
Abstract
Objective:
To evaluate the effects of CO2 pneumoperitoneum on venous hemodynamics and cardiopulmonary function during transperitoneal or retroperitoneal laparoscopic surgery.
Materials and Methods:
A single-institution prospective study. Forty-three patients with renal-cell carcinoma undergoing retroperitoneal (22) or transperitoneal (21) laparoscopic partial nephrectomy were enrolled. Hemodynamic functions were monitored by minimally invasive FloTrac/Vigileo system. Transesophageal echocardiography was used to measure the diameter and blood flow of the inferior vena cava (IVC). Measured parameters were recorded at baseline, 10, 30, 60 minutes following insufflation to 14 mm Hg and 10 minutes following desufflation.
Results:
For hemodynamic changes in the transperitoneal laparoscopic surgery (TPL) and retroperitoneal laparoscopic surgery (RPL), transperitoneal CO2 insufflation resulted in a rapid parallel increase in central intravenous pressure (CVP), peak airway pressure (AWP), and IVC blood flow velocity after the first 30 minutes of pneumoperitoneum (p < 0.05). In contrast, CVP, AWP, and IVC blood flow velocity increased progressively in RPL. The variation of those parameters was significantly lower than that of TRL (p < 0.001; p = 0.002; p = 0.004). The mean maximum CVP in the two groups was 20 and 16 mm Hg, respectively. The IVC diameter at the cavoatrial junction was significantly reduced in TPL after 10 minutes of insufflation, but it remained unchanged in RPL throughout the surgery. For cardiopulmonary function changes, heart output decreased after a short period of pneumoperitoneum, but no statistical differences were observed between the two groups. The increments of partial pressure of arterial carbon dioxide and end-tidal carbon dioxide tension were significantly higher in RPL than TPL (p < 0.001; p < 0.001).
Conclusions:
Compared with retroperitoneal pneumoperitoneum, transperitoneal pneumoperitoneum has significant effects on IVC hemodynamics. Elevated intra-abdominal pressure (IAP) causes higher AWP and venous return resistance, which lead to the significant increase of CVP during transperitoneal approach. Adjusting the balance between IAP and CVP might be an effective way to control intravenous bleeding.
Clinical Trial Registry:
Registration number: ChiCTR2000038291.
Introduction
Minimally invasive surgery has become the gold standard of surgical management for T1 renal-cell carcinoma. Its advantages over open surgery include less postoperative pain and ileus, faster convalescence, and better cosmesis. There are two approaches that have been investigated widely for renal surgery, including transperitoneal laparoscopic surgery (TPL) and retroperitoneal laparoscopic surgery (RPL).
Several studies have compared the advantages and disadvantages of the two surgical approaches. Those comparative studies suggested that RPL might have advantages over TPL in operating times and estimate blood loss (EBL). 1 –3 Our previous study has confirmed that retroperitoneal inferior vena cava (IVC) thrombectomy tended to have less EBL compared with the transperitoneal group. 4 Meanwhile, we observed that the morphology of IVC was more shriveled and collapsed in retroperitoneal surgery. It indicates that these two procedures might have different hemodynamic effects. Although the changes of cardiopulmonary function during transperitoneal or RPL have been described, 5 –7 little is known about the impact of CO2 insufflation on venous hemodynamics through different pneumoperitoneum models.
In this study, we conducted a prospective clinical research to explore the effect of pneumoperitoneum on venous hemodynamics and cardiopulmonary function during laparoscopic surgery. It could help comprehensively understand the relationship between different pneumoperitoneum approaches and EBL, which may guide the reasonable management of intra-abdominal pressure (IAP) and anesthesia in laparoscopic surgery.
Materials and Methods
Patients
After institutional review board approval, this single-institution prospective study was registered in the Chinese Clinical Trial Registry (registration number: ChiCTR2000038291). A total of 43 patients with renal cell carcinoma (RCC) who met the inclusion criteria from September 2020 to July 2022 were eligible for this study. The main inclusion criteria include American Society of Anesthesiologists (ASA) physical status I to II, age older than 18 years, and candidate patients for laparoscopic partial nephrectomy. Exclusion criteria were absolute contraindications to surgery, severe endocrine and hematopoietic diseases, and previous laparoscopic surgery.
