperative decision making even for post-TPS urethral stricture. In this context, we previously reported on the efficacy of urethroscopy with small caliber ureteroscope (4.5F/6.5F), together with uroflowmetry and retrograde and voiding urethrography as useful landmark for treatment decisions. 9 Indeed, we found that bulbar urethra is the commonest location involved by TPS-induced strictures as also previously reported by different retrospective studies. 4 However, we highlighted that every segment of the urethra could be ideally damaged during TPS, with up to 20.4% of patients suffering from panurethral disease.
Second, we found that despite the greatest portion (71.6%) of patients suffering from TPS-related stricture was previously treated with no-invasive approaches, the median stricture length was 5 cm (4–7) at time of diagnosis. These data highlight that post-TPS urethral stricture is not always an easy-to-treat condition because of its characteristics, frequently different from those commonly reported in the literature. 17 Furthermore, even though endoscopic or no-invasive treatments are the preferred options, 18 especially as first option, previous treatments could also interfere in worsening stricture degree. 7
Third, the rate of penile stricture was higher in patients with lichen sclerosus diagnosis than in patients with other urethral segments. Furthermore, patients with lichen sclerosus had a higher risk of penile and midbulbar location of urethral stricture after TPS than patients with other urethral sites. According to these data, we speculated that together with the well-known risk factors associated with post-TPS urethral stricture development, such as monopolar energy, instrument caliber, and duration of postoperative catheterization, 17 lichen sclerosus could play a role in urethral stricture evolution and location. 19 Thus, histologic analysis for lichen sclerosus should be recommended especially for those patients suffering from recurrent urethral stricture in the anterior urethra after TPS. 20
Finally, most (94%) of patients in our cohort were treated with augmented urethroplasty, which was also the preferred approach in patients who underwent previous treatment. For bulbar and penile urethra strictures, dorsal onlay urethroplasty was mostly used, whereas ventral onlay or double face augmentation techniques were the preferred options for membranous urethra strictures. 21 Taken together, these data focus on the importance of referring patients suffering from post-TPS urethral stricture to surgeons with high expertise on its management to suit the treatment to the characteristics and location of the stenosis, regardless of its etiology.
Our study had inherent limitations owing to its retrospective nature. Furthermore, despite our findings are based on a large series of patients treated with urethroplasty for post-TPS urethral stricture, it derives from a cohort of referred patients that does not represent an objective picture of the general population. Nevertheless, we demonstrated that post-TPS stricture can be a more complex condition than previously expected, requiring a high level of expertise to be dealt with best.
Conclusions
Urethral stricture after TPS is not always an easy-to-treat condition as it could show poor characteristics and ideally involve every segment of the urethra. Thus, patients should be aware on the possible high risk of recurrence after no-invasive treatment and surgeons should refer patients to high specialized centers.
Footnotes
Authors' Contributions
M.B., P.M.J., and S.B.K. contributed to protocol/project development. M.B., C.Y., P.M.J., D.N., S.B., A.A., and S.B. were involved in data collection or management. F.M., P.M.J., and S.B.K. oversaw project supervision. M.B. and G.B. carried out article writing/editing.
Author Disclosure Statement
The authors have no relevant financial or nonfinancial interests to disclose.
Funding Information
No funding was received for this article.