
Abstract
Transurethral resection of prostate (TURP) has been the “gold standard” for surgical removal of the enlarged prostatic adenoma for many decades, and is likely to remain so despite the advent of multiple minimally invasive alternative procedures. TURP has stood the test of time, whereas the alternatives have come and gone in succession, as we have witnessed over the years. The accompanying video demonstrates the complete steps of TURP in a case of prostatic adenoma, highlighting the important nuances of the principles and the technique of resection.
Featured Video
https://stream.cadmore.media/player/9acba8a3-4dd8-4a68-a429-2fa458083ccb

Introduction
Transurethral Resection of Prostate (TURP) has been the “gold standard” for surgical removal of the enlarged prostatic adenoma for many decades, and is likely to remain so despite the advent of multiple minimally invasive alternative procedures. TURP has stood the test of time, whereas the alternatives have come and gone in succession, as we have witnessed over the years.
Indications
Indications for TURP include moderate (8–19) to severe (20–35) lower urinary tract symptoms (LUTS) not responding to medical treatment, refractory urinary retention with at least one failed attempt at catheter removal, and chronic urinary retention with back pressure changes leading to hydronephrosis and/or renal insufficiency. TURP is also indicated for the complications of benign prostatic hyperplasia, including recurrent urinary tract infection, recurrent gross hematuria, bladder diverticula, and bladder stones. 1
Preoperative Preparation
Optimization of the cardiac, renal, respiratory status, glycemic control, and general improvement of the physiologic reserves are mandatory in patients being prepared for TURP. 2 Besides a thorough general physical examination, including examination of the abdomen and external genitalia, a digital rectal examination is mandatory. Apart from the routine blood workup, serum prostate specific antigen is indicated to rule out malignancy. An ultrasound of the kidney, ureter, and bladder, and a transrectal ultrasound for prostate are required for accurately assessing prostate volume and postvoid residual urine. In patients who are voiding, uroflowmetry is required to assess the degree of outflow obstruction. A pressure-flow study (cystometrography or CMG) is indicated in case of uncertain diagnosis and suspected underlying neurologic etiology. Antibiotics should be administered in patients with evidence of infection and in patients on indwelling catheter. 1
Patient Positioning
Modified lithotomy position is the preferred position for TURP. Standard lithotomy or extended lithotomy positions should be avoided. Care should be taken to avoid overextension at the hip joint, and adequate padding support should be used for pressure points due to bony prominences 1 (Fig. 1).
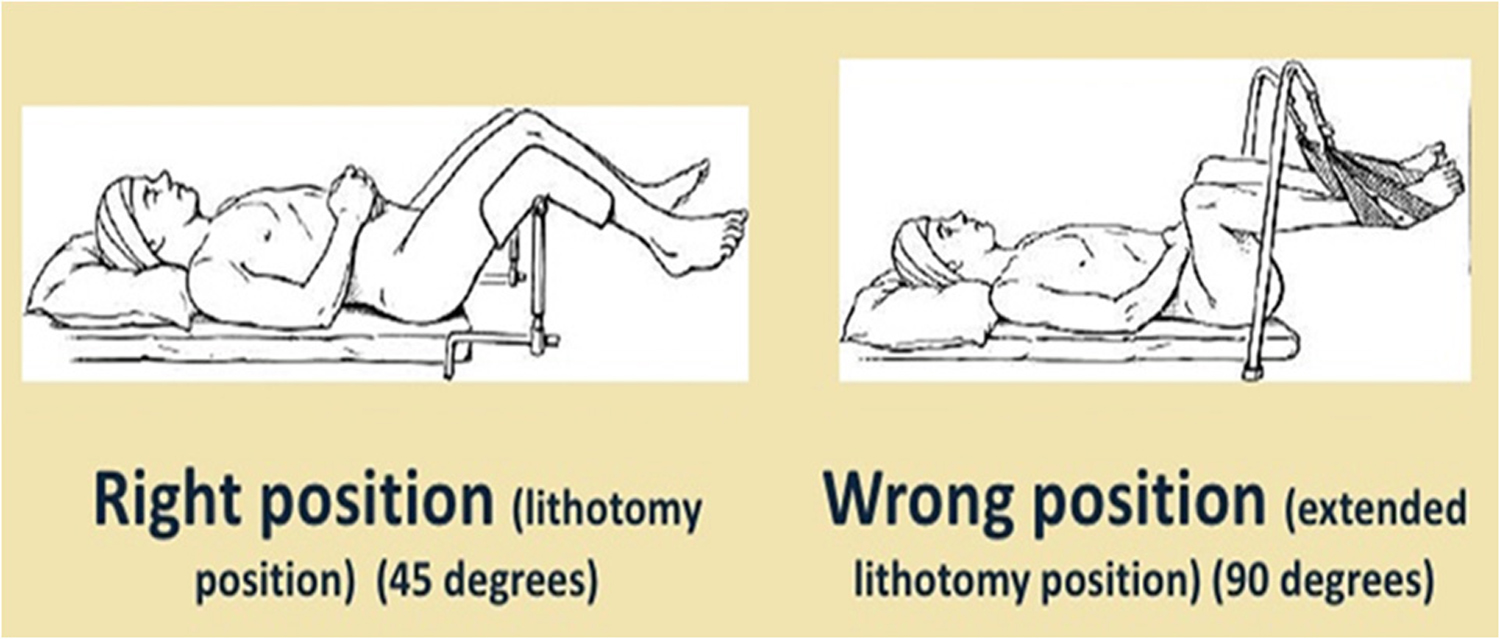
Positioning.