Anesthesia techniques
All of the patients were given a conventional general anesthetic regimen. The Diprifusor was used to provide a target-controlled infusion of propofol (Diprivan 1% AstraZeneca Corp), which was based on the Marsh pharmacokinetic model. The propofol was injected at 4 μg/mL until the bispectralindex (BIS) dropped to 60. Rocuronium 0.6 mg/kg and sufentanil 0.3 μg/kg were intravenously administered. BIS decreased to 60, an endotracheal intubation was inserted. Hemodynamic functions were monitored by placing FloTrac/Vigileo. The parameters of mechanical ventilation were as follows: tidal volume 8 to 10 mL/kg, respiratory rate 12 times/min, oxygen concentration 70% to 80%, and PetCO2 35 to 45 mm Hg. Intravenous rocuronium 0.2 mg/kg was administered as needed.
Surgical technique
All patients were operated by three surgeons with >100 cases of laparoscopic surgery experience. The indication for the surgical approach was determined by the surgeon, mainly based on the anatomical characteristics of tumor. In the RPL group, patients were placed in a 90° left lateral decubitus position with overextension. In the TPL group, positioning for these cases was a 45° to 60° modified flank position. The procedure for RPL and TPL was performed using the operating techniques previously described. 8,9 The IAP was maintained at 14 mm Hg with CO2 insufflator throughout the laparoscopic surgery.
Data collection
The minimally invasive FloTrac/Vigileo system was used to monitor hemodynamic parameters, including mean arterial pressure (MAP), heart rate (HR), while central venous catheter was placed to monitor central venous pressure (CVP), and arterial blood gas analysis for PH, arterial carbon dioxide pressure, and arterial oxygen pressure. Transesophageal echocardiography (TEE) was used to measure the IVC diameter (IVCD) and blood flow velocity at the cavoatrial junction to coincide by the end of breath cycle inhalation. Heart capacity-related indicators were also detected by TEE, including cardiac output (CO), stroke volume (SV), and atrial end diastolic volume. Respiratory function-related indicators were recorded from the ventilator, including tidal volume, positive end expiratory pressure, and end-of-breath CO2 pressure (PETCO2). Measured parameters were recorded at baseline, 10, 30, 60 minutes following insufflation to 14 mm Hg and 10 minutes following desufflation.
Statistical analyses
The Shapiro–Wilk test was applied for normality test. Continuous variables are presented as the median (IQR) or median ± SD, depending on whether the data coincided with normal distribution. Categorical variables are presented as the frequency count and percentage. Student's t test or Mann–Whitney U test was applied for the comparisons between each treated group and the control group (based on normal distribution or not). Statistical significance was determined by one-way ANOVA for comparison across treated groups. All statistical analyses were performed with SPSS Statistics software 18.0 (IBM Corp., Armonk, NY), with p < 0.05 considered statistically significant.
Results
Baseline characteristics
A total of 43 patients with RCC met the inclusion criteria followed by retroperitoneal or transperitoneal laparoscopic partial nephrectomy. Twenty-one and 22 patients underwent TPL and RPL, respectively. Baseline patients' characteristics are summarized in Table 1. Compared with the TPL group, the RPL group has lower blood loss (35 vs 50, p = 0.046), and shorter operation time (125 vs 150, p = 0.015). No significant differences were found between the two groups with regard to sex, age, BMI, tumor side, ASA grade, and total intraoperative fluid.
Patient Characteristics
ASA = American Society of Anesthesiologists physical status grade; BMI = body mass index; IQR = interquartile range; RPL = retroperitoneal laparoscopic surgery; TPL = transperitoneal laparoscopic surgery.
Hemodynamic changes before and after CO2 insufflation
The morphology of IVC in both groups is shown in Figure 1. In the TPL group, HR increased significantly after 10 minutes of CO2 insufflation (p < 0.01) and attained a plateau after 30 minutes until the end of surgery. By contrast, HR increased slowly in the RPL group after insufflation (p < 0.05). HR tended to decline to baseline levels in both groups 10 minutes after desufflation (Fig. 2A). Meanwhile, we observed a similar trend in MAP (Fig. 2B). Cardiac output (CO) decreased after a short period of pneumoperitoneum in both groups (p < 0.05). However, the measurements did not show statistical differences at any time point between the two groups.

