
Abstract
Percutaneous nephrolithotomy
Featured Video
https://stream.cadmore.media/player/4784ee5e-78c7-403a-bac9-28ff506aa820
Introduction
Percutaneous nephrolithotomy (PCNL) is the gold standard treatment for large renal calculus and is traditionally being done in prone position. PCNL has evolved many a fold and was originally described in supine position by Valdivia et al. 1 In this position the direction of the tract is posterior and thus preserves a low pressure in the renal pelvis, and thereby reduces the risk of fluid absorption and allows spontaneous clearance/washout of fragments by gravity-directed flow of fluid. In 2007, Galdakao-modified supine Valdivia position was described by Ibarluzea et al 2 for supine PCNL.
During the era of initial years of PCNLs, intravenous pyelography was the standard imaging modality for stone disease and current modern cross-sectional imaging techniques such as ultrasound or CT were not commonly used—thus, the surgeons who performed early PCNL did not have the knowledge of perirenal anatomy, which is readily available to the modern urologist. Valdivia Uría 1 postulated that PCNL could be performed in the supine decubitus position and using preoperative CT scans for patient evaluation, demonstrated similar outcomes and complications for PCNL performed in the supine position with potential advantages in terms of ergonomics and the administration of anesthesia.
Preoperative Preparation
The preoperative evaluation should include a detailed history, clinical examination, and routine laboratory investigations. All patients should be subjected to CT intravenous pyelography (IVU) or noncontrast-enhanced spiral CT of the urinary tract to evaluate the stone location, burden, and radiolucency. A preoperative sterile urine culture was mandatory and patients with a positive culture should be treated for 48 hours before PCNL, and the treatment continued for 7 days afterward. A second-generation cephalosporin is given as prophylaxis to patients with a sterile culture at the time of surgery, and continued for <24 hours afterward. This was in accordance with American urology association and European association of urology guidelines. 3,4
Patient Positioning
In the supine position, after administering general anesthesia, the patient is pulled down toward the edge of the surgical table and placed in standard lithotomy position. The ipsilateral side (stone-bearing side) remains straight on half of the table and the contralateral leg on the stirrup. With this, we avoid the stirrup holder bumping with our instruments, especially when trying to reach the upper calix from a lower pole access with the endoscope pushing onto the patient's body. Contralateral arm remains straight and the ipsilateral arm is placed over the patient's chest high enough to avoid obscuring the angle of C-arm of mobile fluoroscopy.
The patient is slightly rotated away from the stone-bearing side toward the contralateral side, and a tubular cushion is placed below the patient from the scapula to the gluteus. The patient is then pulled laterally toward the stone-bearing side and placed 5 cm inside the metallic edge of the table to avoid interposition with fluoroscopy imaging. Once the patient has been properly positioned and landmarks are drawn, skin prepping and draping are then carried out, a flexible cystoscope is inserted through the urethra into the bladder and the respective ureteral orifice is identified and cannulated with a guidewire, over which an open-ended ureteral catheter is placed for performing a retrograde pyelogram.
