
Abstract
Introduction:
The creation of synthetic reservoirs for bladder replacement has been limited by challenges of interfacing synthetic materials and native tissue. We sought to overcome this challenge by utilizing a novel bilayer silk fibroin scaffold (BLSF) as an intermediary toward the development of an acellular prosthetic reservoir.
Methods:
Under institutionally approved protocols, 3D-printed reservoirs were implanted in six juvenile female pigs after cystectomy. BLSF was attached to the in situ prosthetic reservoir serving as an intermediary to native ureteral and urethral tissue anastomoses. Our first protocol allowed four pigs to be survived up to 7 days, and the second protocol allowed two pigs to be survived for up to 1 year. At the first sign of functional decline or the end of the study period, the animals were euthanized, and kidneys, ureters, prosthetic bladder, and urethra were harvested en bloc for histopathology analysis.
Results:
The first two pigs had anastomotic urine leaks because of design flaws resulting in early termination. The third pig had acute renal failure resulting in early termination. The artificial bladder design was modified in subsequent iterations. The fourth pig survived for 7 days and, upon autopsy, had intact urethral and ureteral anastomoses. The fifth and sixth pigs survived for 11 and 12 weeks, respectively, before they were sacrificed because of failure to thrive. One animal developed an enteric fistula. The other animal had an intact anastomosis, and the BLFS was identified at the ureteral and urethral anastomoses on histopathologic analysis.
Conclusions:
Replacing the porcine bladder with a prosthetic bladder was achieved for up to 3 months, the second longest survival period for a nonbiologic bladder alternative. BLSF was used for the first time to create an interface between synthetic material and biologic tissue by allowing ingrowth of urothelium onto the acellular alloplastic bladder.
Introduction
Bladder cancer is the sixth most common malignancy in the United States, accounting for 4.6% of all new cancer diagnoses in 2019. Bladder cancer affects men 2 to 3 times more often than women and is thought to be because of increased exposure to carcinogens such as tobacco and industrial chemicals. 1 The incidence of bladder cancer has significantly increased in developed countries, specifically those with a high human development index. As the economies of developing countries improve and their populations age, the rate of bladder cancer will likely increase. 2
Although the majority of patients present with superficial bladder tumors, ∼30% present with muscle invasive bladder cancer, whereas another 15% will progress to invasive disease during the period after their initial tumor diagnosis. 3 Radical cystectomy with urinary diversion is the standard of care for patients with localized muscle-invasive bladder cancer or high-risk Bacillus Calmette-Guerin (BCG) unresponsive non-muscle-invasive bladder cancer. 4 Simple cystectomy is also utilized in intractable benign bladder diseases. According to the National Cancer Database and the American Cancer Society, a total of 21,105 cystectomies were performed for bladder malignancy from 2015 to 2017. 5
Both radical and simple cystectomy with urinary diversion are complex procedures, owing to the simultaneous manipulation of the urinary and gastrointestinal tracts. Nearly 58% of cystectomy patients present with complications within the first three postoperative months. 6,7 Furthermore, the 5-year postcystectomy survival rate is only 68%. The high rate of complications is most attributed to the reconstruction of the bladder. 8 Long-term complications (e.g., stomal complications, recurrent infections, renal failure, ureterointestinal anastomotic strictures, and metabolic disorders) further diminish the quality and longevity of a patient's life and result in increased cost to the health care system. 9
Since the first radical cystectomy in 1887 by Bardenheuer, there has been an ongoing effort to improve and innovate with respect to bladder reconstruction and replacement. The differences between gastrointestinal mucosa and urothelium, especially with respect to the types of solutes they absorb, present an unalterable challenge. 10 To date, bladder transplantation has not been entertained or attempted. Alternatively, synthetic prosthetic models of the bladder have been constructed for the past 50 years; these have consisted mostly of silicone. 6,11,12
Most efforts were trialed in dogs and sheep and the longest duration implant was the Lutzeyer sheep model that had ∼50% success at 7 months. 12 Challenges to these approaches include infection, encrustation, hydroureteronephrosis, and biocompatibility. 11 –21 The benefit of a truly prosthetic bladder would be the replacement of a complex bowel reconstruction with a simple prosthesis implantation with only three, or possibly two (vida infra), anastomoses. The development of this alternative could lead to major reductions in cost, complications, and patient rehabilitation.
A major limitation of prior bladder prostheses has been the interface between the prosthesis and native tissue. Prior studies have noted intraluminal ureteral papillomas at the uretero-prosthetic junction (Stern model). 21 We sought to overcome this issue by using a novel bilayer silk fibroin scaffold (BLFS), which has recently shown promise for tissue regeneration and incorporation within the urinary tract. 22,23
Herein, we report an in vivo series of six porcine cystectomies with implantation of a 3D printed synthetic bladder designed to serve as an adynamic drainable cistern rather than a dynamic structure that would store and empty (i.e., contract).
Methods
Creation of a prosthetic bladder reservoir
Over the course of two decades, four versions of a prosthetic bladder reservoir were created with each change derived from the preceding experiment. The initial titanium bladder was produced as a “joke” by Mr. Richard Ewers, an engineer formally at Applied Urology, Inc., upon the suggestion of one of the authors (R.V.C.) in 1999 (Fig. 1). The subsequent 3D printed models were designed using a computer-aided design (CAD) file that was created using SolidWorks software (Dassault Systemes Solidworks Corporation, Waltham, MA). The second, third, and fourth versions were designed on CATIA V5 (Dassault Systemes Solidworks Corporation).

Artificial bladder version 1. Volume 230 mL (Designed by Richard Ewers in 1999).
The final 3D rendering of each allopathic bladder design was then imported into PrusaSlicer (Prusa Research, Prague, Czech Republic), which generated the code necessary to properly print the parts. In PrusaSlicer, the bladders were set to have a layer height of 0.15 mm with an infill of 15%. The reservoirs were printed such that the internal supports pointed vertically and a support structure, from the underside of the bladder to the printer surface, was included for a more stable print. The bladder was printed using an Original Prusa i3 MK3 machine (Prusa Research) with silver polylactic acid (PLA) material. Figure 2 depicts the second version of the artificial bladder.
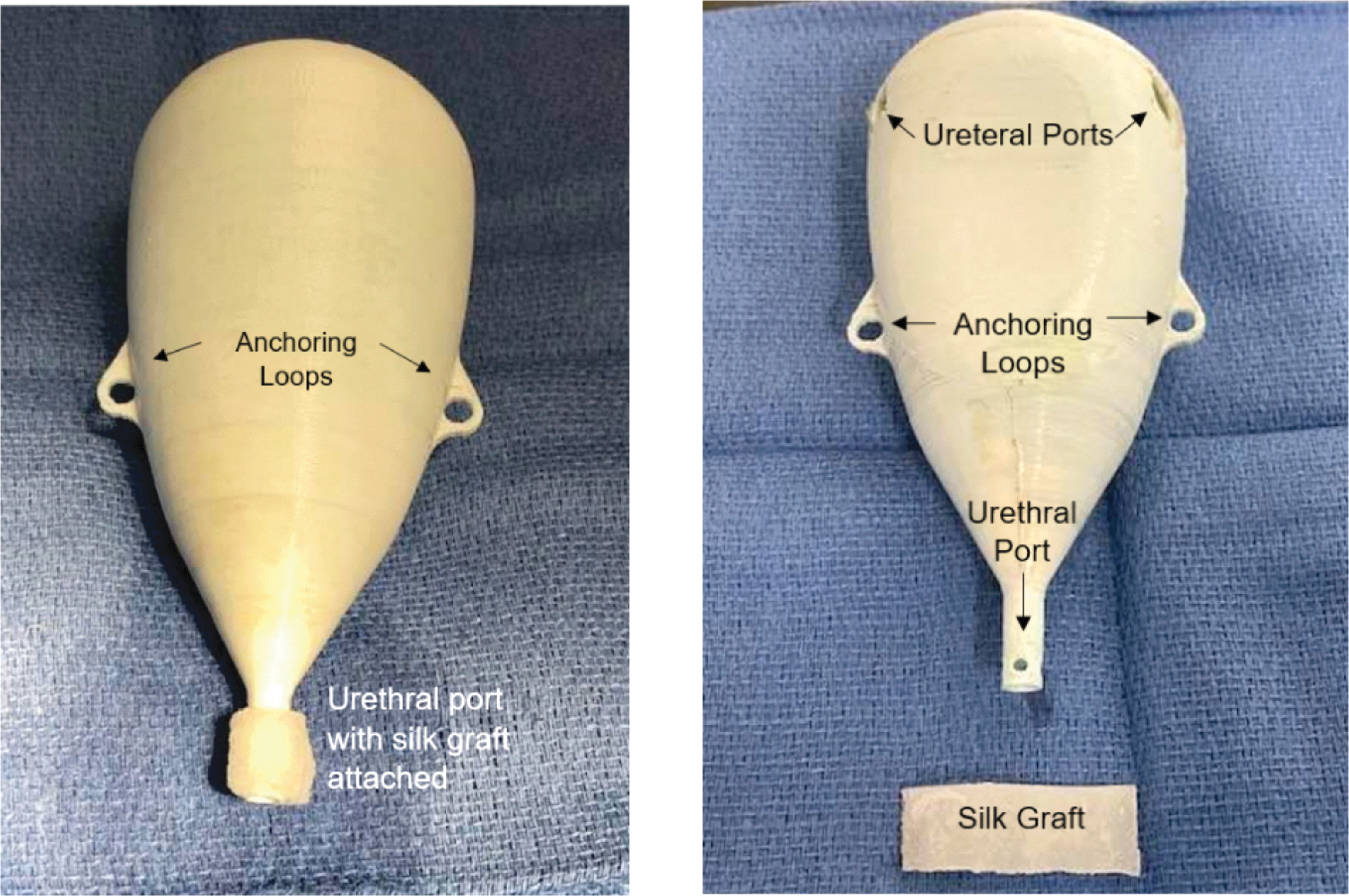
Artificial bladder version 2. Volume 160 mL. Reservoir was anchored to the anterior abdominal wall through anchoring loops. Silk scaffold was applied to urethral port. Also, silk scaffolds were tubularized to provide a “tunnel” through which the ureters were passed.
