
Abstract
Introduction:
Only 9.9% of practicing urologists in the United States are women. This percentage is even smaller in leadership positions and high-ranking appointments. Endourology is one of the least reported fellowships completed by women urologists. We sought to evaluate how endourologists perceived the climate for women physicians and compare perceptions and experiences of gender equity.
Materials and Methods:
An IRB approved and validated survey, Culture Conducive to Women's Academic Success (CCWAS) questionnaire was sent out to the Endourological Society listserve. Subcategories of equal access, work-life balance, freedom of gender bias, and leadership support were analyzed. An open comment section was provided for respondents to include their own experiences. Wilcoxon rank-sum and Kruskal–Wallis tests were used to compare CCWAS scores between groups.
Results:
A total of 104 completed surveys were received. Response rate was 7% (104/1492), 26.9% of which were female. There was a statistically significant difference between male and female respondent CCWAS scores; p < 0.05. The male CCWAS score median was 196.0 (interquartile range [IQR] 176.75–214.0) vs female CCWAS score median of 166.5 (IQR 127.5–210.0). There was no significant difference in CCWAS scores based on years in practice, parental status, or academic vs private practice.
Discussion:
In this study, male endourologists' perceptions of gender equity were incongruent with the reported experiences of their female colleagues. This indicates that male respondents perceive the culture in their department toward women more positively than their female colleagues. This is suggestive that there are gender-based differences in how gender inequities are perceived and potentially experienced.
Introduction
Urology is a largely male predominant specialty with a notable increase in female representation in recent years. According to the American Urological Association's (AUA) census, female practicing urologists grew to 9.9% in 2019 from 7.7% in 2015 and 9.2% in 2018. 1 While female representation is increasing in the field of urology, it is still lower than the medical trainee population with over half of American medical students being female. 2
In 2021, 141/481 (29%) of matched positions went to women. 3 Urology has experienced the highest growth rate in female representation among all specialties, with urology training programs seeing approximately an 11-fold increase in women from 1978–1982 to 2009–2013 (1.9%–23.1% mean female representation). 4 According to the 2018 AUA Census report, ∼78% and 63% of practicing urologists reported that their practices made efforts to hire women and underrepresented minorities, respectively. 5 As Urology progresses toward equal gender numbers in the workforce, there continues to be large disparities in overall compensation, academic positions, and leadership advancement, particularly in the academic environment for female urologists. 6 –8
Perceptions and experiences of discrimination and inequity may play a role in marginalization of women in academic medicine. A recent study from an Internal Medicine department in Canada revealed that senior male physicians perceive gender equity differently from the reported experiences of the women working in their department. 9 This discrepancy between perceptions and experiences of equity may help explain the persistence of disparities in our field. We are unlikely to change what we do not recognize.
We sought to evaluate the perceptions and experiences of gender equity among Endourologists. We hypothesized that there will be discordance between perceptions of gender equity among male and female endourologists. By better understanding the reported discrepancies, we can seek out actionable items to help promote gender equity and inclusion within the field.
Materials and Methods
This study was approved by the Institutional Review Board, STUDY00020826. An online survey was conducted using the Culture Conducive to Women's Academic Success (CCWAS) questionnaire, a validated instrument designed to measure how conducive the workplace is for women in academic positions. 10 The survey is designed to examine four domains of equity: equal access, work-life balance, freedom from gender bias, and supportive leadership. All items are rated using a 5-point Likert scale. A higher score reflects a perceived favorable environment for women. Additional demographic data were assessed, including gender, years in practice, parental status, and academic appointment. The survey was emailed in two blasts over a 6-week period via the Endourological Society listserve to all active members. The survey was closed 6 weeks after the initial emailed invitation was sent.
Survey results were analyzed using R version 3.6.3. Descriptive analysis was used to summarize respondent characteristics. Surveys with incomplete CCWAS score results were excluded from analysis. The distribution of CCWAS scores were evaluated graphically using histograms and were tested for normality using Shapiro-Wilkes test. Wilcoxon rank-sum and Kruskal–Wallis tests were used for comparison of overall CCWAS score and score in each domain by respondent characteristic groups (gender, years in practice, role, and parental status). p-Values <0.05 were considered statistically significant for these analyses. Graphical analysis by scatterplot was used to elucidate the relationship between faculty gender ratio and overall CCWAS score; however, Pearson's correlation of this relationship was not reported because the independence of respondents from the same department cannot be ensured (Fig. 1).