Other supine positions described in literature
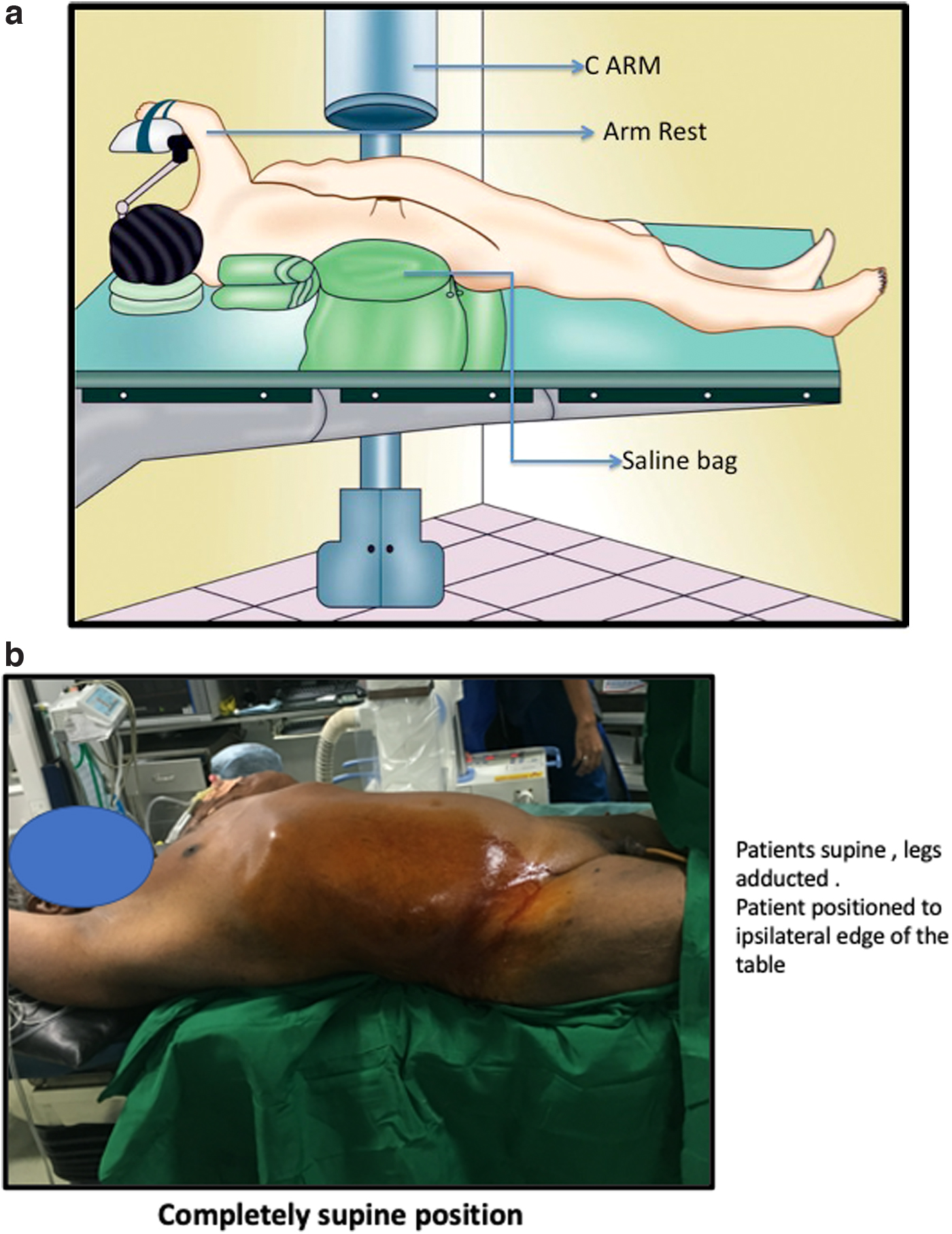
The first described supine position was that of Valdivia et al 1 with a 3-L saline bag below the flank (Fig. 1a, b). This original position does not allow for easy concurrent retrograde instrumentation and also provides limited space for choosing an access and hence has never been universally popularized.