This reservoir had an ellipsoid/conical shape with a volume of 160 mL. Figure 3 depicts the third version of the artificial bladder, a flask-shaped reservoir with a volume of 170 mL, which was made flatter to better accommodate the suprapubic space. Figure 4 depicts the fourth version of the bladder, a heart-shaped flask reservoir with a volume of 52 mL and thicker walls of 3 mm (20 × thicker than the prior models) designed to facilitate a single Wallace ureteral anastomosis and to resist potential fragmentation of the reservoir itself. These prosthetic bladder iterations were implanted into six juvenile female pigs under two Institutional Animal Care and Use Committee (IACUC)-approved protocols. Pig 1 received artificial bladder version 1, pig 2 received version 2, pigs 3 and 4 received version 3, and pigs 5 and 6 received version 4.
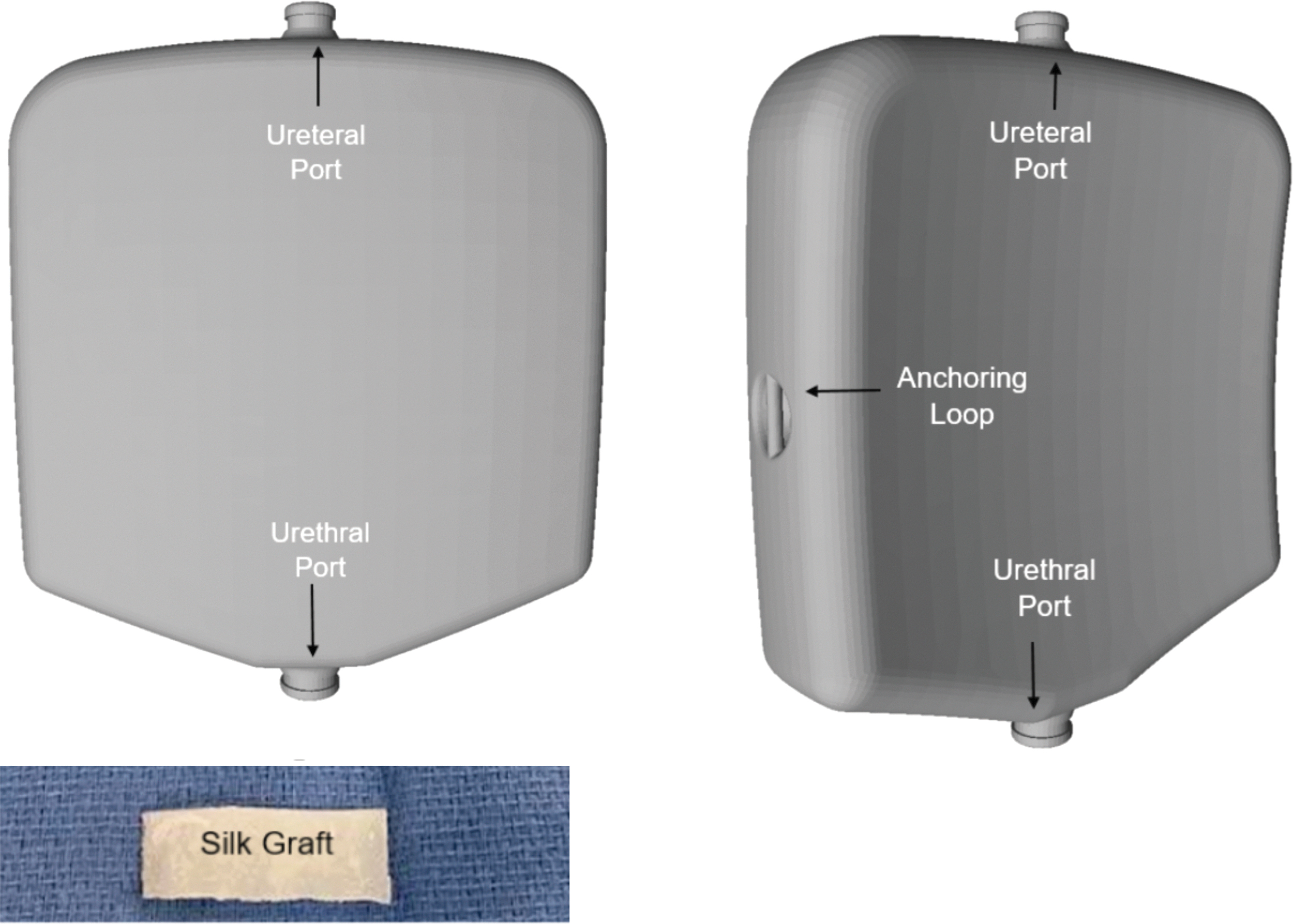
Artificial bladder version 3. Volume 170 mL. Silk graft applied around both the ureteral and urethral ports. Reservoir anchored to the anterior abdominal wall through anchoring loops.

Artificial bladder version 4. Volume 52 mL.
Silk scaffolds
The BLFS was fabricated from aqueous silk fibroin solutions by using a previously described solvent-casting and salt leaching process with silk fibroin film casting combinations. 24 The silk scaffolds were then tubularized to serve as the intermediary between the alloplastic reservoir and the native ureters and urethra for the second through fourth version of the prosthetic bladder (Fig. 2).
Animal use protocols
Four pigs (trials 1–4) were under AUP-18-005, which mandated harvest of any implanted animal by day 7. Two pigs (trials 5–6) were under AUP-21-004, which mandated a protocol of serum chemistries and regular follow-up for 8 weeks. If the animal did not show any signs of decline, the animal would continue to live and be monitored until 1 year postoperatively or until it exceeded the weight limit of the vivarium (80 kg). If the animal showed any signs of decline during or after the 8-week follow-up period, it was euthanized, and the urinary tract tissues and the prosthetic bladder were harvested.
Anesthesia and intraoperative care
Each animal was administered a preanesthetic mixture of xylazine (2 mg/kg) and Telazol (6–8 mg/kg) intramuscularly (IM) using a 20-gauge needle. Endotracheal intubation was performed. Mechanical ventilation was performed using 1.5% to 2.5% isoflurane anesthesia and tidal volumes ranging from 350 to 500 mL. An ear vein was cannulated for intravenous fluid therapy. Throughout the surgical procedure, vital signs (heart rate, respiratory rate, end CO2, and SpO2) and muscle tone were monitored to assess the level of anesthesia. Adjustments were made in anesthetic delivery in response to changes in vital signs. Once sedated, the animal was transferred to the surgery suite and positioned in a supine position. A preoperative antibiotic (enrofloxacin 2.5 mg/kg) was administered IM. The abdomen and perineum were then prepared and draped.
Cystectomy
A midline incision was made from 2 cm above the umbilicus to the pubic symphysis. Electrocautery was used to dissect through the subcutaneous tissues to expose the anterior rectus fascia, which was then incised. The rectus muscle was split, and the posterior sheath was then incised. The peritoneal cavity was entered sharply. The pig was positioned in Trendelenburg position to allow the bowel to be packed superiorly. A Balfour self-retaining retractor was placed. The external iliac veins were identified bilaterally.
Both ureters were identified and dissected from the pelvic brim to their insertion in the bladder, being careful to preserve the surrounding adventitial tissue to prevent devascularization. The ureters were ligated at the ureterovesical junction using 0-silk ties and transected. Both ureters were left occluded to allow for hydrodistention. Next the vascular pedicles to the bladder were ligated and divided. The lateral attachments were freed with electrocautery. The urethrovesical junction was transected with electrocautery and a purse-string stitch was placed around the urethra in preparation for the subsequent anastomosis to the prosthesis. Figure 5 shows the completed cystectomy before implantation of the prosthetic bladder reservoir.