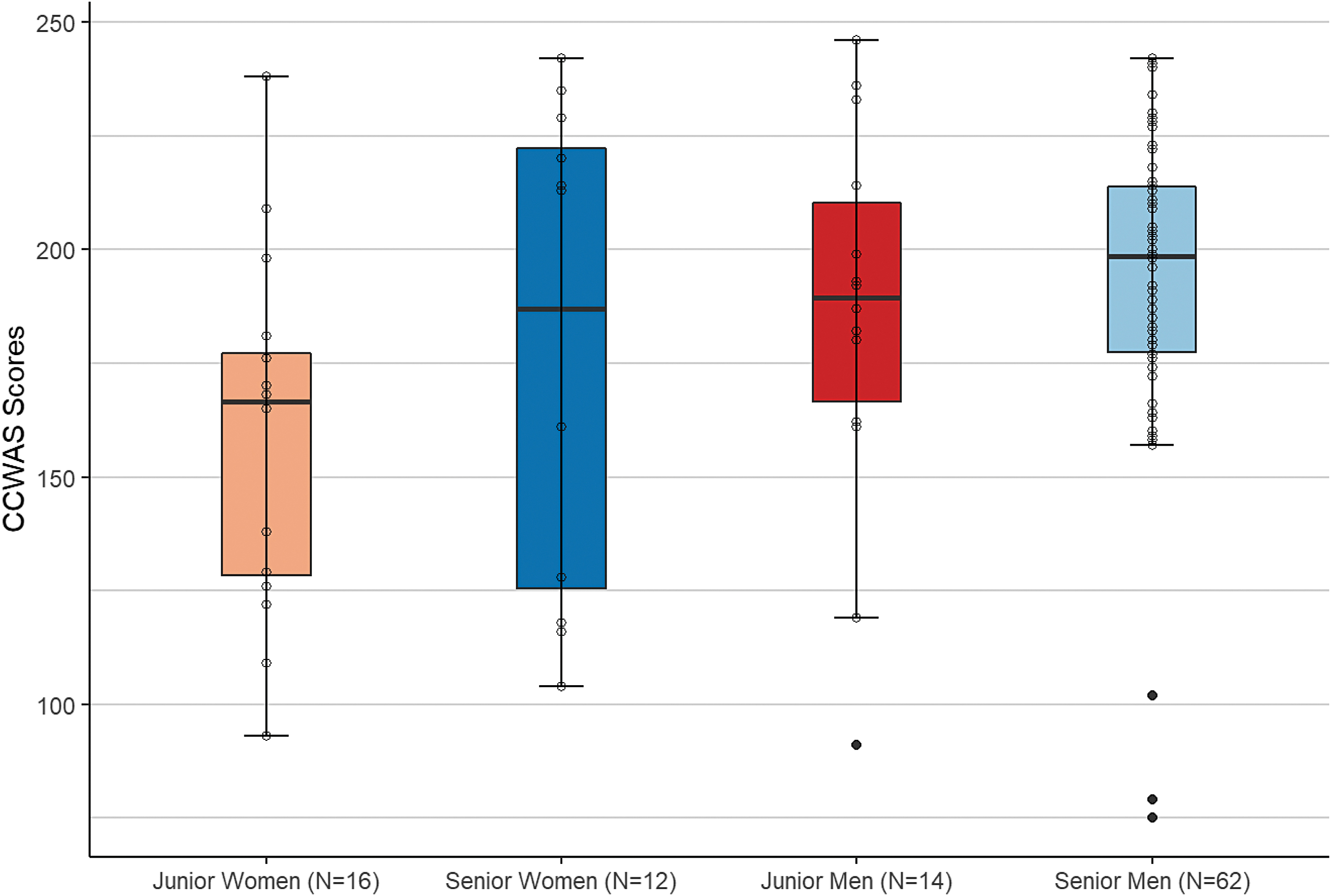
Median CCWAS score of respondents by years in practice and gender. Junior was defined as <5–10 years' experience; Senior was defined as >10 years' experience. CCWAS = Culture Conducive to Women's Academic Success. Color graphics are available online.