A modification of this was the Galdakao-modified Valdivia (Fig. 2) position with again a saline bag below the flank with the legs in lithotomy, the affected side extended with the contralateral leg abducted. This allows entre to the entire urinary tract without the need for shifting position and allows simultaneous retrograde access if required. 2
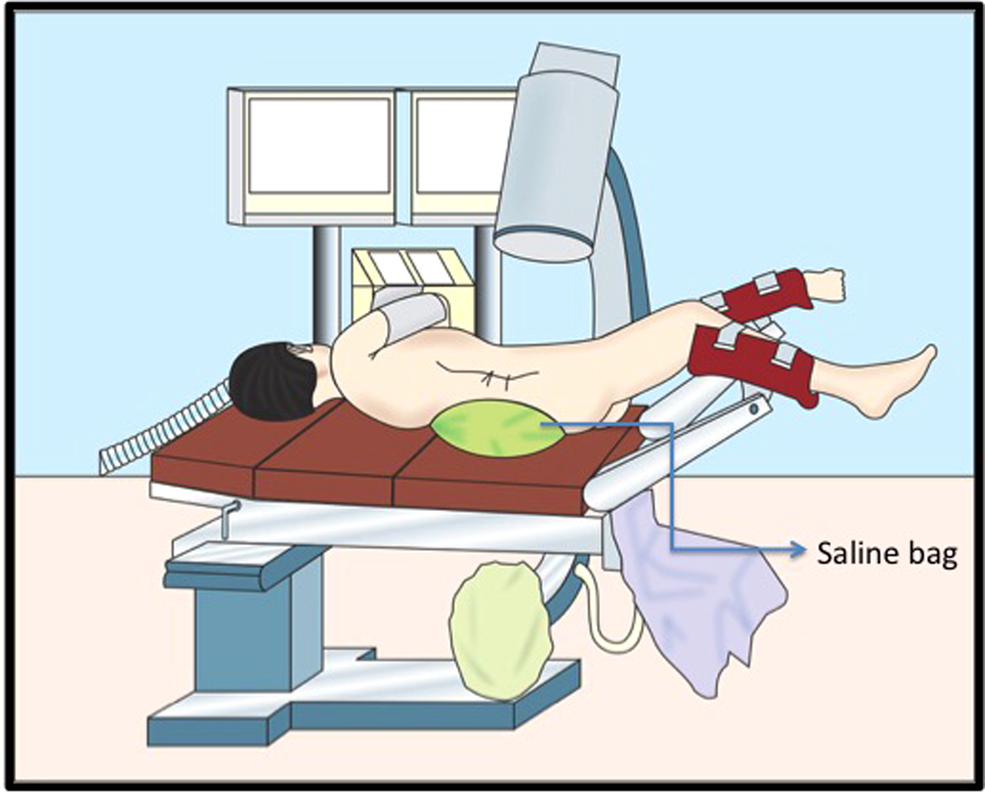
Galdakao-modified Valdivia.
The Barts modified Valdivia position (Fig. 3) offers a large surface area for access with easy manipulation of the nephroscope, as the trunk is placed at 90° to the operating table. However, renal access is not always forthright. The position results in rotation of the kidney such that the calices are viewed easily and the spine lies in the field of the collecting system. Therefore, puncture is difficult to achieve under fluoroscopy alone and often requires ultrasound localization. In this position, the kidney is hypermobile hence the puncture and guidewire manipulation is more difficult. In obese patients, supine position leads to longer tracts, which in turn leads to reduced nephroscope mobility. There is a greater torque required to manipulate the nephroscope, which can lead to damage to the renal parenchyma and increased risk of bleeding from the tract.
Barts modified Valdivia position.
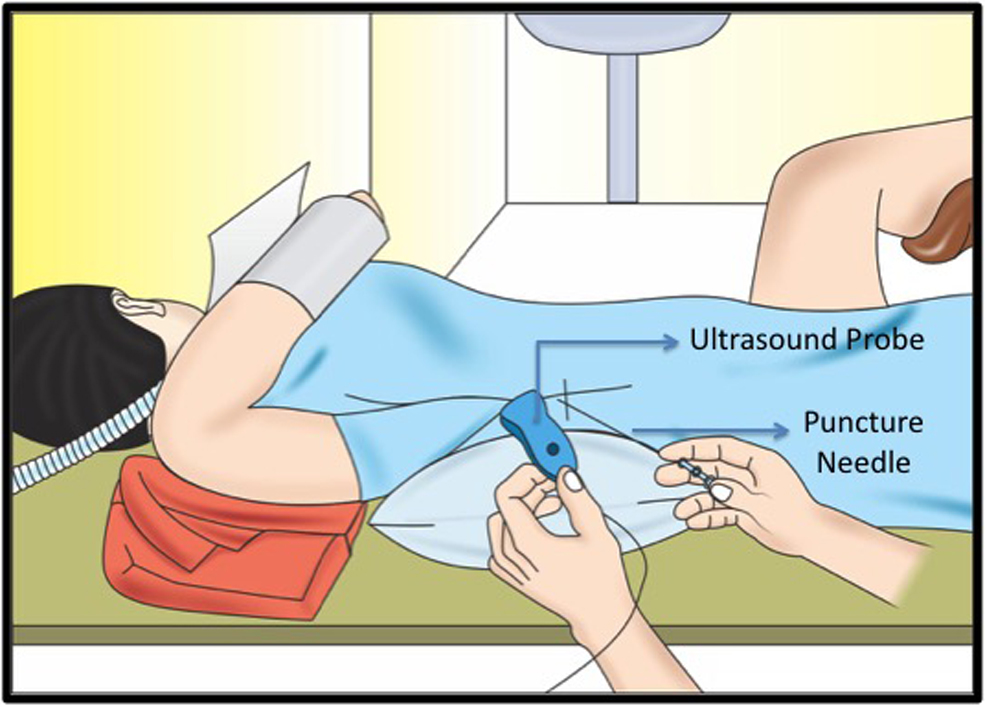
The Barts flank-free modified supine position (Fig. 4), involving a 15° tilt by using a 3-L saline bag under the ipsilateral rib cage and a small gel pad under the ipsilateral pelvis, with the ipsilateral arm brought across the chest to the contralateral side The legs are placed in lithotomy, with the ipsilateral side relatively extended