Preimplantation (cystectomy completed).
Implantation of the prosthetic bladder reservoirs
Trial 1—version 1
In the first pig, each ureter was widely spatulated. 6F stents were passed into both renal pelves. The stent's distal coils were then passed into the respective ureteral ports and then the ureters were affixed to the artificial bladder with a loop of 4-0 Vicryl. A 10F Foley catheter was inserted through the urethra into the artificial bladder. The urethral anastomosis was performed with a single loop of 4-0 Vicryl; there was no BLSF used in this initial animal. A leak test was performed through the urethral catheter noting no leakage from the three anastomoses. Estimated blood loss was 25 mL.
Trial 2—version 2
In the second pig, BLSF was glued with Dermabond onto the 3D printed reservoir at the urethral port as shown in Figure 2. BLSF washers were glued with Dermabond to the ureteral openings. Cut portions of 5F open-ended ureteral catheters were placed into each ureter up to the renal pelvis with the assistance of a 0.035″ Glidewire. The 5F catheters were then secured to the distal ureters with 5-0 Vicryl. Next both ureters were individually passed through the BLSF washers and the respective ureteral openings on the artificial bladder. The ureters were fixed to the silk washer with 5-0 Vicryl. A 10F Foley catheter was inserted through the urethra and into the artificial bladder. The urethral anastomosis was then performed between the artificial bladder's silk interface and the native urethra. A leak test was performed through the urethral catheter; no leakage of fluid was noted. Estimated blood loss was 25 mL.
Trial 3—version 2
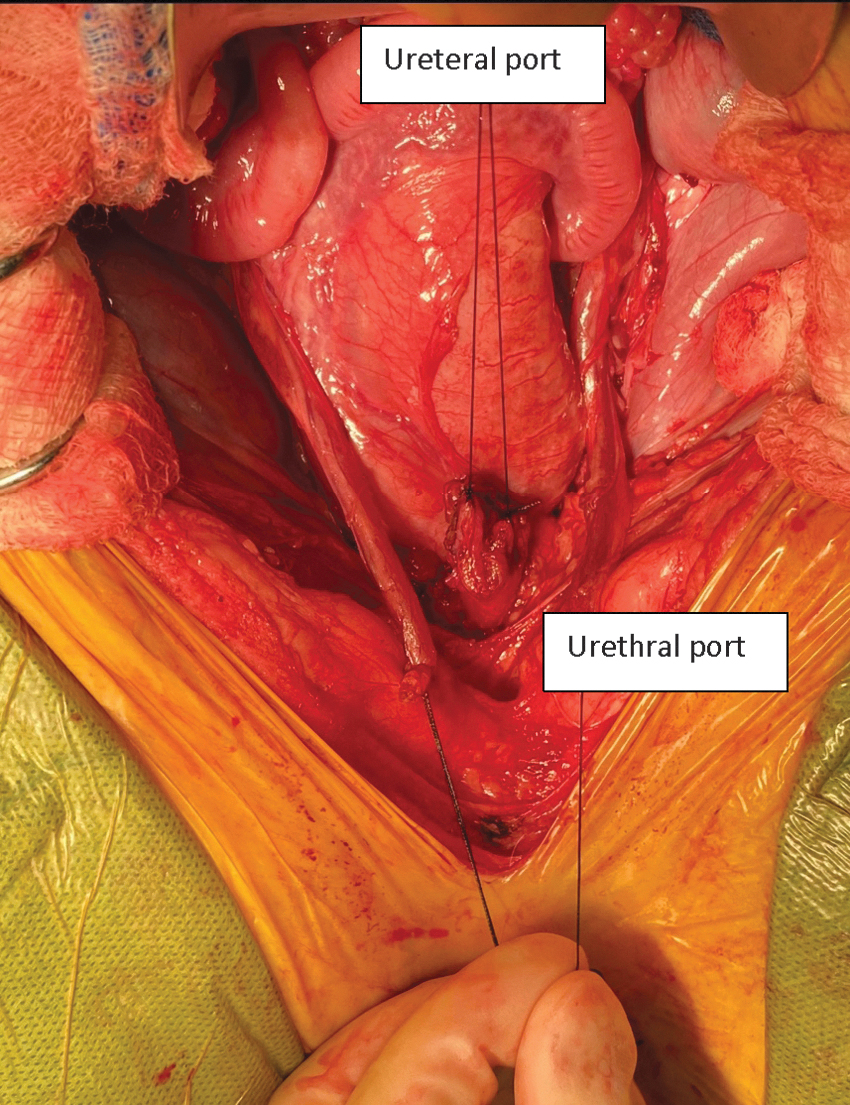
In the third pig, both ureters were widely spatulated (Fig. 2). The right ureter was passed through both ureteral openings on the reservoir and then anastomosed to the left ureter in a Wallace manner. The anastomosed ureters were then drawn back into the prosthetic bladder and the adventitia on both sides were fixed to the BLSF washer with 5-0 Vicryl. Next, a 6F × 30 cm stent was modified with additional holes cut in the middle of the stent and then each curl was passed up the ureters, with a coil formed in each kidney with assistance of a 0.035″ Glidewire. A 10F Foley catheter was inserted through the urethra into the artificial bladder. The urethral anastomosis was then performed by tying the already preplaced purse-string urethral stitch over the BLSF (Fig. 2). Figure 5 shows the implanted artificial bladder. A leak test was performed through the urethral catheter; there was no leakage. Estimated blood loss was 10 mL. Figure 6 shows the implanted bladder.

Postimplant for bladder version 2, trial 3.
Trial 4—version 3
In the fourth pig, the BLSF was glued with Dermabond onto the 3D printed reservoir at both the single ureteral and urethral ports to serve as an interface between the native tissue and prosthetic reservoir (Fig. 3). The ureters were then partially transected proximal to a silk stay suture, which was used as a handle. Using a 5 mm laparoscopic stapler (Bolder Surgical, Louisville, CO), both ureters were then pulled over the jaws of the stapler and stapled together, in a Wallace manner (Fig. 7). Two 4.7F ureteral stents were placed bilaterally into the kidney with assistance of a 0.18″ Glidewire and then passed through the solitary central ureteral port of the prosthetic bladder reservoir.
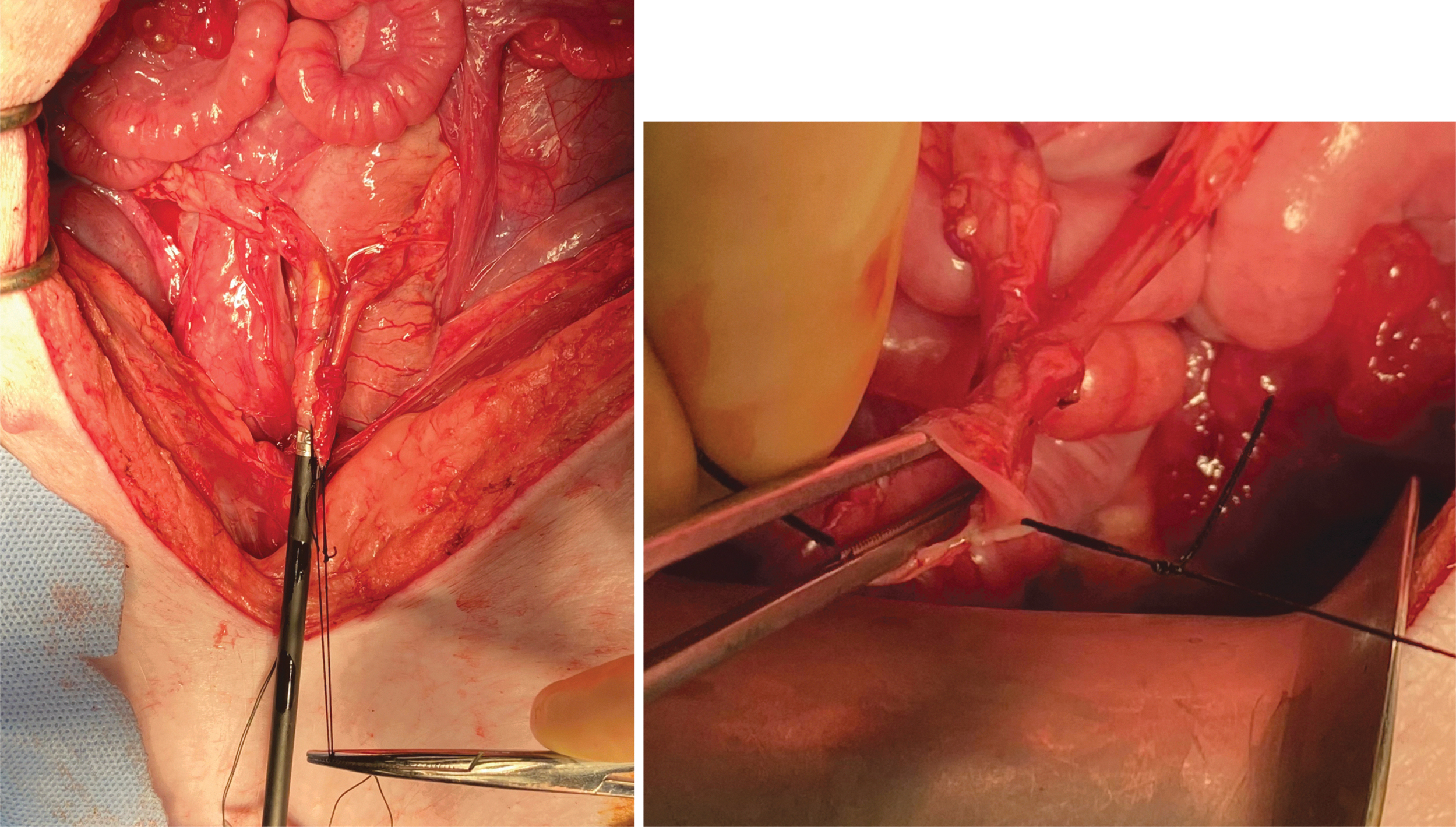
On the left, the 5 mm stapler is demonstrated. On the right, the common sheath of the stapled Wallace ureteroureteral anastomosis is shown.