Results
Of 1492 surveys sent to the Endourological Society listserve, 104 (7%) completed responses were received. It is unknown how many of the members of the listserve are actively practicing and active within the Endourological Society. Of completed responses, 26.9% were female. Of the 500 members in the United States that the survey was sent to, 59 responded, and the remaining respondents were of an international constituency. Demographic information of all 104 completed survey participants is included in Table 1.
Demographic Descriptive Statistics and Culture Conducive to Women's Academic Success Score
CCWAS = Culture Conducive to Women's Academic Success; IQR = interquartile range.
There was a statistically significant difference between male and female respondents regarding the perception of the institutional culture toward women. The male median CCWAS score was 196.0 (interquartile range [IQR] 189.0–228.0) vs female median CCWAS score of 166.5 (IQR 127.5–210.0; p < 0.05). Higher CCWAS scores suggest that respondents perceive a work culture favorable to women. These results indicate that male respondents perceive the work culture to be more favorable to their female colleagues (Fig. 2).

Distribution of CCWAS scores by gender. Color graphics are available online.
Respondents without children perceived a significantly less favorable work culture for women than those with children (median [IQR] 196.0 [174.0–214.5] vs 172.0 [128.75–193.75]; p < 0.05).
Kruskal–Wallis test was used to compare the CCWAS scores between demographic groups and subcategory questions. There was no statistically significant difference in CCWAS scores based on years in practice (Fig. 3), academic vs private practice, or location (Table 2). Questions related to the subcategory “equal access” showed discrepancy between males and females (p < 0.05), indicating that male endourologists perceived their female colleagues to have equal access to career development, however, female respondents CCWAS score showed that they did not agree.
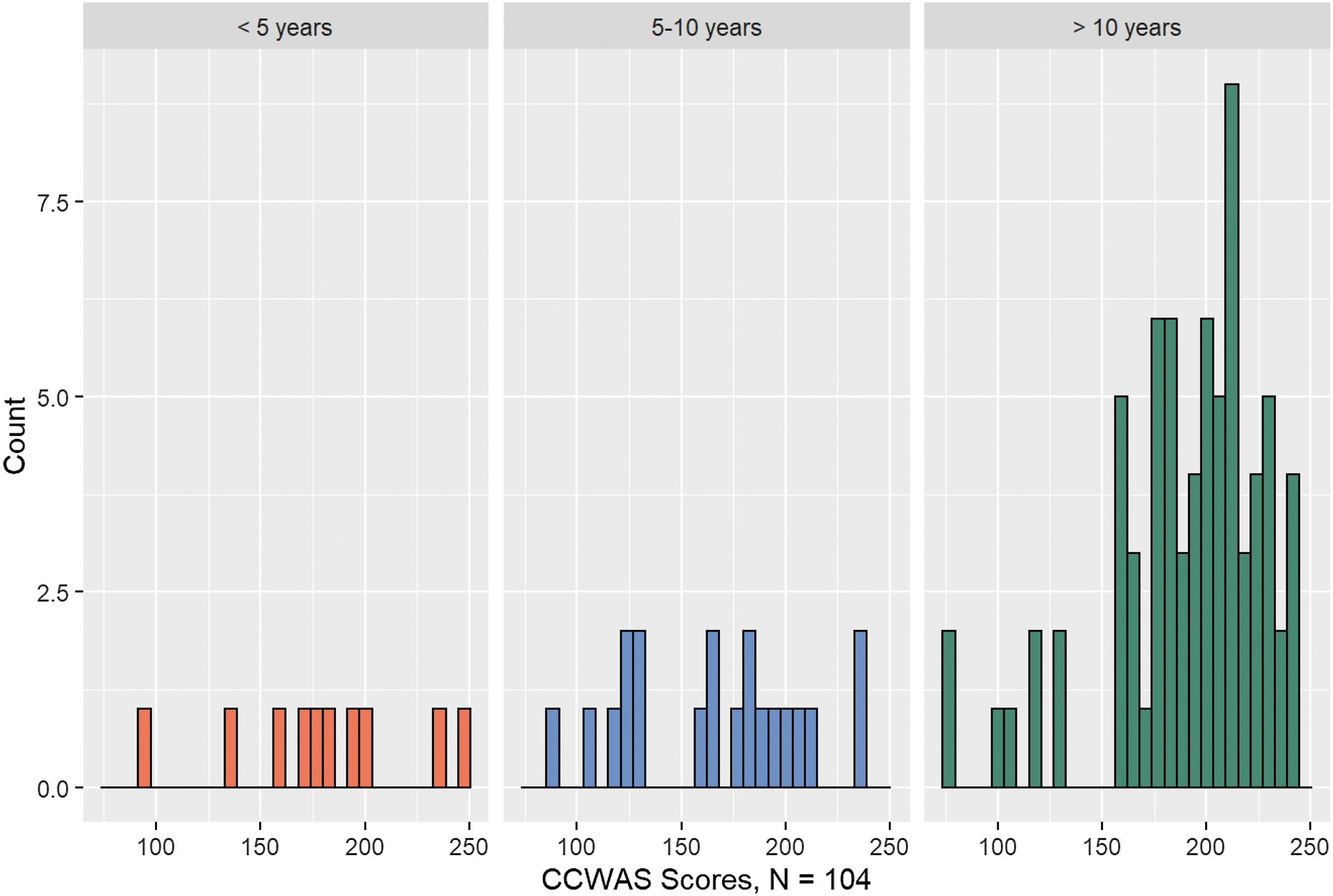
Distribution of CCWAS scores by years in practice. Color graphics are available online.
Kruskal–Wallis Test Results of Culture Conducive to Women's Academic Success Domain Scores by Demographic Domains: Equal Access, Work Life Balance, Freedom from Gender Bias, and Leadership Support
Denotes inexact p-value because of rank-sum tie. Exact Wilcoxon/Kruskal-Wallace tests were performed as one subsample was less than 50 in each analysis. For all the analysis performed, a p value less than 0.05 is considered statistically significant.