and the contralateral side abducted. There is no support under the loin thus allowing more space for ideal renal access and the ability to use image-guided access with relative ease. Fluoroscopy is easier and conventional in this supine position, with the surgeon's hands being further from the operative and radiologic field.
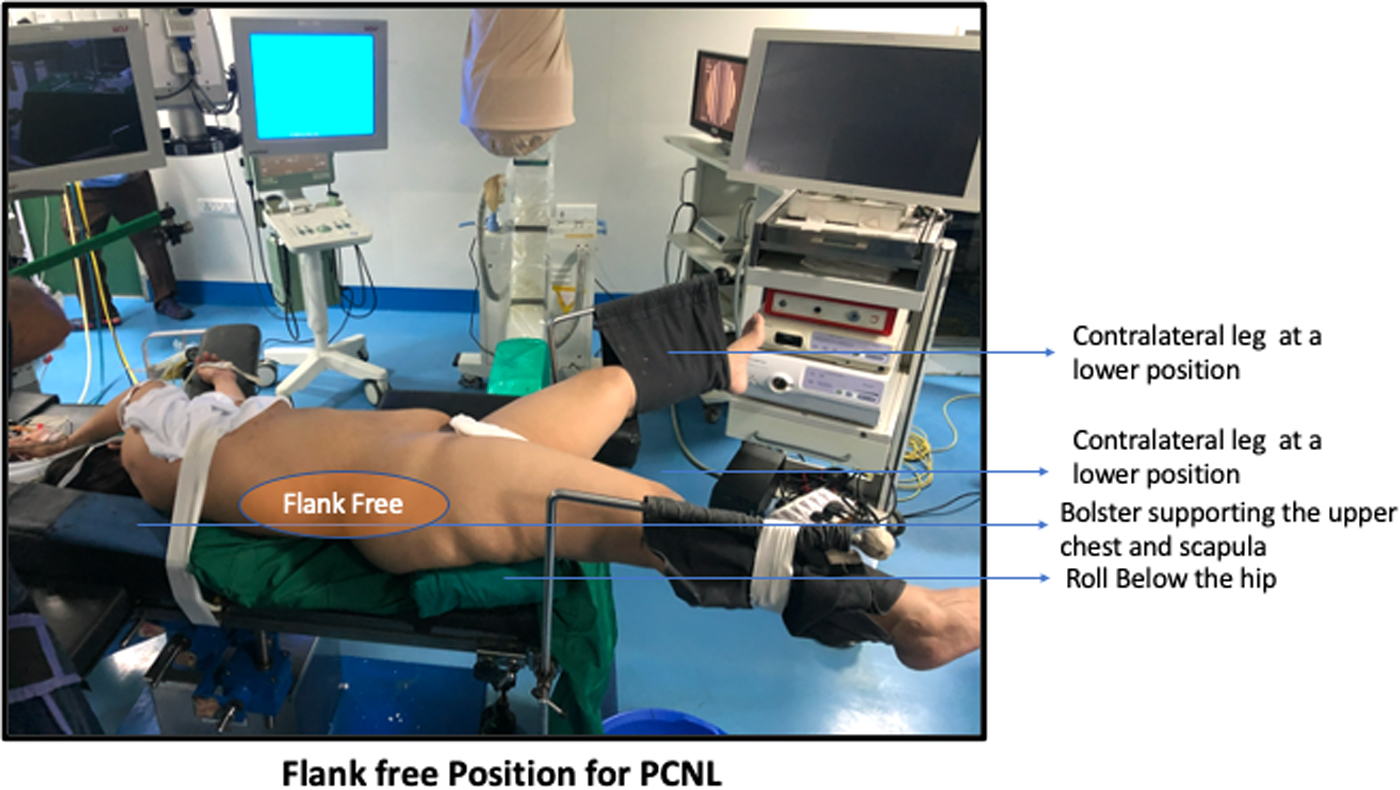
Barts flank-free position.
In addition, the kidney lies in a neutral position as compared with the semisupine positions, for example, the modified Valdivia and Barts positions and, therefore, it is less likely to displace anteriorly. The kidney is, therefore, also less mobile and puncture and dilatation are consequently easier. This supine position also offers great flexibility in planning surgery, in that primary ureteroscopy may be embarked upon in this position quite readily and then if percutaneous access is required then no further adjustment is required. However, there is a smaller operative field with the tract being fairly horizontal, even more so than the modified Valdivia, and again this facilitates lower intrarenal pressures and washout of fragments. The more horizontal angle may on occasion make the nephroscope more difficult to maneuver because of the low position of the tract with the operating table getting in the way. 5
The complete supine position allows limited space for planning renal access, as the flank is relatively poorly exposed and may result in reduced ability to maneuver the nephroscope, especially for anterior caliceal calculi. There is also no readily available retrograde access to the urinary tract and hence combined procedures are not possible. 6
Indications
-Cardiovascular compromise