The common sheath of the anastomosed ureters was then passed over the silk interface (Fig. 8). Additional interrupted sutures with 5-0 Vicryl were then placed to anastomose the conjoined ureters to the silk scaffold. A 10F Cope loop catheter was placed in the urethra and guided into the prosthetic bladder reservoir. The urethral anastomosis was then performed by securing the preplaced purse-string stitch over the urethral port and BLSF interface. A leak test was performed through the urethral catheter; there was no leakage. Estimated blood loss was 10 mL.
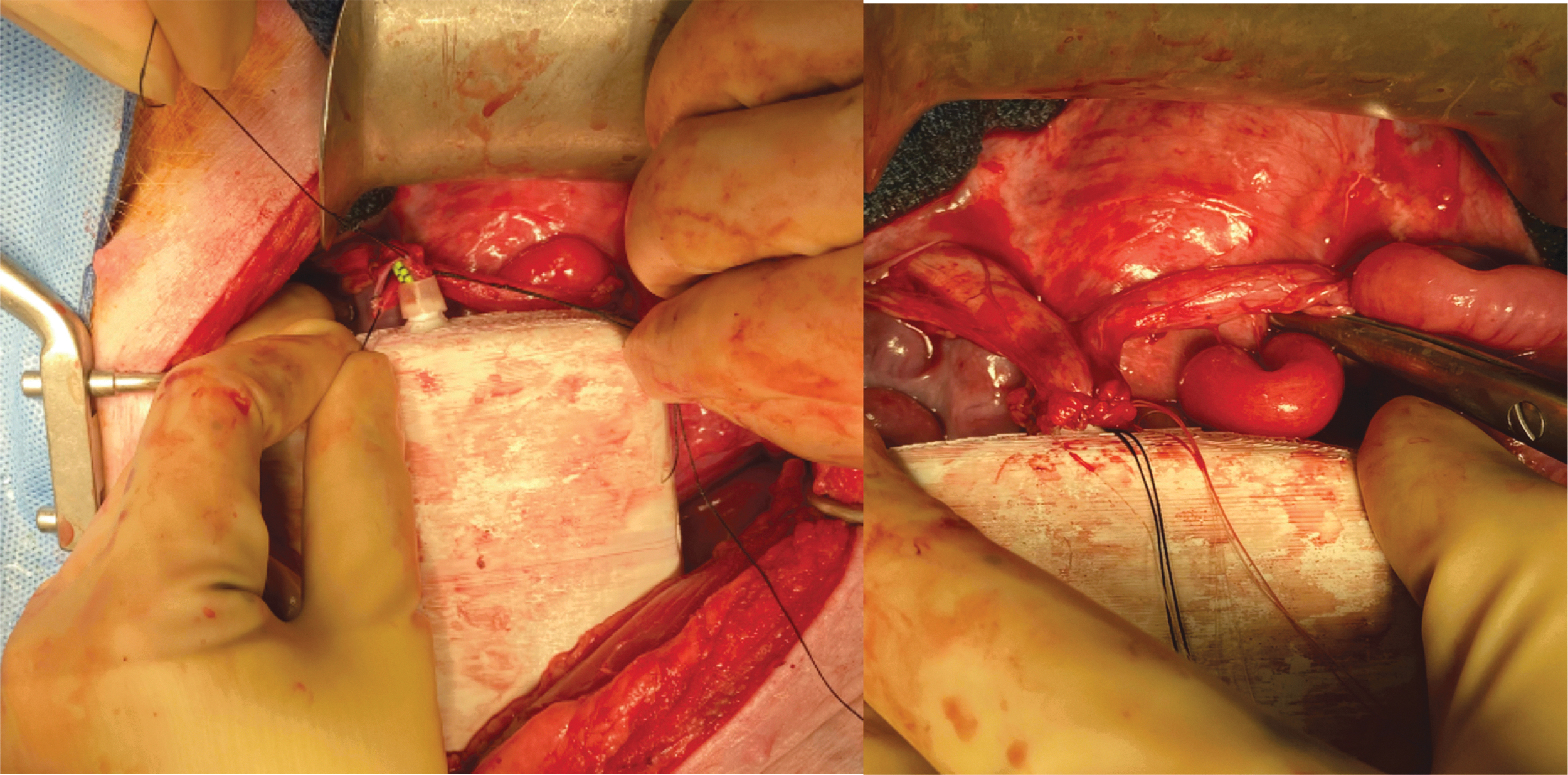
(Left) Ureteral stents were passed into the artificial bladder and up each ureter; note the preplaced sutures aid in securing the common sheath to the silk scaffold, which in turn encircles the ureteral port. (Right) Completed ureteral attachment to the prosthesis.
Trials 5 and 6—version 4
BLSF was adhered to the 3D printed reservoir at the urethral and ureteral ports with Dermabond (Fig. 4). Both ureters were sewn together in a Wallace manner before anastomosing the Wallace construct to the silk scaffold with 5-0 Vicryl (we were unable to use the prior stapler because of availability issues during the time of the experiment). Two 4.7F 20 cm ureteral stents were placed bilaterally. The urethra was anastomosed to BLSF glued onto the prosthesis using a purse-string stitch. A 10F Cope loop catheter was placed in the urethra and guided into the prosthetic bladder reservoir. Based on the earlier trial results, Seprafilm (Baxter International, Inc., Deerfield, IL) was placed posterior to the artificial reservoir to reduce the risk of adhesions. A leak test was performed through the urethral catheter; there was no leakage. Estimated blood loss was 10 mL. The implanted bladder is shown in Figure 9.
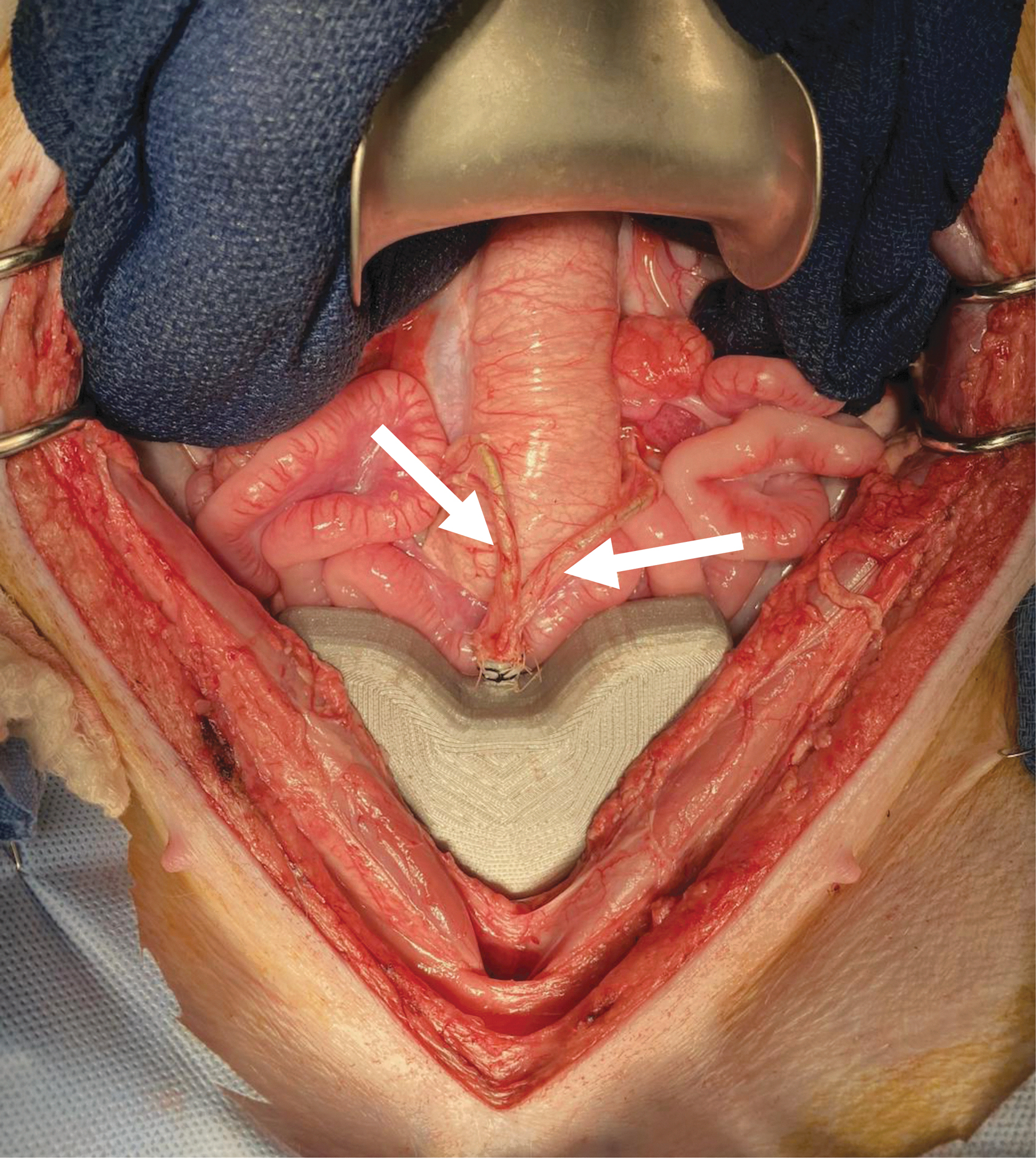
Artificial bladder version 4 as it was implanted in pigs 5 and 6. Arrows point to the ureters with stents in place.