Equal access CCWAS scores varied depending on number of years in practice, with respondents with greater than 10 years' experience having the highest median CCWAS score, followed by <5 years of practice, and the lowest CCWAS score was in those with 5–10 years of experience (median [IQR] 80.0 [68.0–87.0] vs 70.0 [65–72.75] vs 63.0 [50.0–74.0]; p < 0.05). This indicates that those in the middle of their career perceive the culture for women to be worse than those at stages earlier or later in their careers. There was no difference between departmental status and location.
The perception of “work-life balance” domain again showed higher CCWAS scores from male respondents in comparison with their female counterparts (p < 0.05). In the domain evaluating freedom from gender bias, female respondents had lower CCWAS scores in comparison to male respondents (p < 0.05). Leadership support aligned with that of previous domains showing statistically significant differences between male and female CCWAS scores (p < 0.05).
At the conclusion of the survey, there were two free response questions posed to respondents. One asked: “Are there any programs or interventions that you would like to see within Endourology to improve gender equity?” Twenty-eight males responded, 11 of which said no programming is necessary, 3 said that equity had already been addressed in their department, 2 requested active recruitment of female urologists, and 3 requested educational programs regarding microaggressions and gender biases. Another male noted “too many already.” Ten females responded, two of which said no programming is necessary, two requested leadership changes that included women, and two indicated a need for external reviews. Responses are shared in Table 3.
Free Text Responses to “Are there any programs or Interventions That You Would Want to See Within Your Department to Improve Gender Equity?”
The second question invited respondents to share any comments with the study team, including barriers to gender equity that have been experienced, anecdotes, stories, comments, and/or concerns (Table 4). Twenty-one males responded. Four of these male respondents felt that women and men were equal in their practice. One male respondent felt that minorities had advantages over white, male colleagues. Twelve females responded, with nine of them reporting harmful microaggressions and biases that they had experienced.