The morphology of IVC was more shriveled and collapsed in retroperitoneal group

Effect of CO2 insufflation and deflation on hemodynamics and cardiopulmonary parameters (HR, MAP, CO, CVP, AWP, PaCO2, PetCO2, IVC, blood flow velocity, and IVC diameter). Measured parameters were recorded at baseline, 10min, 30min, 60min, and 10 min following desufflation. Hemodynamic changes before and after CO2 insufflation shown
There was a parallel increase in CVP in both groups during the first 30 minutes of pneumoperitoneum (p < 0.01). After 30 minutes of insufflation, CVP became significantly higher than the baseline level and reached a plateau. It immediately dropped to the baseline level until the pneumoperitoneum disappears. We observed that the increase of CVP in TRL was significantly greater than that in RPL after 10 minutes of CO2 insufflation (confidence interval [95% CI]: 13.41–16.04 vs 17.01–20.61, p < 0.001), and the maximum mean CVP in the two groups was 20 and 16 mm Hg, respectively (Fig. 2D).
Respiratory changes before and after CO2 insufflation
The airway pressure (AWP) in both groups increased significantly after 10 minutes of CO2 insufflation in comparison with the control (p < 0.05). The values were significantly higher in TPL than in RPL at 30 minutes of insufflation (95% CI: 21.51–25.31 vs 25.73–28.93, p = 0.002). They returned to the preinsufflation level after 10 minutes of insufflation relief in both groups (Fig. 2E).
PaCO2 in TPL increased significantly after 10 minutes of CO2 insufflation, then remained increased throughout the procedure (Fig. 2F). It was worth noting that PaCO2 showed a gradual upward trend in RPL, even surpassing TPL after 60 minutes of CO2 insufflation (95% CI: 42.16–47.15 vs 37.71–40.83, p < 0.001). Meanwhile, we observed a similar trend in PetCO2 (Fig. 2G), it increased significantly 10 minutes after CO2 insufflation, respectively (p < 0.01).
IVC blood flow analysis before and after CO2 insufflation
The IVC blood flow velocity significantly increased from a baseline value of 0.40 ± 0.20 m/s before insufflation to 0.94 ± 0.37 m/s after 30 minutes of insufflation in TRL group (95% CI: 0.36–0.60 vs 0.77–1.11, p < 0.001, Fig. 2H). Following desufflation of pneumoperitoneum, the IVC flow rate returned to a near-baseline value of 0.51 ± 0.21 m/s. The same trend was also present in the RPL group, but the variation of blood flow velocity was significantly lower than that of TRL group at 30 minutes of insufflation (95% CI: 0.49–0.76 vs 0.77–1.11, p = 0.004).
The diameter of the IVC was immediately reduced in TRL group after 10 minutes of CO2 insufflation (95% CI: 1.48–1.97 vs 1.0–1.49, p = 0.006, Fig. 2I), but it remained unchanged in RPL throughout the surgery (p = 0.947). The images of IVC hemodynamic changes measured by TEE are shown in Figure 3.