Drain placement
For trials 1 through 3, a 7F JP drain was placed through a separate stab incision and then secured to the skin with a 2-0 Nylon suture. This was then connected to bulb suction. For trials 4 to 6, there was no drain placed because of the ease of dislodgment of the drains noted in the preceding cases.
Abdominal closure
The abdomen was irrigated with saline. The prosthesis was secured with silk sutures through the fixation ports to the anterior abdominal wall. The fascia was closed with running 0-PDS suture. The skin was closed with a skin stapler.
Postoperative care and survival period
Serum chemistries were obtained before awakening each animal. Pain was managed with buprenorphine 0.005 to 0.01 mg/kg IM every 6 to 12 hours for the first 48 hours and then every 6 to 12 hours as needed thereafter. For antimicrobial prophylaxis, Enrofloxacin (Baytril) 2.5 mg/kg IM was administered for 3 days postoperatively. Pigs 1 to 4 were observed during the mandated maximum survival period of 7 days.
Pigs 5 and 6 were performed under a separate animal use protocol, which allowed for longer survival. Postimplantation, the right and left stents were removed at 4 and 5 weeks, respectively. The pigs underwent renal ultrasonography at 2, 4, 5, 6, and then every 2 weeks. Endoscopic evaluation was performed at 4, 5, 6, and then every 2 weeks and at harvest. Serum chemistries were obtained every week for the first 4 weeks, and then every 2 weeks or more often if the pig showed signs of failure to thrive.
Euthanasia and autopsy
Eutha-6-Ethanasia solution (0.3 mg/kg) was injected into the cannulated vein. Fluoroscopic images were obtained to evaluate the position of any indwelling ureteral stent(s) and the urethral catheter. The staples were removed, and the abdomen was opened. All anastomotic sites were evaluated. A leak test was performed through the urethral catheter. The urethral catheter was removed and a flexible ureteroscope, Karl Storz Flex-XC (Karl Storz & Co. KG, Tuttlingen, Germany), was inserted into the urethra and cystoscopy of the prosthetic bladder reservoir was performed. The ureteral stents were then removed and ureteroscopy was performed to evaluate the ureteral anastomosis. The urethra, artificial bladder, and both kidneys and ureters were then harvested en bloc.
Results
Trial 1—version 1: survival <1 day
The pig was extubated and recovered after surgery. The animal was oliguric postoperatively, producing <50 mL of urine for 24 hours. The animal appeared lethargic, and the decision was made to proceed with euthanasia. On autopsy, a moderate amount of clear fluid in the peritoneum was observed. Both ureters were observed to be angled inferolaterally from the anastomosis resulting in bilateral ureteral obstruction. The urethral anastomosis was partially disrupted with resultant leakage of urine.
Trial 2—version 2: survival <1 day
The animal was extubated and recovered after surgery. The pig was found deceased on postoperative day (POD) 1. On autopsy, there was moderate amount of free fluid (∼500 mL) within the peritoneal cavity, presumably urine. Both ureteral anastomoses were intact. The urethral anastomosis was disrupted along the anterior urethra with resultant urine leak. There was marked small bowel distention.
Trial 3—version 2: survival 3 days
The animal was extubated and recovered after surgery. Postoperatively, the animal demonstrated normal activity, tolerated feeds with return of bowel function and urine output (not measured). The JP drain had minimal output in the initial postoperative period and became dislodged on POD 2. Routine serum chemistries performed on POD 3 showed a steep rise in serum blood urea nitrogen (79 mg/dL) and creatinine (18.2 mg/dL). The animal became more lethargic on POD 4 and was euthanized.
At autopsy, there was minimal intraperitoneal fluid; the creatinine level in the intraperitoneal fluid was the same as serum. A leak test was performed through the urethral catheter; there was no extravasation of fluid. Both ureteral anastomoses and the urethral anastomosis were intact (Fig. 10). No hydronephrosis was noted; however, both kidneys appeared grossly enlarged. Renal histopathology analysis revealed congested interstitial capillaries with focal interstitial hemorrhage. Upon examination of the urethra and ureters, there was no epithelialization around the silk scaffold; however, there was moderate to marked mixed acute and chronic inflammation without any foreign body giant cell reaction.

Autopsy findings for trial 3. Urethral and bilateral ureteral anastomoses are intact.
Trial 4—version 3: survival 7 days (protocol mandated euthanasia at 1 week)
The animal was extubated and recovered after surgery. Postoperative serum chemistries demonstrated a creatinine of 2.4 mg/dL, increased from a preoperative baseline of 1.1 mg/dL; serum electrolytes were within normal limits. During the postoperative period, the animal demonstrated normal activity, tolerated feeds with return of bowel function, and urine output. On POD 7, serum creatinine had declined to 1.6 mg/dL; electrolytes were within normal limits. At autopsy at 1 week, as per protocol, significant bowel adhesions were noted adjacent to the artificial bladder.
Both ureteral stents and the urethral catheter were noted to be in proper position (Fig. 11). Both the urethral and ureteral anastomoses were intact. Endoscopic evaluation of the stapled ureter and common sheath revealed healthy viable tissue (Fig. 12). A leak test was performed, noting no leakage from the anastomoses. Of note, there was a hairline crack in the posterior wall of the prosthetic bladder reservoir. This likely resulted in a urine leak, which was contained by the adhesions and accounts for the significant adhesions encountered with the mild rise in serum creatinine from baseline. Histopathology analysis showed no significant epithelialization around the silk scaffold.