Free Text Responses to “Leave Information for the Study Team Regarding Gender Equity, Including Barriers, Experience, Anecdotes, Stories, Comments, and/or Concerns”
Discussion
This study found a disconnect regarding perceptions of gender equity between male and female endourologists who answered this survey, with males perceiving a more advantageous/equitable work environment for their female counterparts. This disparity of perception was preserved across all subcategories measured, including equal access, work-life balance, freedom from gender bias, and supportive leadership. These results support the hypothesis that the perception of an organization's culture may differ from that of lived experience. Similar results were found in the internal medicine study previously mentioned and in our prior study surveying the Society of Pediatric Urologists. 11 Ruzycki et al, hypothesized that this discrepancy could explain the lack of action when it comes to correcting disparities within the medical field. 9
Our survey included an option for free-text comments from respondents. Female respondents hoped for transparency, education, and leadership opportunities (Table 3). These comments reflect recent studies regarding the gender pay gap, female urologists' workload, and leadership progression. 6 –8 Female gender has been shown as a significant predictor of lower compensation, even when controlling for work hours, call frequency, age, fellowship training, practice setting, and type. 6 Adjusted salaries among female urologists were $76,321 less than that of their male counterparts. 6 A recent study by North et al, found that while men and women work equal hours women urologists were more likely to work in less profitable settings, perform fewer inpatient procedures, and see fewer patients. 7
While some argue that this is related to productivity, a recent study by Mayer et al reviewed the publication productivity of academic urologists in the United States by gender and found that there was no difference in research productivity by successive rank when controlling for career duration. 12 In a multivariable analysis, gender remained a significant predictor of lower compensation after controlling for age, practice setting and type, fellowship training, call frequency, work hours, employment of midlevel providers, and ancillary income. 6
It is known that female urologists are more likely to have completed fellowship training, with Female Pelvic Medicine and Reconstructive Surgery and Pediatric Urology being the two most popular subspecialties for women urologists. 1 Nettey et al studied gender representation in urologic subspecialties and found that male urologists were 1.3 times more likely to identify as endourologists than their female colleagues. 13 AUA data from 2018 support these findings showing low numbers of women reporting endourology fellowships. Interestingly, even though women are more likely than men to subspecialize and practice in an academic setting, they are less likely to ascend to leadership positions in urology. 1 A survey of academic urology programs in 2016 noted that women comprised 3.3% of chairs, 4.5% of vice chairs, 7.9% of division directors, 9.4% of fellowship directors, 8.1% of residency directors, and 27.4% of medical student clerkship directors. 8
The Endourological Society is the only society with female representation on their executive board, while all other urologic societies and professional organizations had at least one woman in other leadership positions (e.g., officers and members at large). Leadership opportunities are an important factor for career progression. A comment from a survey respondent recounts lack of leadership advancement for female colleagues within her department and the paternalistic justifications given for continually promoting junior male faculty (Table 3). This is reflected in our results as mid-career endourologists (5–10 years) perceive a worse culture for women in comparison to more senior (>10 years) or junior (<5 years) urologists.
Mid-career urologists are affected at a greater proportion when it comes to lack of sponsorship and promotion than junior colleagues entering the workforce. Those more senior endourologists may perceive a better culture for women endourologist possibly due to being largely male-dominated and/or being in positions of power.
With regard to work-life balance, it has been found that urology has one of the highest burnout rates of any specialty. 14 The lack of time for personal/family life while working was listed as a top reason for early retirement. 5 Comments from respondents echo a need for resources to support those with children (Table 3). Those with children at home perceived the work culture to be less advantageous for females in comparison to those without children. This may reflect the continued cultural belief that women are responsible for childcare. This idea is reiterated by a comment from a female respondent stating that most male faculty members in their department had partners who stayed at home with their children (Table 3). The 2018 AUA census data reported 60.4% of practices offered paid maternity leave, and 28% of practices paid paternity leave. 5
Informal and unconscious bias could be a factor perpetuating the difference in perceptions of the work environment between male and female urologists. Respondents to our survey noted “receiving emails asking female urologists to wear dresses to the annual department photo” and “being asked to write emails in a nicer tone or use smiley face images as to not come off as too aggressive” (Table 4). It is possible that some male urologists are unaware that their female colleagues receive comments such as these, or that they cause offense. Some urologists may view instructions to dress in a certain gender normative way or use specific language in emails as harmless; however, these subtle nuances preserve and transmit the informal cultural biases. Continually enduring these biases can feel collectively repressing and amplify the marginalization or isolating of women from their male colleagues.