Surgical Steps
The procedure begins with diagnostic cystourethroscopy. If the external meatus is found to be narrow, meatotomy or meatal dilatation might be required. If the urethra is found to be narrow, urethral dilatation is done before introducing the resectoscope. In case of dense urethral stricture, a formal internal urethrotomy procedure might be required.
Several resection techniques have been defined in TURP. One of the most popular techniques is the Barnes' approach, popularized by Blandy, which involves resection from inside out (Fig. 2). An alternative approach, described by Nesbit many years ago, involves resection along the capsule, a kind of enucleation of the adenoma with the resection loop (Fig. 3). This approach merits greater attention today, in view of the current interest in endoscopic enucleation procedures for prostatic adenoma. The Nesbit procedure works around the lateral lobes along the capsule, dropping the lateral lobes one by one. The devascularized lateral lobes, which fall to the floor, are resected with relative ease at the end, along with the median lobe if present, to complete the procedure (Fig. 4).

Barnes technique of resection.
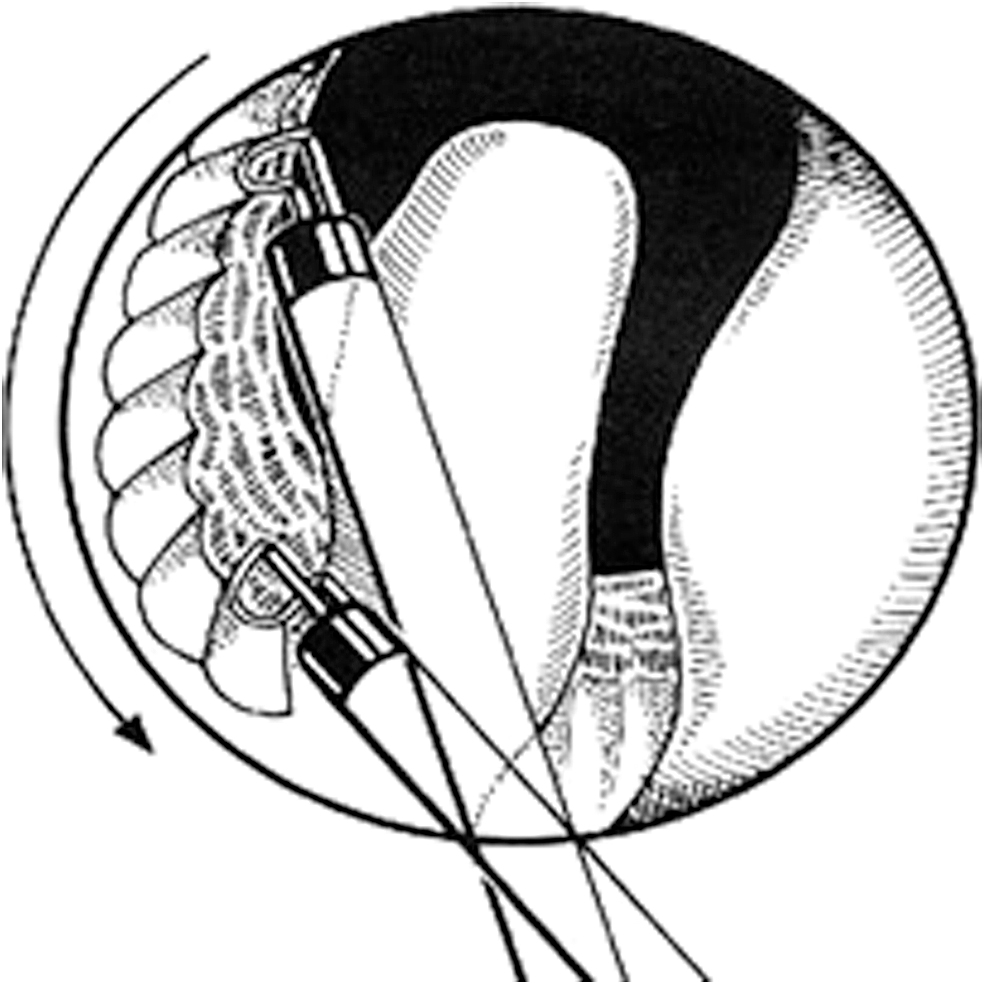
Nesbit's technique of resection.