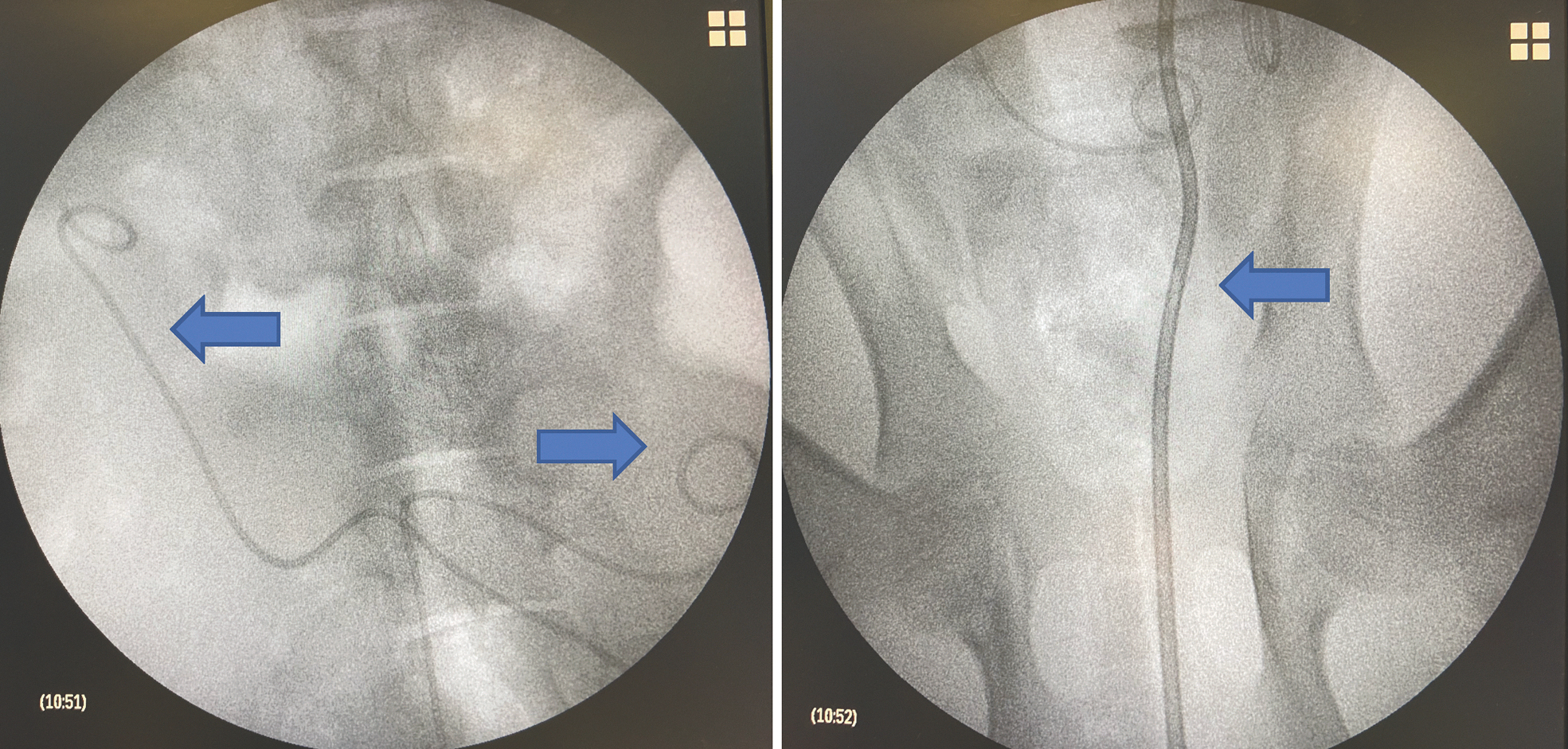
(Left image) Fluoroscopic images demonstrating appropriate position of both ureteral stents (arrows) and (right image) Cope loop urethral catheter (arrow).
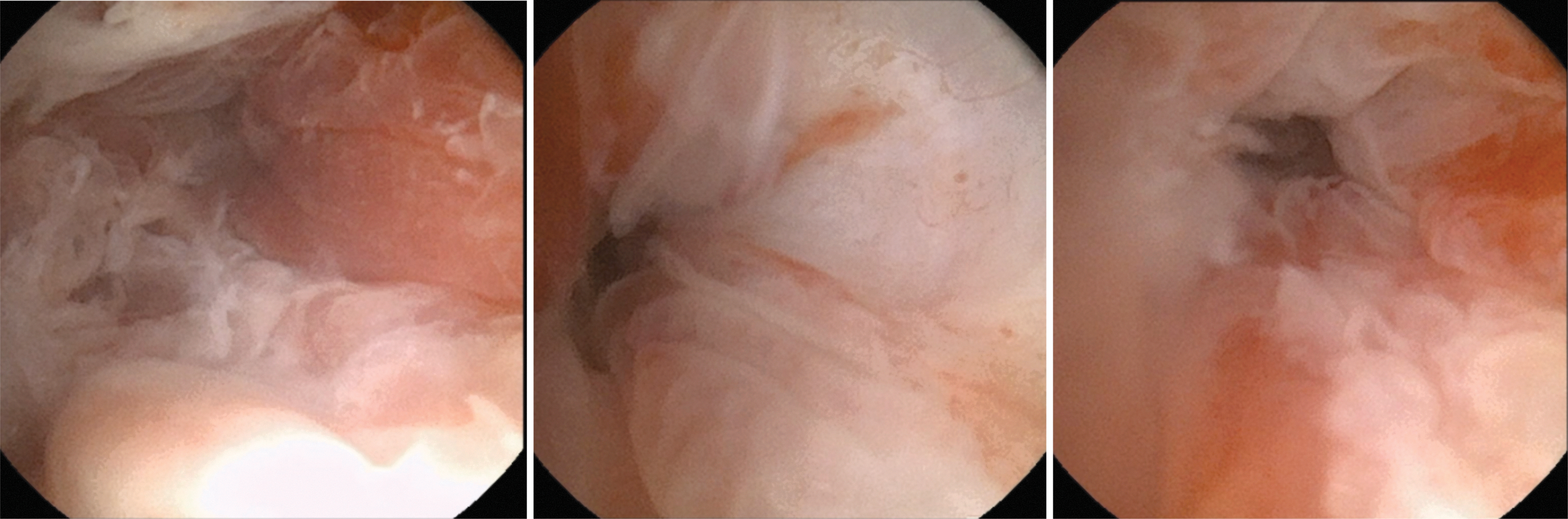
Ureteroscopic views. Left—common Wallace sheath of the anastomosed ureters (arrow points to the staple line). Middle–right ureter. Right–left ureter.
Trial 5—version 4: survival 11 weeks
The animal was extubated and recovered after surgery. POD 7 serum chemistries demonstrated a creatinine of 1.5 mg/dL, increased from a preoperative baseline of 1.3 mg/dL. The rest of serum electrolytes and blood counts were within normal limits. During the survival period, the animal had serum electrolytes and blood counts within normal limits for the first 3 weeks. There was a mild elevation of serum creatinine to 1.8 mg/dL at week 4, which then dropped to 1.5 mg/dL by week 5. On endoscopic evaluation, there were crystals and early signs of encrustation within the prosthetic bladder; at each endoscopic evaluation, crystals and loose encrustations were irrigated from the prosthetic bladder (Fig. 13).
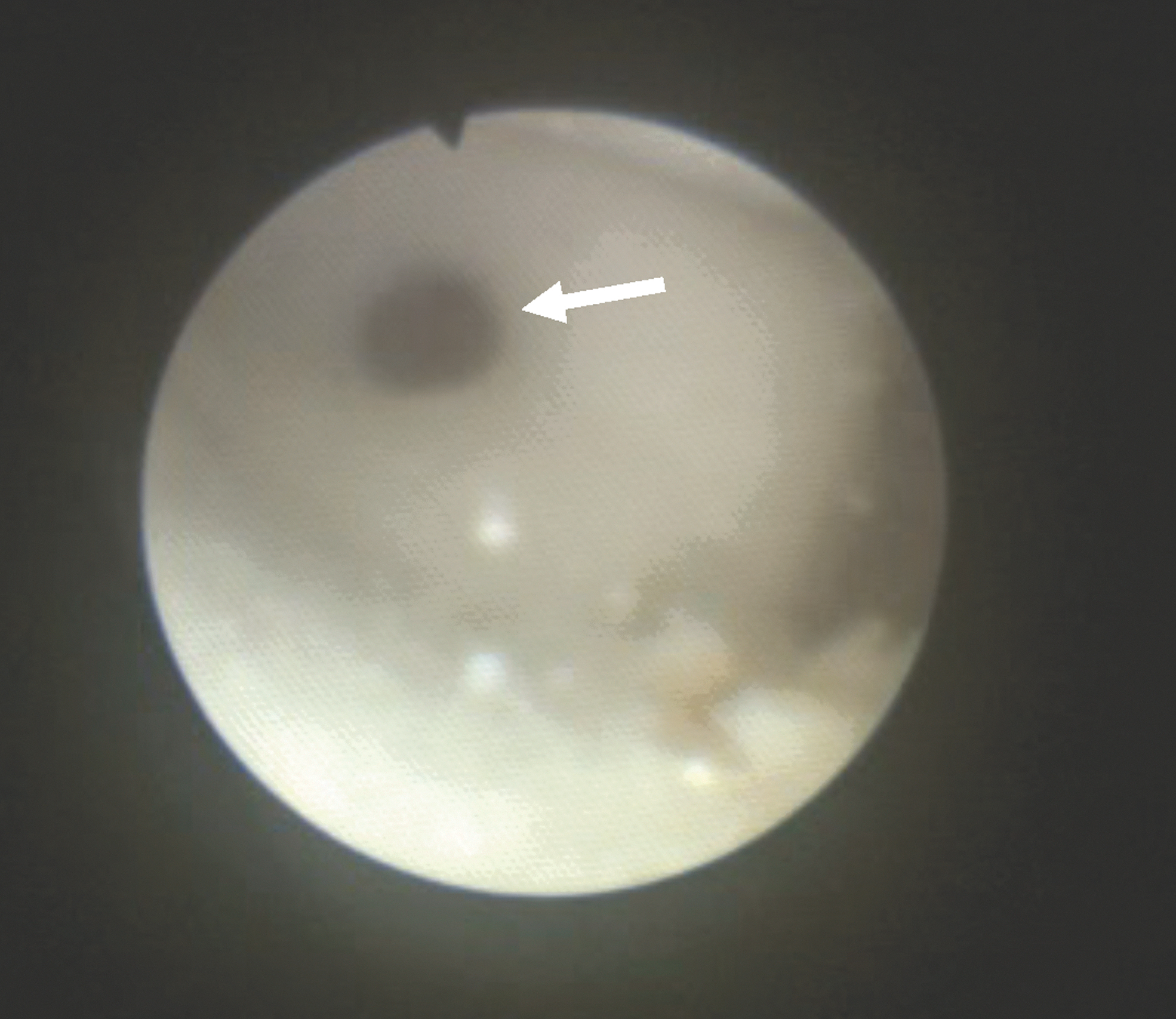
Shown is an endoscopic view with a flexible ureteroscope, which is used to perform cystoscopy. Arrow points to the ureteral opening (stents have been removed). Encrustation that developed within the lumen of the prosthetic bladder is seen layering at the bottom of the screen.