There are limitations in this study. We received a low response rate for this survey. It is not clear how many of the 1500 people are active members of the endourologic society, which could skew our response rate. This survey was sent to a large international contingent, and only English language surveys were utilized. Previous meta-analysis of internet survey response rates shows a wide variability of response rates to internet-based surveys, and in 2000, the average was 39.6% with a large standard deviation of 19.6%, and in 2007, this decreased to 32.7%. 15,16 A recent review focused on internet surveys of physicians showed that a response rate <20% is not uncommon. 17
Physicians have a low response rate for internet-based surveys with a study showing similar response rates of 9%, of emailed surveys, even with incentives. 18 This could be due to the overwhelming amount of email received by individuals, which aligns with the decline in internet survey responses since their inception in the late 1980s. 19 This study was sent via email and took ∼10 minutes to complete, which limits responses to those who had the time and access to email during the survey response window. Language, given this was largely an international list, could have been a barrier as well. Those with stronger opinions may have felt more inclined to respond, potentially creating bias. These limitations while important to note should not detract from the important issue that this survey addresses.
This survey was sent through the Endourology Society listserv, and operated within the rules of the Society with regard to distribution, number of email blasts, and time between email blasts. Despite the low response rate, the number of responses is equivalent to the same survey that was sent out to other urologic specialty committees (Society of Urology Oncology, Society of Pediatric Urology, Society of Urodynamics, Female Pelvic Medicine and Urogenital Surgery). 11 A brief literature review of surveys conducted via the Endourological Society published in the Journal of Endourology over the last 10 years identified numerous studies with similar number of respondents and/or response rates. 20 –23 Survey studies are inherently biased with both response and nonresponse biases.
The authors conclude that this low rate is partially a result of a less curated listserve. In addition, the higher percentage of women responses may speak to the knowledge that this workforce has about gender equity and how pervasive this issue is within Endourology. These findings provide a foundation for further study. The nonresponse of this study demonstrates a need to further discuss this important topic. Equally, it is important to publish these results as to not silence the responders' experiences, while fully disclosing the inherent limitations of the study.
The survey was designed to specifically assess gender equity in the academic setting, and therefore may not be as applicable to the private practice setting. However, we felt it imperative to include the private practice data in this study, as many urologists work in the private sector and their experiences are significant.
At the time of this study, the Endourological Society did not collect gender or demographic data, and we are therefore unable to comment on how our sample's population correlates with the general population of this organization. The lack of demographic data is a significant limitation, and an actionable item for the society to work on. Currently, however, the Endourological Society is actively performing a census so that demographic data can be more easily included in future studies, which will enable researchers to better track progress of diversity and inclusion within the Society. This study is also limited to the field of endourology. Studies investigating and comparing the perceptions of gender equity across various urologic societies is of future interest.
While survey results may not be completely representative of all Endourology members, these results demonstrate female respondents perceive a less equitable environment for women within their field, indicating an opportunity for improvement.
Conclusion
This study suggests that there are significant differences in the perception of gender equity between male and female endourologists who responded to the survey. These data show that male endourologists perceive an environment that is equitable for women in the field. However, female responses indicate a less favorable working culture. This knowledge will hopefully be a conduit to more notable interventions and help to identify opportunities to improve gender equity within endourology.
Footnotes
Authors' Contributions
The authors confirm contributions to the article as follows: study conception and design: L.H.M., R.E.H., S.L.B., and C.A.S.; data collection: L.H.M., R.E.H., S.L.B., and C.A.S.; analysis and interpretation of results: L.H.M., R.E.H., R.A., and C.A.S.; draft article preparation: L.H.M., R.E.H., S.L.B., M.J.S., R.A., and C.A.S. All authors reviewed the results and approved the final version of the article.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.