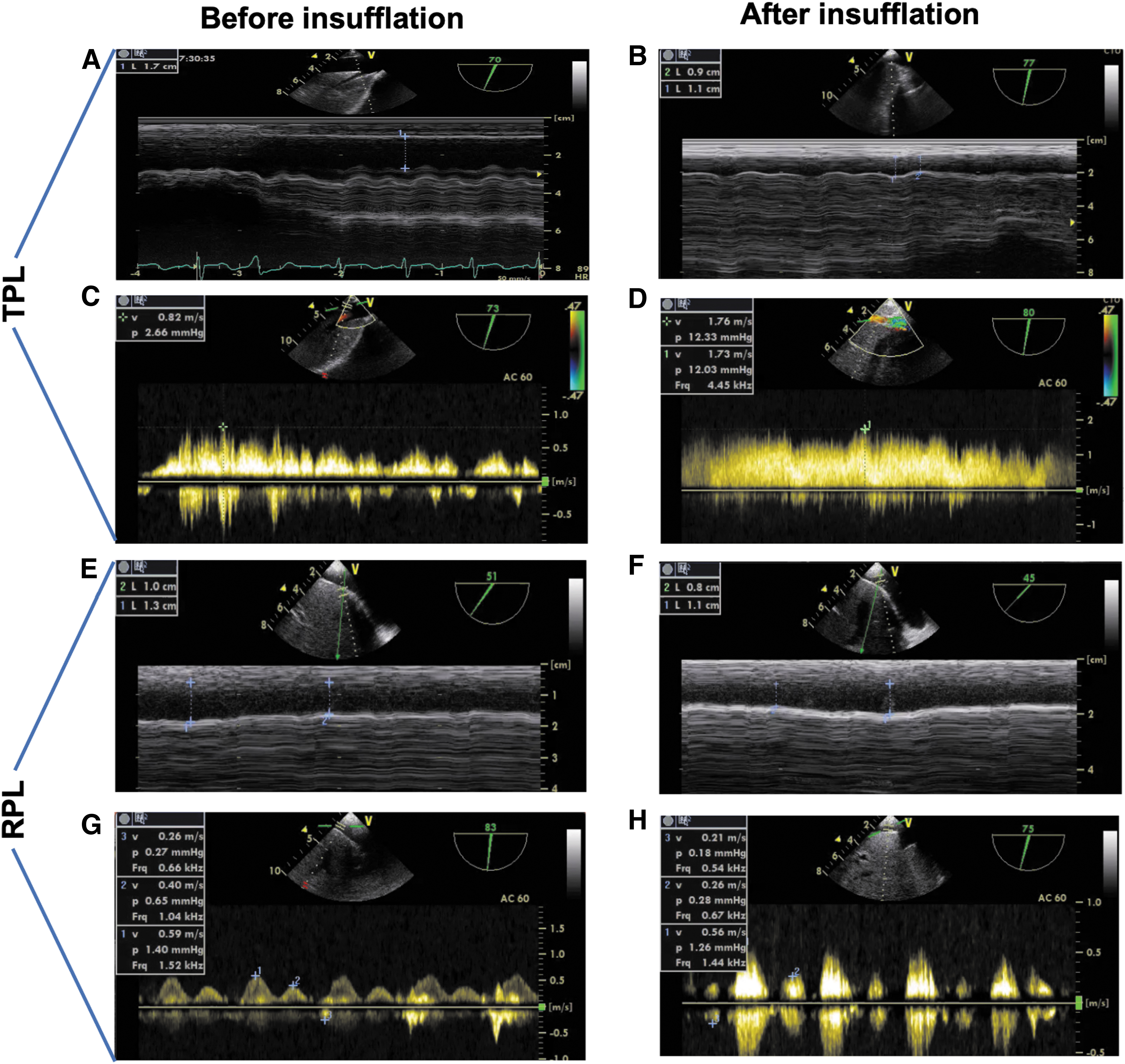
TEE was used to measure the IVC diameter and blood flow velocity at the cavoatrial junction to coincide by the end of breath cycle inhalation. The diameter of the IVC was immediately reduced in TRL group
Discussion
Minimally invasive surgery has become the gold standard of surgical management for T1 renal-cell carcinoma. There are two widely accepted surgical approaches for laparoscopic partial nephrectomy, including transperitoneal approach and retroperitoneal approach. Several studies have compared the advantages of these two procedures. Pavan et al 2 evaluated the perioperative results of transperitoneal and retroperitoneal methods for robot-assisted partial nephrectomy (RAPN) in 886 and 513 patients, respectively, in a systematic review. Significantly shorter operating times and lower EBL were found with the retroperitoneal approach, which is consistent with our research data. In a multi-institutional study, Arora et al 3 compared the results of retroperitoneal and transperitoneal RAPN; EBL was significantly lower in the retroperitoneal group, with 100 mL vs 125 mL, respectively (p = 0.007).
This difference is particularly noticeable in IVC thrombectomy. 4 The reasons for this discrepancy remained controversial and relatively complex, and some scholars believe that the effects of CO2 pneumoperitoneum on abdominal visceral organs and stress response are the causes of the different hemodynamic changes, however, they could not explain why the morphology of IVC appears differently between TPL and RPL.