The ureteral stents were removed at weeks 4 and 5, respectively. There was no hydronephrosis on ultrasound at 2, 4, 5, 6, 8, and 10 weeks (Fig. 14). Routine endoscopic evaluation after stent removal at 6 and 8 weeks showed intact anastomoses. At week 10, the pig developed diarrhea. Serum creatinine was 1.4 mg/dL; however, the blood urea nitrogen (BUN) was elevated to >140 mg/dL. There was concern for porcine proliferative enteritis and 2.5 mL of Denagard 12.5% (tiamulin hydrogen fumarate) was given. For the subsequent week, the pig had progressive failure to thrive and was euthanized. At that time, ultrasound examination showed mild left hydronephrosis, no right hydronephrosis, and no pelvic or abdominal fluid collections.

Ultrasound comparison at 2, 5, and 6 weeks. Stable parenchymal thickness is shown.
At autopsy, there were few adhesions and no intra-abdominal fluid collection. A pseudocapsule of fibrotic tissue was noted around the implant. Of note, an enteric fistula was noted communicating with a portion of the urethra and urethral anastomosis, which is best seen on retrograde urethrogram and cystogram. In addition, the bladder was engulfed by a loop of bowel such that the prosthetic bladder had been incorporated into the bowel lumen. The ureteral anastomoses were intact and allowed for endoscopic ureteroscopy. On histopathologic analysis, the ureteral anastomotic site showed acute and chronic inflammation. The silk fibroin graft was identified along the ureteral mucosal surface at the anastomotic site. At the fistula site, there was marked acute and chronic inflammation with ulceration of the intestinal mucosa and chronic inflammation.
Trial 6—version 4. survival: 12 weeks
The animal was extubated and recovered after surgery. POD 7 serum chemistries demonstrated a creatinine of 1.4 mg/dL, a decrease from a preoperative creatinine of 1.6 mg/dL. The rest of the serum electrolytes and blood counts were within normal limits. During the survival period, the animal had serum electrolytes and blood counts within normal limits for the first 5 weeks with serum creatinine ranging from 1.4 to 1.7 mg/dL. On endoscopic evaluation, there were crystals and encrustations that progressively formed within the prosthetic bladder, which was irrigated at the time of each endoscopic evaluation. The ureteral stents were removed on weeks 4 and 5, respectively.
There was no hydronephrosis on ultrasound at 2, 4, 5, 6, 8, and 10 weeks. On week 6, the serum creatinine rose to 2.2 mg/dL. Ultrasonography did not show any abdominal fluid collections or hydronephrosis bilaterally. Routine endoscopic evaluation after stent removal at 6 and 8 weeks showed intact anastomoses. Serum creatinine decreased to 1.7 mg/dL. This pig at 11 weeks developed mild diarrhea and failed to thrive necessitating euthanasia. Before autopsy, ultrasonography showed no hydronephrosis and no pelvic or abdominal fluid collections. Serum creatinine was 2.1 mg/dL and BUN of 57 mg/dL. There was no evidence of extravasation on retrograde cystourethrography.
On endoscopic evaluation, the anastomoses at the urethra and ureters were patent and intact (Fig. 15). At autopsy, there was no abdominal fluid collection; minimal adhesions were noted. A pseudocapsule of fibrotic tissue surrounded the prosthetic bladder. The kidneys, ureters, alloplastic bladder, and urethra were harvested en bloc (Fig. 16). On histopathologic analysis, the distal ureter showed mild chronic inflammation. At the ureteral anastomosis, there was marked acute and chronic inflammation, ulceration, and granulation tissue. The silk fibroin graft was identified along the ureteral mucosal surface at the bladder anastomotic site. A representative section of urethra revealed a remnant of the BLSF scaffold deep in the fibromuscular wall with no significant inflammatory response. The silk fibroin graft was present within the urethral mucosa and along the serosal surface (Fig. 17).


Trial 6, prosthetic bladder version 4 with the explanted kidneys, ureters, and urethra en bloc.
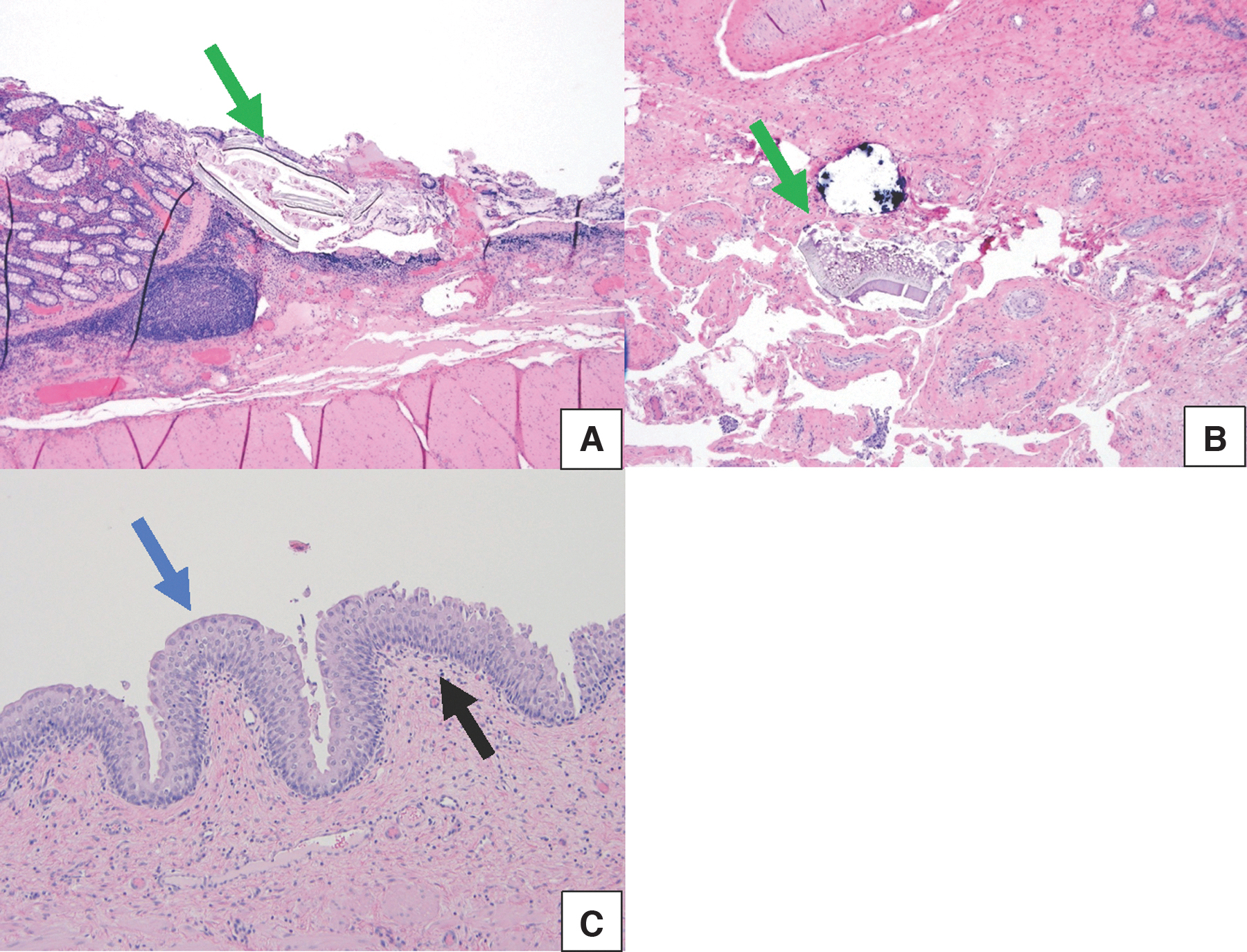
Histopathology analysis in pig 6 at 12 weeks.