Nesbit's procedure steps.
A 26F size resectoscope, the Iglesias continuous irrigation type, is the most frequently used equipment (Fig. 5). The resection is begun at the 12 o'clock position, the location of the anterior commissure, and progressed to a depth where circular fibers of the bladder neck and prostatic capsule become visible. The enucleation of lateral lobes is then begun one by one according to surgeon's preference. For the right lobe, the resection is carried along the capsule in an anticlockwise direction down to the 7 o'clock position (Fig. 6).
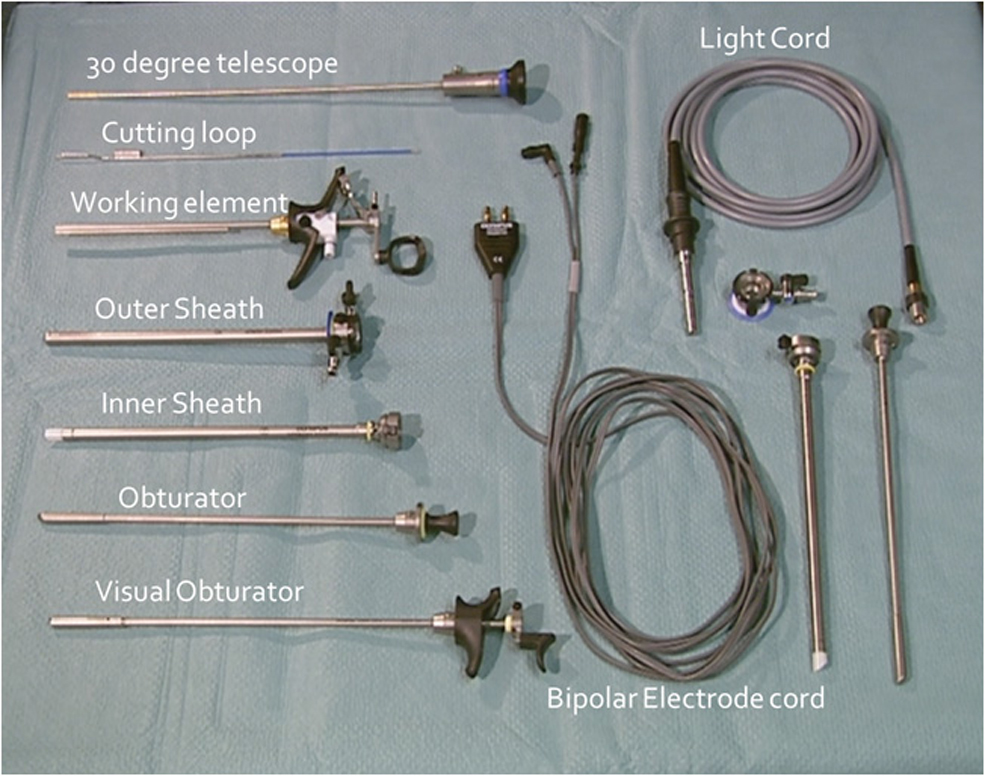
Instruments.

The resection of the prostatic tissue along the capsule results in the falling of the lateral lobe medially and toward the floor, in the process devascularizing the lobe, which now remains attached only on the floor. Once the resection of right lobe is complete, the resection of the left lobe is started again from the 12 o'clock, going down to the 5 o'clock position in a clockwise direction.