In this study, we evaluated the effects of pneumoperitoneum on venous hemodynamics and cardiopulmonary function. Under general anesthesia and 14 mm Hg with CO2 insufflator, the increase of HR, MAP, CVP, and AWP was significantly greater in TPL than that in RPL, which indicated that TPL caused much more change in hemodynamics. From the view of pathophysiology, elevated IAP could cause IVC compression and diaphragmatic displacement, which lead to the increase of the AWP and intrathoracic pressure. Finally, these increased pressures were transmitted to the cardiac pericardium and caused venous return resistance and CVP increase. Due to the less impact of retroperitoneal pneumoperitoneum on diaphragmatic displacement and organ compression, the change in venous return resistance was milder than in the TPL.
To confirm our hypothesis, we also used TEE to measure the IVCD and blood flow velocity. Previous studies have confirmed that pneumoperitoneum could decrease IVC blood flow at an IAP of 15 mm Hg. 10 However, no study has described changes in IVC hemodynamics between TPL and RPL. In the TPL group, pneumoperitoneum leads to a decrease in superior diaphragm IVC diameter and an increase in blood flow velocity. Changes in the blood flow of IVC confirmed our previous hypothesis. The increase of intrathoracic pressure caused by elevated IAP results in a decrease in IVC blood flow. Conversely, the change of IVC hemodynamics in RPL was relatively milder, which proves that higher venous return resistance and IVC compression exist in the TPL group.
As previously proved, the main factor influencing intraoperative bleeding from the venous system depends on the pressure gradient between IAP and CVP. 11,12 The mean maximum CVP in TPL was ∼20 mm Hg, which is much higher than that of RPL (16 mm Hg) and standard IAP (14 mm Hg). Higher CVP could lead to venous blood reflux, and undoubtedly increases the risk of bleeding during transperitoneal surgery, compared with retroperitoneal surgery. How to adjust the balance between IVP and CVP seems to be an effective method that can control bleeding from the renal vein and IVC. Kobayashi et al have confirmed that CVP was persistently higher than IAP under high AWP, thus bleeding from the hepatic vein cannot be controlled by increasing IAP under high AWP. 13 Meanwhile, high IAP may increase the risk of gas embolism. 12,14 There is currently no consensus on the optimal IAP for transperitoneal laparoscopic surgery.
Some scholars have studied the feasibility of low pneumoperitoneum pressure laparoscopic surgery, 15,16 however, its effect on bleeding control is still unclear. It remains common practice to use an elevated IAP level to control backflow bleeding from the veins throughout the surgical procedure. As positive correlations were observed between AWP and CVP, dropping AWP to reduce CVP is optional, but a sufficient ventilatory volume must be guaranteed by anesthesiologist. Considering that the patient's age, position, and depth of neuromuscular blockade can all have effects on IAP, the individualized pneumoperitoneum pressure strategy and real-time monitoring might be a rational procedure in the future.
Consistent with previous research, RPL tends to cause much more change in the respiratory measurements. 7 The effect of RPL on respiration is related to the anatomical structure of a retroperitoneal pneumoperitoneum. Separated fat and connective tissue accelerate the absorption of CO2, which cause a high level of PaCO2 and PetCO2 in RPL. If PaCO2 increases too much during surgery, it is necessary to increase minute ventilation. Minute ventilation should be increased by increasing ventilation frequency to prevent a further increase of Ppeak, which would cause further increments of PetCO2. 12
This study has a limitation; due to the interference of pneumoperitoneum, we were unable to measure renal venous reflux through the transbody ultrasound. Intra-abdominal ultrasound could provide more accurate measurements, but this procedure may prolong renal ischemia. Further optimization of measurement procedures was needed to measure renal venous reflux in laparoscopic partial nephrectomy.
In summary, compared with retroperitoneal pneumoperitoneum, transperitoneal pneumoperitoneum has significant effects on IVC hemodynamics. Elevated IAP causes higher AWP and venous return resistance, which lead to the increase of CVP. This will shed new light on intraoperative bleeding control. Adjusting the balance between IVP and CVP might be an effect way to control intravenous bleeding during transperitoneal laparoscopic surgery.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This work was supported by the National Natural Science Foundation of China (Grant Nos. 81970594 and 81970665).