Discussion
The bladder may be viewed as an organ of social convenience. Lacking exocrine or endocrine function and metabolically inactive, it largely serves as a biologic cistern with the capacity of storing and releasing urine as needed. Despite the basic simplicity of this hollow organ, it has proven quite difficult to design an effective alloplastic substitute. There are two approaches to bladder replacement: tissue based and alloplastic. Tissue engineering and cellular matrices have been explored and shown early promise. However, these efforts are plagued by the complexity of the implant as well as challenges with regard to innervation and vascularization; problems develop with regard to rupture of the implant as well as stone formation. There are also reports of early fibrosis and inadequate contractility.
This has prevented widespread clinical translation. 10 As such, we sought to proceed with the alternative alloplastic approach of developing an entirely synthetic acellular bladder. Issues that have plagued synthetic bladder replacements aside from recreating the external/internal sphincteric control and contraction mechanisms include fibrous capsule formation, encrustation, infection, anastomotic strictures, hydronephrosis, urine leakage, and biocompatibility. 25 A review of prior attempts to create an alloplastic bladder replacement highlighted that the ideal reservoir should be “totally biocompatible and impermeable, have the capacity to store a sufficient volume of urine, permit filling and voluntary voiding without any pressure repercussions on the upper urinary tract, avoid any leakage of urine, resist encrustation and infection, be simple to implant, and simple to remove/replace in the event of malfunction, and have an acceptable duration and cost.” 6
In contrast to this ideal prosthesis, our approach was a far more simplistic endeavor in keeping with our initial view of the bladder as a cistern of social convenience. As such we avoided the complexities associated with voluntary voiding, contractility, and pressure dynamics and just concentrated on creation of a biocompatible storage vessel focusing on functional ureteral and urethral anastomoses. Once this challenge was met, the next step would be to construct the prosthesis out of a noncompressible material that would resist encrustation, such as titanium. Work in that direction is currently underway in our laboratory.
In our case series, the first two pigs developed fatal urine leaks at the urethral anastomosis because of tearing of the native urethra where it was affixed to the solid protrusion of the prosthetic bladder. To overcome this problem, in the third rendition, we used a silk interface for the urethral port to allow for a more pliable anastomosis. The third trial pig survived longer but succumbed because of worsening acute kidney injury of unexplained etiology. Indeed, there was no evidence of obstruction at the ureteral or urethral anastomoses nor was there any urine leakage identified, which could have accounted for the elevated creatinine. Likewise, to date, thorough histopathologic evaluation of both kidneys failed to provide a satisfactory explanation.
Another problem with the first two versions of the bladder prosthesis was their shape. Both the spherical and conical shapes made it difficult to close the abdomen after implantation. As such, we shifted the design toward a flatter flask-shaped reservoir, which conformed better to the abdominal wall and resolved the abdominal closure problem in subsequent implants. As we worked further on the design, we realized that it was not necessary to have two separate ureteral anastomotic sites and thus in the fourth iteration we opted for a single central ureteral anastomotic site in line with the urethral site.
The single ureteral Wallace-type anastomosis was facilitated by utilizing a 5 mm laparoscopic stapler, which rapidly created a large caliber common sheath for the ureteral anastomosis. To the best of our knowledge, this is the first report of a stapled Wallace anastomosis. In this animal that survived the full 7 days of the protocol, there were no issues with leakage at either anastomotic site both of which had a silk scaffold interface between the native tissue and the prosthesis; also, there was no evidence of any encrustation forming on the staple line.
The one drawback to the reservoir was a crack that developed in the body of the prosthesis and resulted in a small amount of urine leakage, which likely contributed to the significant adhesions and reaction noted at autopsy surrounding the prosthetic bladder and ureters. This issue was addressed in version 4 of the artificial bladder by increasing the wall thickness although with a decrease in volume; there was no urine leakage or damage of this iteration of the prosthesis in either pig into which it was implanted. Unfortunately, because of a lack of availability of the stapler and staple loads at the time of trials 5 and 6, we were unable to evaluate the long-term efficacy of a stapled Wallace ureteral anastomosis.
Both the fifth and sixth animals were survived concurrently. The initial animal developed diarrhea and likely experienced a gastrointestinal bacterial overgrowth associated with Lawsonia intracellularis, which can occur in this swine species. 26 This occurred despite giving both animals Denagard (tiamulin hydrogen fumarate) upon arrival to preclude this infestation; upon consultation with the veterinarian, repeat doses were given to both animals. Unfortunately, once the diarrhea began, it could not be resolved and thus both animals entered a failure to thrive phase and were euthanized before the 1-year mark. One animal had developed an enteric fistula (animal no. 5), whereas animal 6 had intact anastomoses and no evidence of urine leak or fistula formation.
The interface between synthetic reservoirs and native tissue has presented a vexing problem in prior attempts at creating an acellular prosthetic bladder (e.g., Stern model). 21 As such, we utilized a novel silk interface to serve as the intermediary between the alloplastic anastomotic sites and the native tissue (e.g., ureters and urethra). The bilayer silk fibroin scaffold (BLSF) has previously been shown to be a favorable substance for encouraging tissue regeneration in the urinary tract. The dual structure of BLSF comprises a porous inner foam layer (pore size ∼400 μm) annealed to the nonporous silk film; this provided a urine leakproof interface between the prosthetic bladder and the ureteral and the urethral anastomoses (Fig. 2). 22
At 1 week, there was no ingrowth or deposition of urothelial cells onto the silk. However, in our longer-term trials at 11 and 12 weeks, we noted incorporation of the urothelial mucosa onto the silk, which supported our hypothesis that the silk served as an effective intermediary scaffold between the nonbiologic prosthesis and biologic tissue. The ureteral anastomoses accommodated passage of guidewires, ureteral catheters, and a ureteroscope; ureteroscopy was performed under pressurized irrigation of 100 mm Hg without issue.
In the past, synthetic bladders have been created from multiple different types of material. Prior attempts at creating an alloplastic bladder include both fixed volume rigid as well as dynamic (i.e., expanding and collapsing) models. 6 The distensible models were often composed of silicone that resulted in a reactive inflammatory response with resultant production of a thick fibrous capsule around the prosthesis, which compromised its dynamic properties. 15 In this study, we sought to create a noncompliant alloplastic reservoir and thus focused on the shape of the bladder and the urethral and ureteral anastomoses, which could then be rapidly prototyped using 3D printing with PLA. PLA has been explored in medical prosthetic applications and noted to be biocompatible and nontoxic. 25,27
We learned that despite PLA being a lightweight material easily used in 3D printing applications, that it is not an ideal material to interface with urine given the significant crystals and encrustation found in the artificial bladder lumen in both long-term animals. As such, in future iterations we intend to design a PLA scaffold bladder internally coated with titanium or create a bladder fully constructed of titanium. Titanium appears to resist encrustation when exposed to urine in the absence of intestinal mucus as documented in series of laparoscopic stapled pyeloplasty as well as stapling of the bladder cuff during a laparoscopic nephroureterectomy. 28,29 In the former, follow-up CT scans failed to show evidence of encrustation; similarly in the later circumstance, surveillance cystoscopy for multiple years showed only one patient with a <3 mm encrustation on a staple.
Our findings demonstrate that bladder replacement with a synthetic acellular reservoir in a pig is feasible and functional in a mid-term survival model. Given the ready availability of 3D printers and CAD programs, today, we can rapidly prototype and test new designs using materials that have previously been available. Accordingly, based on our experience to date, the next step will be to create a 3D printed bladder prosthesis constructed with titanium alloy, which would potentially greatly reduce or eliminate the crystal and encrustation problems noted with the PLA models. Finally, once mentally “freed” of the urethra, one can foresee the future development of a 1 L prosthesis with a one-way transumbilical valve that requires drainage only once or twice a day by the recipient.
Conclusions
After earlier failed attempts and significant design alterations, replacement of the porcine bladder with an acellular prosthetic reservoir was successively achieved for a 3-month period. 3D printing of synthetic bladders with PLA allowed for rapid prototyping. In addition, BLFS overcame the major challenge of creating a compatible interface between the prosthesis and the cellular ureter/urethra. At this time, the major hurdle remains the reduction/elimination of encrustation; this will require the use of materials unique to the urinary tract. Although this area of study remains in its nascent phase, it is our contention that an acellular prosthetic bladder will become a part of the urologic surgeon's armamentarium within the next decade.
Footnotes
Authors' Contributions
Conceptualization by P.J., R.M.P., J.L., and R.V.C. Methodology by P.J., R.M.P., J.M., J.L., and R.V.C. Formal analysis and investigation by P.J., S.N.A., R.B.A., A.P., A.B., A.S., K.L.M., G.G., S.T., and R.M.P. Writing review and editing by P.J., S.N.A., K.L.M., and R.V.C. Resources by K.L. and E.L. Supervision by J.M., J.L., and R.V.C.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This study was funded by the Department of Urology, University of California, Irvine's Curiosity and Innovation fund.