The procedure is now completed by harvesting the fallen lateral lobes between the 5 and 7 o'clock position, along with the median lobe, if present. The final part of resection can be completed relatively easily as the lateral lobes are already devascularized following separation from the capsule laterally. Deep resection should be avoided at the level of bladder neck to prevent undermining of the trigone. Finally, the resection of apical part of the prostate is completed.
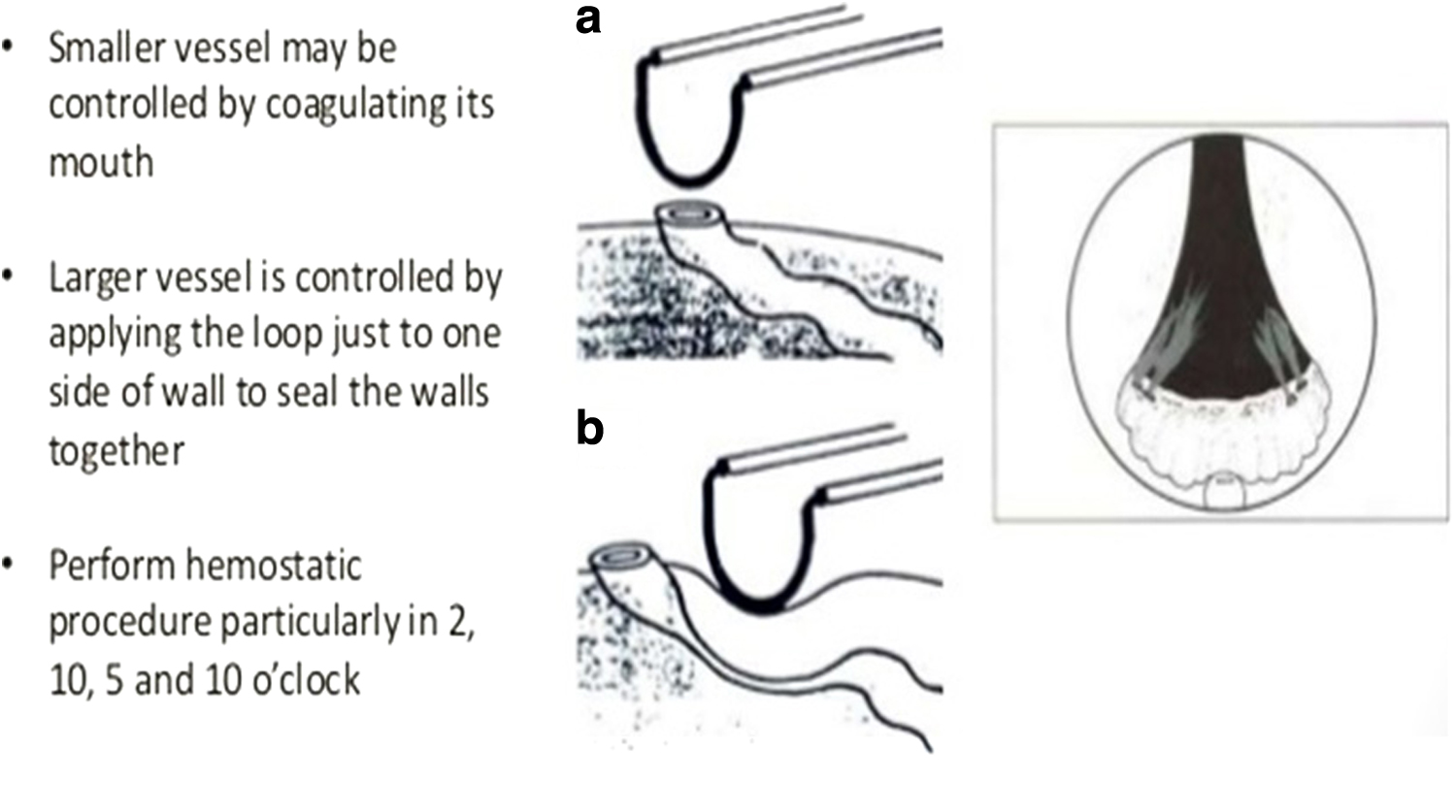
Care must be taken to avoid damage to the external sphincter. The distal extent of resection should not extend beyond the level of verumontanum in most instances, except in extremely large adenomas that extend beyond the verumontanum. The resection at the 12 o'clock position should be performed with caution as external sphincter injury is most common at this position. Hemostasis is obtained by coagulating the bleeders at the level of the capsule (Fig. 7). Once hemostasis is confirmed, evacuation of the resected tissues is performed. The procedure is concluded with the placement of a three-way Foley catheter, with gentle traction and saline irrigation (Fig. 8).