-Patients requiring simultaneous PCNL and flexible ureteroscopy
-Severe kyphoscoliosis and musculoskeletal abnormalities precluding prone positioning.
Instruments Required
Mini-PCNL system by Karl Storz™ is available in two lengths: if supine position is adopted, longer access sheaths and dilators are used to overcome the longer tract faced in this position.
-IP (initial puncture) needle
-GW (guidewire)
-Screw Dilator
-Fascial Dilator
-Single-step dilators with their sheath (Storz MIP-M system, Clear Petra sheath, and Shah's sheath)
-Amplatz Dilator and sheath
-Nephroscope
-Energy source such as Lithoclast, Laser.
Surgical Steps
The procedure commences with the patient in the lithotomy position, with insertion of an open-tip 6F ureteral catheter, with a 20F cystoscope. After inserting the catheter, the patient is placed in supine with the ipsilateral arm secured to the chest, and a 3-L fluid bag under the flank. Under ultrasound/fluoroscopic guidance an 18G needle is used to puncture the collecting system. Unlike in the prone position, the needle must remain almost horizontal or slightly inclined upward toward the operating table. The puncture site was marked at the level of the posterior axillary line under the level of the 12th rib, targeting the lower posterior calices.
A guidewire is inserted, followed by dilatation of the tract using screw dilator (9F–12F) dilators up to 12F. The tract may dilated up to 30F using Alkens dilators or metallic telescopic dilators (Alken's dilators), followed by the insertion of a Amplatz sheath (24F–30F). The tract is dilated with a single-step dilator using a Storz™ MIP-M, Clear Petra™ Sheath with dilator, and Shah's™ sheath with dilator.