Postoperative Care
Irrigation with prewarmed saline is usually continued in the postoperative period until urine is completely clear. Traction on the Foley catheter is usually released after 2 to 4 hours unless there is persistent hematuria. Most patients are allowed oral fluids 2 hours after surgery, and made ambulatory on the first postoperative day.
High vigil should be maintained for the early recognition of the postoperative complications. Postoperative monitoring of hemoglobin, renal functions, and electrolytes is mandatory. Antibiotics are usually continued till the patient is catheter-free, and longer if there was preoperative urinary tract infection.
The patient is given a catheter-free trial after 48 to 72 hours, and discharged from the hospital after satisfactory voiding. In selected patients, a trial of voiding can be done on postoperative day 1, and the patient can be discharged on the first postoperative day as well.
Troubleshooting
TURP for large prostate glands may be associated with longer operative times and greater morbidity. The problems are mainly due to increased absorption of irrigation fluid and blood loss. Early termination of the procedure is warranted under those circumstances to minimize the morbidity. However, incomplete resection is associated with a greater incidence of reactionary and secondary hemorrhage, infection, and early recurrence. 3
“Hemiresection” of the prostate is advised in this scenario, which involves resection of one lateral lobe of the prostate along with the median lobe (if present). The efficacy of hemiresection of the prostate is comparable with that of standard TURP in patients with large prostate glands, but with the added advantage of reduced morbidity. 4
List of Instruments
Modern high-frequency electrosurgical generator, 26F resectoscope (continuous flow resectoscope, Iglesias variety), working element, Cutting loop, 30° lens, three-way Foley catheter (18F or 20F) (Fig. 5).
Alternate Techniques
TURP has been conventionally performed using monopolar electrosurgical energy. 5 However, in recent years, there has been a growing trend to replace monopolar energy with bipolar diathermy. The technique and the operative procedure of resection with bipolar technique remain the same as monopolar, with the major advantage of resection in saline instead of using glycine as irrigation fluid.
Bipolar TURP involves plasma-kinetic technology for generation of plasma around the cutting loop, which cuts through the prostatic tissue easily, and has excellent hemostatic properties. The advantage of bipolar technique is less risk of electrolyte imbalance and Trans-urethral resection-syndrome, less conductive trauma (i.e., tissue charring), better hemostasis, and a shorter catheter time. Bipolar technology has proven to be safe and effective. This approach is especially useful in cases of large adenomas.
Clinical Outcomes
The “Agency for Health Care Policy and Research” panel conducted a meta-analysis where the results of TURP were found to be significantly better than other less invasive modalities. 6 There is a steady decline in the morbidity and mortality rate of the procedure with progression of time. The mortality rate of the procedure is around 0% to 0.25%. 7 The decline in the morbidity and mortality rate is attributable improvement in the armamentarium, refinement of technique, and better teaching modalities.
Following are the results of the meta-analysis conducted by Ahyai et al 8 on the functional outcomes and complications following transurethral procedures for LUTS resulting from benign prostatic enlargement (BPE), including 23 different randomised controlled trials (RCT) with a total of 2245 patients:
Another meta-analysis done by Cornu et al 9 on the outcomes following TURP, including a total of 69 RCTs (8517 patients), found bipolar transurethral resection of prostate (B-TURP) to be associated with a lower rate of perioperative complications. Bipolar procedures were associated with a shorter catheterization time (mean difference: 17.14 minutes; p < 0.00001) and a shorter length of hospital stay (mean difference: 0.79 day; p = 0.003).
Immediate complications were also fewer in the B-TURP arms, with a significant reduction in the transfusion rate (OR: 0.49; p = 0.0009), hemoglobin drop (mean difference: 0.43; p < 0.00001), clot retention (OR: 0.47; p = 0.0002), postoperative urinary retention (OR: 0.68; p = 0.04), and reoperation rate (OR: 0.43; p = 0.02).
There was no significant difference between B-TURP and monopolar transurethral resection of prostate (M-TURP) on International prostate symptom score (IPSS), QoL score, post-void residue (PVR), and prostate volume. B-TURP procedures seemed to be associated with a higher Qmax. At the 12-month follow-up, rate of urethral stricture, bladder neck contracture, stress urinary incontinence, and the overall reoperation rate were similar following M-TURP and B-TURP.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.
Supplementary Material
Supplementary Data
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.