The increased mobility of the kidney, caused by the absence of support when supine, leads to buckling of guidewire, hindering tract dilatation. This was managed by an assistant supporting the patient's abdomen, pushing it backward during dilatation. After tract dilatation a nephroscope with appropriate energy source for stone disintegration is used.
Postoperative Care
A radiologic examination is used to assess stone clearance on the first day after surgery, with either a plain film of the abdomen or CT of the urinary tract.
Advantages of Performing Supine PCNL
Ease of administering anesthesia
No need to change position of patient
Shorter operative time
Decreased radiation exposure
Improved ergonomics of fluoroscopy
Easier endoscopic combined intrarenal surgery or simultaneous bilateral endoscopic surgery
Improved endoscopic access to the upper pole from lower pole puncture tract.
Limitations of Supine PCNL
The main limitation of this position is that the flank is not fully exposed, making IP challenging.
-Not familiar to most of urologists
-Access to posterior calix is not always possible.
-Upper calix puncture is difficult.
-Longer PCNL instruments are needed, reduced mobility of nephroscope.
-Low intrarenal pressure causes PCS collapse.
Troubleshooting
Kyphosis with staghorn calculus: in patients with kyphosis, prone position is impossible hence supine PCNL with few modifications can be adopted as described by Andika et al. 7 The position and method they used are described herewith: modified supine position (lateral 30°) and a 22F rigid cystoscope (OLYMPUS™) was used to pass ureteral catheter under fluoroscopic guidance into the renal pelvis. Right ureteral catheter inserted through right ureter-vesical junction followed by wire insertion. Percutaneous puncture in right flank (two fingers posterior to posterior axillary line) to gain access to the kidney was done. Puncture was done using 17G needle through inferior posterior calix right kidney.
Puncture then dilated using metal dilator no. 6, inner sheath no. 28, and Amplatz no. 28, a rigid nephroscope was inserted. Staghorn renal stone was found then destroyed using shock pulse (OLYMPUS) and pneumatic lithotripter (VIBROLITH™) Stone fragments were evacuated using stone forceps (STORZ). Evaluation showed no residual stone, no infundibulum laceration and active bleeding 4.7F Double-J stent (UROTECH™) was placed from antegrade. Duration of surgery was 2 hours and 45 minutes. There was 50 mL bleeding, and no intra- or postoperative complication reported.
Renal Anomalies with Calculi
In the study conducted by Osther et al, 8 they concluded that prone position is more comfortable in patients with renal anomalies. According to Rana and Bhojwani 9 static investigations such as ultrasound, IVU, or CT are mandatory with regard to the choice of position of the patient on operative table, whether supine or prone, choice of calix for puncture, and tract creation in normal kidneys. The final decision in this respect in patients with anomalous kidneys is best made during dynamic fluoroscopic views while performing retrograde urography. Pliability of the surgeon to alter the conventional PCNL technique, in anomalous kidneys, as situation demands can convert this demanding procedure into a straightforward one achieving desired results.
Clinical Outcomes
Analyzing the available literature and experience, clearly supine PCNL offers better clinical outcomes as compared with prone PCNL. The results of few studies are quoted hereunder (Table 1).
Showing Clinical Outcomes of Supine Percutaneous Nephrolithotomy in Various Series
Choudhury et al 10 in their study entitled “Supine versus prone PCNL in lower calyceal stone: Comparative study in a tertiary care center” concluded that supine PCNL has got higher rate of stone clearance as compared with prone although statistically insignificant. However, it has potential advantages for the high-risk patient especially obese patients.
Proetti et al 11 in their review observed that the balance between pros and cons clearly favors supine position for PCNL.
Take Home Message
Supine PCNL is feasible in most situations.
It is an important tool for patients who have musculoskeletal abnormalities precluding prone positioning.
It gives the surgeon a simultaneous opportunity to do flexible ureteroscopy.
Mobility of the kidney may make the puncture difficult.
Suctioning of the dust using the suction sheath in supine PCNL makes the procedure more effective.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.